
Abstract
Background:
Antenatal care (ANC) is care provided to pregnant women in order to ensure positive health outcomes for both mother and baby. Late ANC contact lacks the opportunity to provide interventions that are effective early in the pregnancy. A huge proportion of pregnant women present late. The aim of this study was to identify determinants of late enrollment in the ANC among pregnant women in public health centers in Ilu Ababor Zone, South-West Ethiopia.
Design and methods:
A facility-based case-control study was conducted on 270 randomly selected pregnant women (135 cases and 135 controls). A pretested interviewer-administered questionnaire was used to collect data. Multi-variable logistic regression was run to identify the determinants of late ANC initiation. The adjusted odds ratio (AOR) and its 95% confidence interval (CI) were used to determine statistical significance at a P-value of 0.05.
Result:
A total of 270 pregnant women were interviewed, making a response rate of 97%. Unplanned pregnancy [AOR: 2.8; 95% CI: (1.3, 6.0)], lack of information on time of ANC initiation [AOR: 2.7; 95% CI:(1.02, 5.0)], older age [AOR: 2.2; 95% CI:(1.01, 4.7)], not attending ANC in the previous pregnancy [AOR: 4.07; 95% CI: (1.8, 9.5)], and fear of COVID-19 were determinants of late initiation of ANC in the study area.
Conclusion:
Age, pregnancy and care-related factors, and fear of COVID-19 were determinants of late initiation of ANC. Community-based provision of comprehensive information on planned pregnancy and the ANC is important. A resilient system has to be built to deliver essential health services during emergencies like COVID-19.
Introduction
Antenatal care (ANC) is a care provided by skilled health-care professionals to pregnant women to ensure positive health outcomes for both mother and the baby. 1 The World Health Organization (WHO) recommends the implementation of a new ANC platform that consists of eight ANC contacts and a well-defined set of activities proven to be beneficial for maternal and neonatal health. The term visit in the old focused ANC is replaced by contact to stress on an interactive approach enshrined in the newer version. The current recommendation also prioritizes person-centered health and well-being through the human rights approach of ANC, going beyond the prevention of morbidity and mortality.1,2
The development and implementation of the new ANC guidelines is in accordance with the renewed global commitment to global health and wellbeing in the Sustainable Development Goals (SDGs). One of the targets under the third goal of the SDG is to reduce the global maternal mortality ratio (MMR) to less than 70 per 100,000 live births by 2030. According to the latest global report, the global MMR in 2017 is estimated at 211 maternal deaths per 100,000 live births, representing a 38% reduction since 2000, when it was estimated at 342, but also indicating the need for concerted effort to meet the target. 3 Even though the global reduction in the MMR is promising, it shows that the world has a long way to go to achieve its targets. Extraordinary effort is needed to curb the problem in developing countries.
Sub-Saharan Africa (SSA) and Southern Asia accounted for approximately 86% (254,000) of the estimated 295,000 global maternal deaths in 2017, with SSA alone accounting for 66% (196,000) of maternal deaths. In the same year, Ethiopia recorded over 14,000 maternal deaths related to pregnancy and child birth, 3 with MMR of 412 per 100,000 live births in 2016. 4 Most maternal deaths are due to causes such as pregnancy-induced hypertension, hemorrhage, anemia, and abortion, which are directly related to inadequate care before, during, and after pregnancy. 5
ANC reduces maternal and perinatal morbidity and mortality both directly, through detection and treatment of pregnancy-related complications, and indirectly, through the identification of women and girls at an increased risk of developing complications during labor and delivery, thus ensuring referral to appropriate care. Despite enormous interventions, only 64% of pregnant women attended the WHO-recommended minimum of four contacts for ANC in 2014, suggesting that much more work needs to be done to address ANC utilization. Low ANC coverage, low ANC utilization, few visits, and delayed initiation of follow up were the predominant problems throughout low and middle income countries (LMIC) including Ethiopia resulting in failure of accomplishment of the SDG objectives. 3
Late ANC contact lacks the opportunity to provide screening services, diagnostic tests, and health interventions that are most effective early in pregnancy. Early assessment of gestational age helps to promote and provide tailored care and provide supplements to reduce the risk of fetal and maternal complications. Additionally, the visits can capture non-communicable diseases and provide guidance on modifiable risk factors such as smoking, alcohol consumption, drug abuse, obesity, and occupational exposures. All these conditions can be detected and treated if early and high-quality antenatal care is provided. 6
In the SSA, the ANC utilization is low when compared with developed countries. Pregnant women who have at least one ANC visit were 69%. Less than half of pregnant mothers had four ANC visit during their last pregnancy. Only one in five of pregnant women enroll to the ANC service within the first 4 months of pregnancy.4,7
Early antenatal care has the potential to reduce maternal and child mortality. A systematic review and meta-analysis found that ANC visit was significantly associated with a 34% reduction in neonatal mortality. 1 A cohort study carried out in Ethiopia reported that having four or more ANC visits was significantly associated with a reduction in postpartum hemorrhage, early neonatal death, preterm labor, and low-birth weight. 8
The current WHO recommendations on ANC have highlighted the importance of effective communication with pregnant women. These ANC communication and support functions were critical not only to saving lives, but also to improving lives, healthcare utilization, and care quality. Women’s positive experiences during ANC and childbirth can create the foundations for healthy motherhood. 1
Despite the widespread existence of late enrollment in the ANC, there has been no published study conducted to assess its determinants in the study area. Furthermore, the determinants of late initiation for ANC were not the same across different cultures, socio-economic statuses, and access to institutions within a society. Thus, assessing the determinants of late initiation of ANC follow up in different settings is important to improving maternal health services for which antenatal care is a key entry point. In addition, the advent of COVID-19 and its potential impact on ANC has not been assessed in prior studies. Therefore, this study will help to fill this gap and identify determinant factors of late ANC initiation among pregnant women attending antenatal clinics in public health institutions in Ilu Ababor Zone, South-West Ethiopia by adding the perceived threat of COVID-19 as an important variable.
Design and methods
Study area, design, and period
This study was conducted in Ilu Ababor zone, Oromia regional state of Ethiopia. Ilu Ababor zone has 13 woredas and 1 town administration. The zone has 263 rural kebeles (the smallest administrative organization in Ethiopia) and 23 urban kebeles. It has a total population of 933,325 of which 465,792 were females. The zone has two public hospitals, 40 functional public health centers and 273 health posts in 2022. A facility based unmatched case control study was conducted from October to December 2020.
Population
Source populations
All pregnant women who attend ANC clinics in public health centers of Ilu Ababor zone in 2020.
Study population
Cases were randomly selected pregnant women who were enrolled in ANC in Ilu Ababor zone public health centers after 20 weeks of gestation, as evidenced by maternal self-report of last normal menstrual period (LNMP) or ultrasound examination.
Controls were pregnant women who attend ANC clinic in selected public health centers of Ilu Ababor zone before or at 20 weeks of their gestational age as evidenced by maternal self-report of LNMP or ultrasound examination.
Inclusion and exclusion criteria
Inclusion criteria for cases and controls
All pregnant mothers who came for ANC visits in selected public health centers of Ilu Ababor zone were included in the study.
Exclusion criteria for cases and controls
Pregnant women who fail to remember their LNMP or for whom ultrasound examination is not conducted were excluded from the study.
Sample size determination and sampling technique
Sample size determination
Sample size was determined by using Epi Info software to determine two population proportions from the factors reviewed, which gives maximum value by using 95% CI, power 80%, case to control ratio 1:1, odds ratio = 2.32, prevalence of the exposure among cases as 36.2% and prevalence of exposure among controls as 19.6 %. 9 By considering a 10% non-response rate, the final sample size was found to be 278 (139 cases and 139 controls; Table 1).
Sample size calculation for the study entitled determinants of late antenatal care initiation among pregnant mothers in Ilu Ababor Zone, Oromia, Ethiopia, 2020.

Sampling technique
Twelve (12) health centers were selected using a simple random sampling method among 40 health centers in the Ilu Ababor zone; then the sample size was proportionally divided among the selected 12 health centers based on their past 12 months achievement of ANC.
The number of pregnant women who received antenatal care in the past 12 months before the data collection time was taken, and the average monthly achievement was calculated and assigned to respective health centers. All participating institutions provided ANC to 486 (486) clients, and the sampling interval was calculated by dividing this number by the total sample size; 486/2782. Accordingly, every other case from all health institutions was interviewed using a systematic random sampling technique. For each case, one adjacent control was selected consecutively until the required sample size was achieved. The first client was selected by lottery from the first two cases.
Operational definitions
Enough time
Time spent between health professional and pregnant women for counseling at previous ANC follow up and acceptable if ≥30 min at follow up.
Family support
Opinion, financial, and other physical support from family members such as husband, mother, sister, etc. during ANC service follow up. 5
Access to service
Availability of health facility providing ANC service within 2 h distance on foot. 11
ANC services waiting time
It indicates the time that the clients have to wait for the care providers to receive services and it is defined as acceptable if ≤45 min and not acceptable if >45 min. 5
Data collection procedure
A structured pre-tested questionnaire was used to collect the data. The study participants were interviewed about four category of behaviors. The exit interview technique was used to assess socio-demographic and economic determinants, individual-related characteristics, health care service determinants, and obstetric determinants. The questionnaires were adopted from the tools used by the Ethiopian Demographic and Health Survey (EDHS) 2015. 4
Data quality assurance
Data collection instrument was adapted from questionnaires used in national assessments by considering local conditions. The English version of the questionnaire was translated into the local language (Afan Oromo) and translated back to English to check consistency by language and medical experts.
Before the actual data collection, the questionnaire was pre-tested on 40 pregnant women outside the study area, and necessary modifications were made. Twelve experienced nurses carried out the data the data collection. A supervisor from each health center supervised the data collection process. Two days of comprehensive training was given to data collectors and supervisors on data collection tools, data collection and recording procedures, techniques, and necessary COVID-19 prevention precautions.
Data analysis procedures
Data was checked manually, entered into Epi-data software version 3.1 and exported to SPPS version 22 for analysis. Appropriate descriptive statistics, including mean, frequency, and percentage, were used depending on the nature of the variables. A bivariable analysis was performed to assess the association of each independent variable with late ANC initiation. Variables with a p-value less than 0.25 were entered into the multivariable logistic regressions. Backward stepwise multivariable logistic regression was used to identify independent determinants of late ANC initiation. The model fitness was tested by the Hosmer and Lemeshow goodness of fit test. Statistical significance was declared at a p-value less than 0.05. The Adjusted Odds Ratio (AOR) and its 95% confidence interval (CI) were used to determine the presence and strength of association.
Ethical consideration
This study was conducted according to the principles of the Declaration of Helsinki. The ethical approval was obtained from the research ethics review committee of the college of health sciences, Mettu University. A formal letter that explains the objectives, procedures, and expected outcomes of the study was written to the respective institutions. The respondents were informed about the objective and purpose of the study, and provided written informed consent. Privacy of the respondents was maintained and confidentiality of the information was respected at all levels.
Significance for public health
ANC is an essential primary health care program that is implemented to improve the health of mothers and children. Late enrollment in the ANC results in missing important windows of intervention to provide interventions that are most effective early in pregnancy. This study indicated the gap in the provision of comprehensive reproductive health information and suboptimal contraceptive as potential causes of delay in enrolling in ANC. In addition, it showed the necessity of building a resilient health system that withstands emergencies to provide continued care to pregnant women.
Result
Socio-demographic characteristics of respondents
A total of 270 pregnant women (135 cases and 135 controls) participated in this study, with a response rate of 97%. More than a quarter (28.9%) of cases were within the age group of 25–29, and 54 (40.0%) of controls were within the age group of 20–24. Most of the cases, 93 (68.9%) and 73 (54.1%) of controls were rural residents. Married women contributed to 113 (83.7%) of cases and 116 (85.9%) of controls. One hundred eight (80%) of cases and 101 (74.8%) of controls were ethnic Oromos. Sixty-two (45.9%) of respondents were Muslims. Nearly half of both cases and controls had no formal education. Considering occupation, 81 (60.0%) of cases and 78 (57.8%) of controls were housewives. One hundred twelve (83.0%) of cases and 124 (91.9%) of controls lived with a family size of five or less. The husbands of 64 (56.6%) of cases and 42 (36.2%) of controls were farmers (Table 2).
Socio-demographic characteristics of pregnant mothers attending selected health centers in Ilu Ababor Zone, 2020.
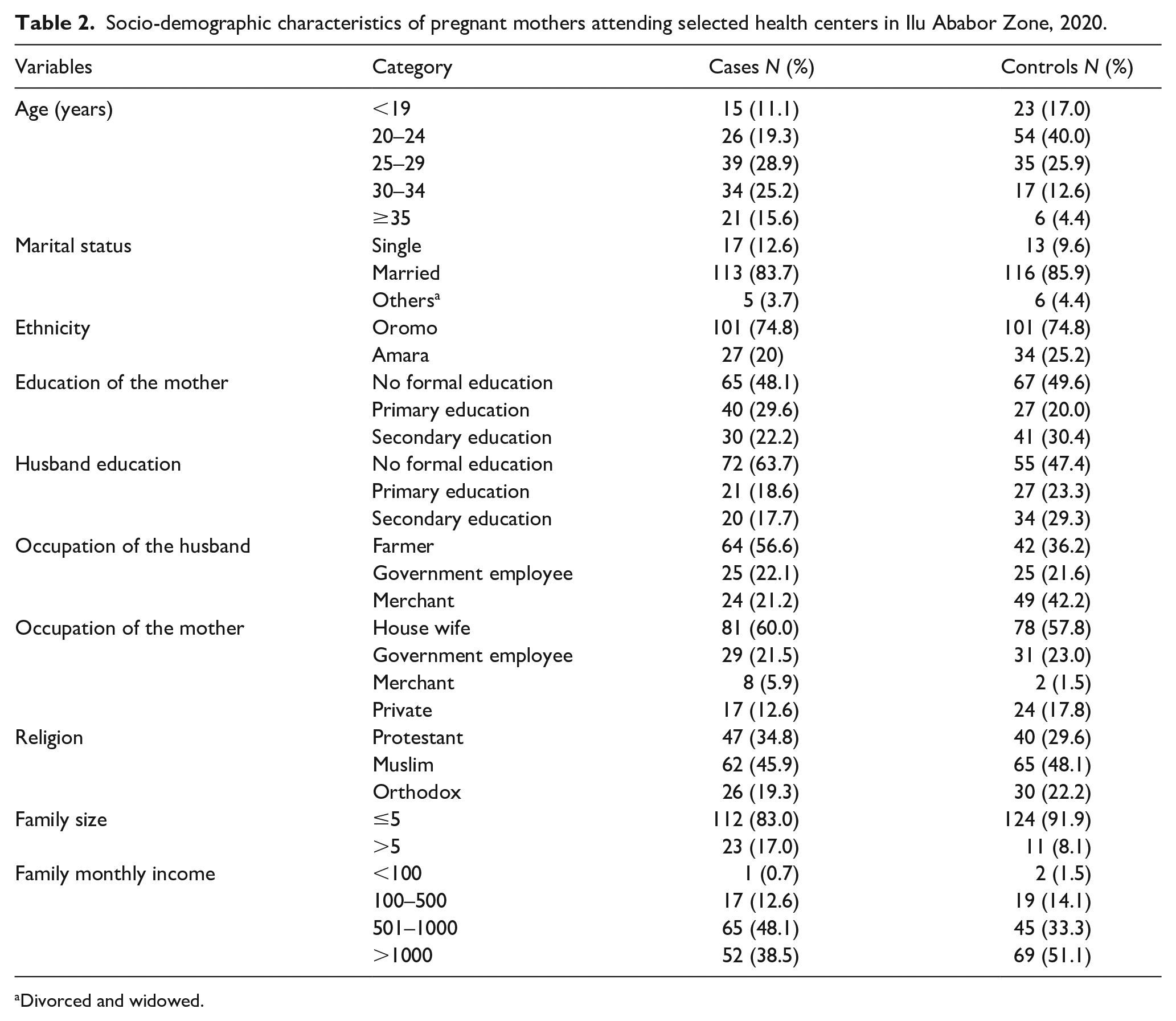
Divorced and widowed.
Obstetric characteristics and antenatal care utilization of the respondents
Forty-one (30%) of cases and 56 (41.5%) of controls were pregnant for the first time. From the multigravida, 67 (71.3%) of cases and 71 (89.9%) of controls had history of ANC visits in their previous pregnancy. Regarding current pregnancy, 56 (41.5%) of cases and 73 (51.4%) of controls had a planned pregnancy. Seventy seven (57.0%) of cases and 106 (78.5%) of controls were informed about the right time of initiation of ANC. Of these, 53 (57.0%) of cases and 88 (79.3%) of controls got the information from health professionals (Table 3).
Obstetric characteristics and antenatal care utilization of pregnant mothers attending selected health centers in Ilu Ababor Zone, 2020.

WHDA: Women Health Development Army.
Concern for COVID-19 and health care related characteristics
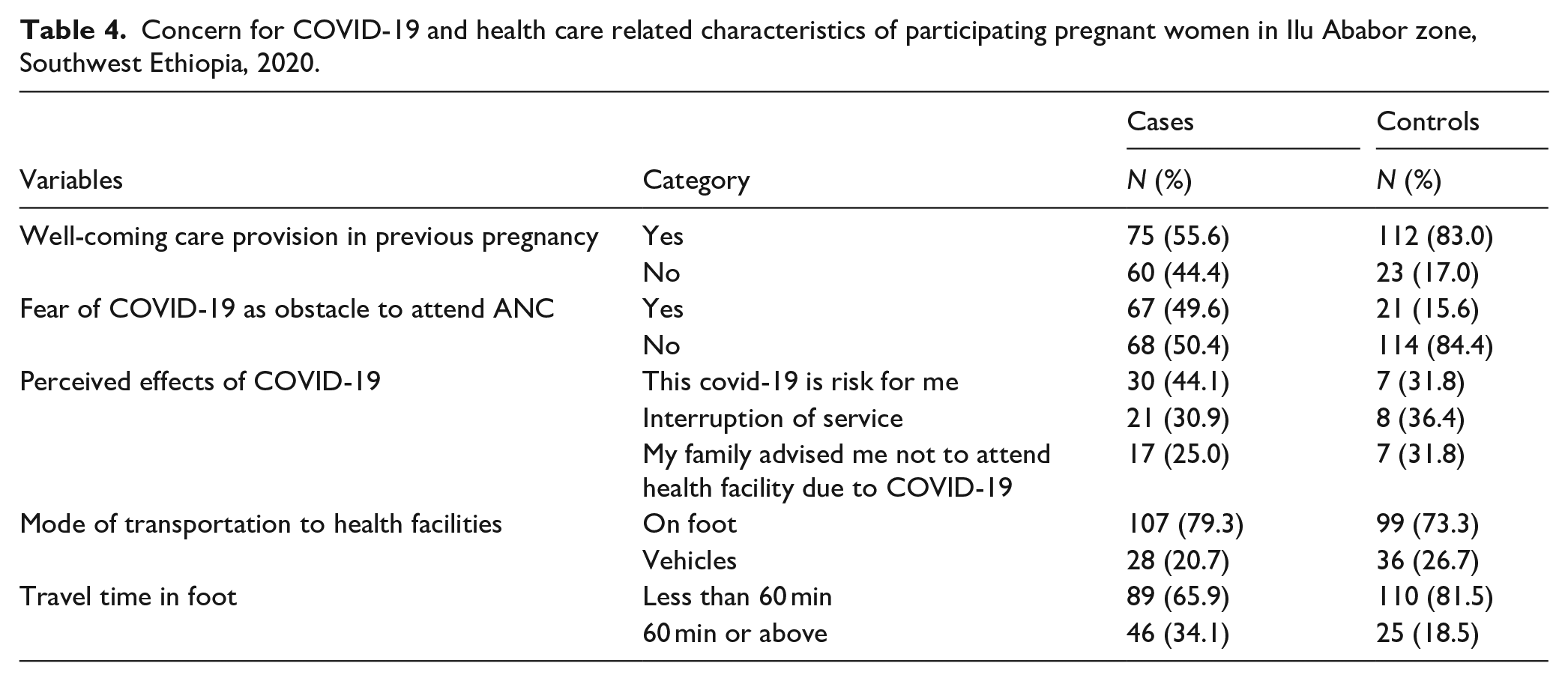
Sixty-seven (49.6%) of cases and 21 (15.6%) of controls reported that fear of COVID-19 was a major obstacle that prevented them from enrolling in the ANC early. Of these, 30 (44.1%) of cases and 7 (31.8%) of controls responded that COVID-19 was a risk to their health. Concerning accessibility of health care, 107 (79.3%) of cases and 99 (73.3%) of controls walked on foot to go to the health facility for ANC. In addition, 46 (34.1%) of cases and 25 (18.5%) of controls spent more than 60 min to reach the nearest health facility to get ANC service (Table 4).
Concern for COVID-19 and health care related characteristics of participating pregnant women in Ilu Ababor zone, Southwest Ethiopia, 2020.
Independent determinants of late ANC initiation
In the bivariable logistic regression, 11 variables showed significant association with p-value 0.25 and were taken to the multivariable model (Table 5).
Bivariable model of determinants with late first ANC initiation among pregnant women in selected health centers of Ilu Ababor zone, 2020.

1 = reference category.
In the multivariable logistic regression model, information on time of booking first ANC, fear of COVID-19, age, unplanned pregnancy, and not attending ANC for past pregnancy were significant determinants of late enrollment in the ANC among pregnant mother receiving care in public health centers of Ilu Ababor zone.
Lack of information on appropriate time of enrollment to ANC was found to be a significant determinant of late ANC initiation. Women who lacked information on time of first ANC visit were twice more likely to book late for the service than women who were informed on appropriate time of booking for ANC [AOR: 2.26; 95% CI: (1.02, 4.99)].
Respondents who feared COVID-19 as a barrier to receiving health care were four times more likely to delay their ANC enrollment than women who were not concerned of the disease [4.28; 95% CI: (1.76, 10.40)]. In addition, women with an unplanned pregnancy were nearly three times more likely to start the care late compared to women with a planned pregnancy [AOR: 2.76; 95% CI: (1.25, 6.10)].
Women who did not receive ANC in their last pregnancy were four times more likely to book late when compared to women who had attended ANC in their past pregnancy [AOR: 4.07; 95%CI: (1.75, 9.46)]. Age was also found to be a significant determinant of the late initiation of ANC. Older women with age of 25 years or older were twice more likely to start ANC later than younger women under 25 years [AOR: 2.18; 95% CI: (1.01, 4.74)] (Table 6).
Multivariable logistic regression for determinants of late Antenatal Care initiation among pregnant women attending health centers of Ilu Ababor zone, 2020.
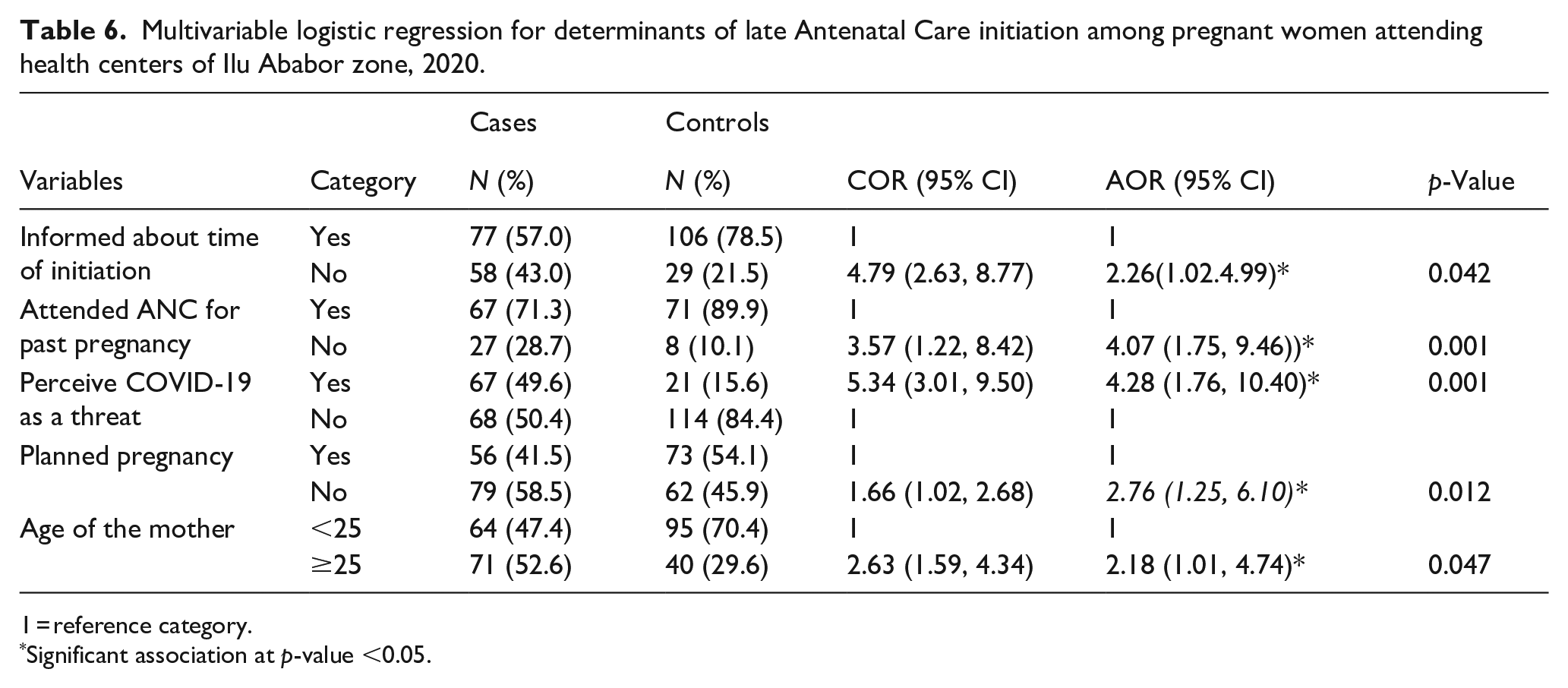
1 = reference category.
Significant association at p-value <0.05.
Discussion
ANC is an essential health care provided to pregnant women to ensure positive pregnancy outcomes. In addition, it lays the foundation for implementing other interventions to promote the health of infants and children. Late initiation of ANC has remained a challenge in developing countries. This study aimed to identify factors that predispose pregnant women to the late initiation of ANC services.
In this study, unplanned pregnancy, lack of information on time of booking first ANC, perceived threat of COVID-19, age ≥25, and failure to attend ANC for previous pregnancy were all significantly associated with late enrollment to the ANC in this study.
The current study revealed that women with an unplanned pregnancy were more likely to initiate ANC late when compared with women whose pregnancy was planned. This study was comparable with a study conducted in Northern Tigray. 9 Evidence from Addis Ababa also indicated an unplanned pregnancy to be an independent determinant of late ANC initiation. 10 A study from Dilla and Myanmar also indicated that women with unplanned pregnancy are more likely to visit late for their first ANC.12,13 Women with unintended pregnancies are generally less likely to use health services meant to improve maternal and child health. Pregnant women with unplanned pregnancies might lack support from their partners or families. In addition, they might not recognize their pregnancy early to make necessary arrangements to enroll in ANC. 14
In this study, older mothers were more likely to start ANC late than younger mothers. This finding is supported by a study conducted in Northern Ethiopia, where older women initiated ANC later than the younger ones. 15 This finding is also similar with finding from studies conducted in East Wollega and Boke where older mothers were less likely to start ANC within the recommended period than younger ones.5,16 A study conducted in Gedo hospital indicated the reduced likelihood of late initiation of ANC among younger women. 17 The possible explanation for this could be that young women may consider themselves at high risk of pregnancy complications and therefore take the precautions to avert them.18,19 Another reason could be that older women are more likely to have many children to care for, and many of the older women might have cultural biases against formal health care.
In this study, respondents who did not attend ANC in the past pregnancy were more likely to enroll late in ANC. This result was in line with a finding from studies conducted in Tigray and Southern region which indicated that women who had no previous ANC follow up were more likely to start ANC late compared to women who had previous ANC follow up.20,21 This could be due to the positive experience of health improvement and implementation of advice and recommendations given by health workers during the first ANC attendance. The recent ANC guideline by the WHO stresses the importance of using the enrollment as a stepping stone to enhance utilization of other maternal health services and future ANCs. 1
Access to information was strongly associated with early enrollment in the ANC. Pregnant mothers who lacked information on the time of first ANC contact were more likely to enroll later in ANC than mothers who were informed about the appropriate time of booking. This result was supported by findings from studies carried out in Addis Ababa, Northern Ethiopia and Gondar.10,15,22 Women who had information on the appropriate time of first ANC booking were also more likely to start ANC early. 23 A study conducted in Dilla was also in line with this study, showing that pregnant women who did not receive advice on the recommended time of initiation were more likely to be registered late for their first ANC than their counterparts. 12 This shows the importance of continued information dissemination activities through diversified means to improve utilization of maternal health services like ANC. 24
COVID-19 has resulted in major disruption to the delivery of maternal health care in many ways. 25 In this study, COVID-19 had a significant effect on the timing of first antenatal care. Women who perceived COVID-19 as an obstacle to getting health service were four times more likely to attend late than women who were not concerned about COVID-19. Similar to this finding, a study conducted in six facilities in Kenya showed delayed initiation of ANC among women who delivered during the COVID-19 pandemic. 26 A study done in public hospitals in Northern Ethiopia also indicated that fear of COVID-19 infection was significantly associated with a reduction in ANC service utilization. 27 This may be due to the low preparedness of health centers to cope with the changing realities during emergencies like COVID-19, as only 26% of facilities in Ethiopia were deemed prepared to cope with the disease and the preventive principles of COVID-19 might not be practiced properly. 28 Fear of getting the infection due to physical proximity may have also limited the readiness of women to go for health care early. 29
Limitations of the study
Pregnant women who attended ANC at hospitals were not included in the study. This may limit the generalizability of the finding to some degree. In addition, LNMP was used to identify cases and controls. This may result in recall bias which leads to non-differential misclassification bias. So errors are made in classifying either disease or exposure status happens in more than one direction which may dilute the study findings.
Conclusion and recommendation
Conclusion
In this study 135 cases and 135 controls were participated with the response rate of 97%. Demographic characteristics, pregnancy and care-related factors, and fear of COVID-19 were significant determinants of late initiation of ANC among pregnant women in the study area.
Recommendation
To gear towards timely enrollment of all pregnant women into the care, community based provision of comprehensive information on planned pregnancy and the ANC is important. Older women should be specially targeted with interventions. A resilient system has to be built to deliver essential health services during emergencies like COVID-19. The opportunity of enrollment at any stage has to be used to lay ground for future adoption of healthy practices among pregnant women.
Footnotes
Acknowledgements
We thank all who helped us in the conduct of this study. We thank the data collectors, supervisors, and research facilitators for helping in the realization of this work. Finally, we thank the study participants for giving us their time and valuable information in this study.
Author contributions
All authors; Mr SZ, Mr, MS, and Mr.AT made equal contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
This study was conducted according to the ethical principles of the Declaration of Helsinki. The proposal of this study was reviewed and cleared by the Ethics Review Committee of the College of Health Sciences, Mettu University. Written informed consent was taken from selected participants ahead of data collection after the provision of comprehensive information regarding the study. All information provided by the participants was kept confidential and anonymous. In addition, any information that may lead to the identification of the study participants was not included in the data collection instrument.
Availability of data and materials
All data for this research article is available and can be accessed from the corresponding author at any time.