
Abstract
Introduction:
Evidences suggest a significant decline in maternal health service uptake following the coronavirus disease 2019 (COVID-19) pandemic in Ethiopia. However, COVID-19 related factors impacting the service uptake are not sufficiently addressed. Hence, the current study was intended to explore COVID-19 related factors influencing antenatal care service uptake in rural Ethiopia.
Methods:
A community-based qualitative study was conducted from September 25/2020 to November 25/2020 among selected pregnant women residing in rural districts of Bench-Sheko Zone, and healthcare providers working in the local health care facilities. Six focus group discussions and 9 in-depth interviews were made between pregnant women, and health care providers, respectively. Data was collected by health education and behavioral science professionals who also have experience in qualitative data collection procedure. Data were transcribed, translated, and analyzed thematically using Open Code 4.0 software.
Result:
The study revealed several COVID-19 related factors influencing the uptake of antenatal care service during the pandemic. Health facility related barriers, perceived poor quality of care during the pandemic, government measures against COVID-19, anxiety related to the pandemic, and risk minimization were the identified factors possibly influencing the current antenatal care service uptake among women in rural Bench-Sheko Zone.
Conclusion:
COVID-19 preventive measures, and health facility related factors and individual factors were responsible for the current decline in antenatal care service uptake. Preserving essential health care service is critical to prevent avoidable losses of maternal and child lives during the pandemic period. Hence, programs and strategies designed to maintain maternal health services particularly, antenatal care service have better take the above determinants into consideration.
Introduction
The impact of COVID-19 pandemic influence worldwide health system, essentially disturbing care provision with high levels of morbidity and mortality.1-5 With more than 56 077 335 cases and 1 346 248 and above deaths were reported globally, 6 numerous nations have executed strict social distancing rules with full or halfway lockdowns again in second wave. 7
COVID-19 also disturbing health, social welfare and the economy in an extent unparalleled in present day history. In expansion to the impacts of the disease itself on public health, a collateral impact to near-universal disturbance.8,9 This outbreak also changed main concerns of the health system, which is finding itself not only overwhelmed but moreover with limited capacity to supply services it has been up to this point expanding to communities. 10
This pandemic may add additional burden and concern for expectant women and for those who give care for them. There is no clearly known evidence weather the pregnant women are more vulnerable to COVID-19 than the others but due to changes that happens during pregnancy, pregnant women may be more at risk to viral respiratory infections.11,12
Since the Covid-19 pandemic, average weekly antenatal care visit was decreased by 16.1%, from 898 to 761 weekly visits. 13 Antenatal healthcare services and routine follow-up at clinics were being delayed at public hospitals due to the temporary reallocation of staff to isolation wards, quarantine camps and centers, screening units, the national lock-down, and also due to the fear among healthcare professionals. 14
The maternal deaths were anticipated to rise by 17% within the best-scenario and 43% within the case of the most exceedingly bad situation due to the COVID-19 pandemics. 15 Movement restrictions or lockdown, transport problems and anxiety secondary to being exposed to corona virus possibly are acting as the factors that affect the utilization of maternal health service. 16
Health professionals may not be able to give the highest quality of care at the time of COVID-19 pandemic with basic safeguards in put, client-provider communication is seriously affected and the time to get the service required may take more as health workers attempts to secure themselves from the contamination. 17
There were changes to antenatal care (ANC) in Europe designed to reduce the COVID-19 infection risk for pregnant women and staff, and whilst phone and online consultations can be acceptable and valued by women as an interim measure 18 and also in order to reduce the risk of infection national policies have proposed that non-mandatory hospital appointments be removed and replaced with remote support as much as possible. 19
In Ethiopia there was huge burden caused by the COVID-19 episode is jeopardizing routine service delivery and undermining other health priorities 20 with 103 395 cases and 1588 death was reported. 6 United Nations Population Fund (UNPF) recently stated that “Ethiopia’s midwives grapple with COVID-19 while ensuring safe delivery.” 21
As the COVID-19 continues to spread globally, vulnerable populations living in countries with weak health systems are at high risk of being hit the hardest. 22 Given the already existing limited service infrastructure 23 and poor health literacy, 24 maternal health service uptake in rural community in Ethiopia would be disproportionately affected by the advent of COVID-19 pandemic. However, very few studies attempted to investigate the COVID-19 related barriers to service uptake in rural setting. Thus, the aim of this study was to explore COVID-19 related factors influencing ANC service uptake in rural Bench-Sheko Zone, Ethiopia.
Conceptual framework was developed after reviewing several related literatures. The below figure reveals the relationship of the health facility factors, risk minimization measure, perceived poor quality of care, anxiety, and government measures on prevention and control of COVID-19 with maternal health service utilization (Figure 1).
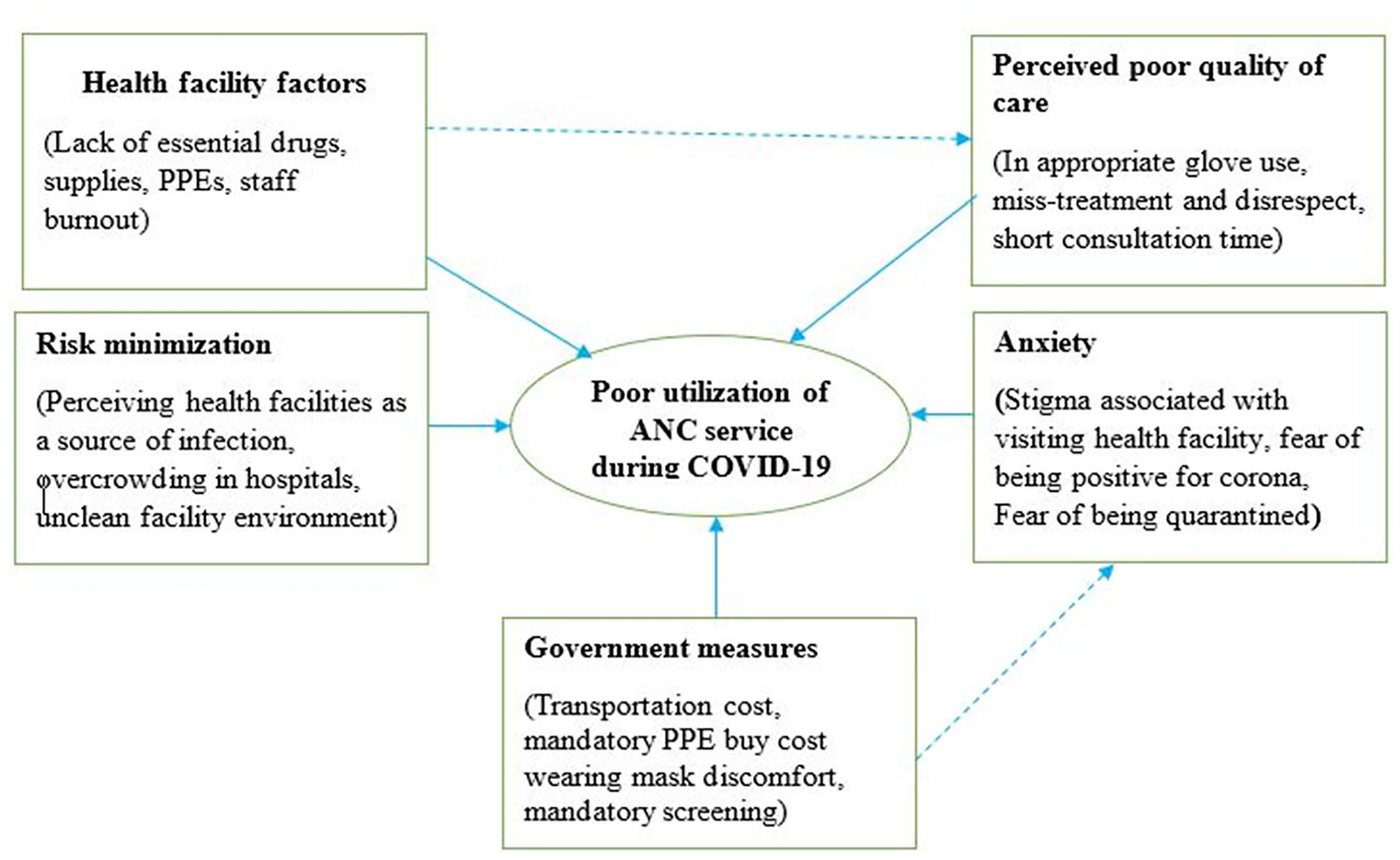
Conceptual model of COVID-19 related factors influencing maternal health services uptake among women in a rural community in Bench-Sheko Zone, 2020.
Methods
Study Design
A qualitative approach, exploratory descriptive design was employed. This design allows the investigator to explore the participant’s perspective of the phenomena under investigation. 25
Study Setting
The study was conducted from September 25/2020 to November 25/2020 in Bench-Sheko zone which is located 561 km away from Addis Ababa, the capital city of Ethiopia, in Southwest direction with an estimated population of 829 493 out of which 418 213 are women, 129 500 are children under 5 and 26 462 are under 1 year. 26 The expected number of households in the zone is about 169 284 and the primary health service coverage of the zone is 92.6% covering a total catchment area of 19 965.8 km2 with majority 86% (1 061 120) of the population living in the rural areas. The zone includes a city administration (Mizan-Teferi), 6 Woredas (districts), 246 kebeles (smallest administrative units) (229 rural and 17 urban). The zone has 2 Hospitals, 26 health centers, and 182 health posts. The zone has 12 physicians’ and 511 of health professionals of different ranks and 476 health extension workers. 27
Study Population and Sampling
The study was conducted among pregnant women residing in rural Kebeles of the selected districts: Gurafarda, Sheko, and Debrework and health care providers working in the same areas. These districts were purposely selected based on their District Health Information System (DHIS) reports on ANC service uptake. Districts that reported a significant decline in antenatal care service uptake during the COVID-19 pandemic, namely Gurafarda, Sheko, and Debrework were considered for this study. Six Focus Group Discussions (FGDs) were undertaken among pregnant women who did not attend all the recommended ANC visits. Gestational age third trimester and above, being able to speak the local language (Amharic), age group 18 to 45 and residing in the area for at least 6 months were considered as inclusion criteria when recruiting FGD participants and a convenience sampling technique was used to select pregnant women who met the inclusion criteria. In order to explore health care providers’ perspectives on factors influencing ANC uptake in the area, 9 in-depth (3 per district) interviews were undertaken among purposely selected health care providers working in facilities found in selected districts.
Data Collection
A total of 6 FGDs (2 FGDs per district) were conducted among pregnant mothers who never attended ANC since the COVID-19 outbreak in Ethiopia (March 13, 2020). In the field, health developmental army (HDA) leaders were used to identify pregnant mothers who did not attend the recommended ANC. With the help of them, pregnant women who didn’t attend ANC were identified. Then, Principal investigator and HDA leaders visited the identified pregnant women and the women were further screened against the inclusion criteria. After securing the informed consent, they were told the schedule and the place where the FGD was going to be carried out. Self-developed FGD guides were used as an instrument for undertaking FGD discussions. Before the opening of each FGD session, the purpose of the study was explained, and upon ensuring all FGD participants’ agreement, the session was formally commenced; the FGD discussion sites and schedule were chosen by participants’ interest. In order to prevent the potential transmission of COVID-19 among FGD discussants, different precaution measures were implemented such as: maintaining physical distancing, using personal protective equipment (PPE) and fixing the size of the FGD groups at most 8. The FGD sessions were led by 2 health education and behavioral science professionals who also have experience in qualitative data collection as a moderator and one research assistant (BSc Nurse) as a rapporteur. Each session lasted about 70 to 90 min. All FGD sessions were tape-recorded and notes were taken to guarantee the accuracy of the data. The 9 in-depth interviews were undertaken among health care providers in the health centers they were working in using an interview guide. The interview guide was self-developed and served as a data collection instrument. The interview sessions lasted 30 to 40 min and all interview sessions were tape-recorded.
Data analysis
The data collected from FGDs and IDIs were analyzed thematically using Open Code 4.0 software. All audio-records and notes which were in the local language (Amharic) were transcribed and then translated into English. Audio-records and notes were compared to the transcribed data to ensure accuracy. Transcripts were carefully read, comprehended, and assigned codes. Similar codes were combined to form umbrella themes based on the research objective as well as themes that emanated from the data itself. To insure the objectivity of the finding, the analysis was carried out discretely by 2 authors. Then the finding was discussed between the 2 authors and the themes that the 2 authors agreed upon was written and a serious debate was made on the themes that the 2 authors disagreed upon until consensus reached. Finally, in presenting the finding, individual quotes were used to underpin the umbrella theme being discussed.
Trustworthiness
Trustworthiness of a qualitative study is the extent to which the identified meanings represent the perspectives of the participants accurately. The 4 criteria for ensuring trustworthiness which includes credibility, transferability, dependability, and confirmability were insured. 28 To guarantee credibility, a member check was done by inviting some of the participants to affirm the accuracy of transcribed data and emerging themes as truly representing their experiences. A clear description of the procedure for participants’ recruitment and detailed description of the research setting was done in order to enhance transferability. Method implemented for data collection, analysis, and interpretation is also captured within the report for dependability. An audit trail consisting of field notes, audio recordings, analysis notes and coding details were also kept for confirmability.
Results
A total of 44 pregnant women participated in the FGD discussions. Participants’ age ranges from 25 to 43 ages and all were married. Regarding their educational status, 29 of them didn’t attend any formal education, and 15 of them claimed to attend primary education. Majority of the participants (32) were protestant religion followers and the rest were Orthodox Christianity and Muslim religion followers 8 and 4, respectively. Nine healthcare provider were interviewed. Of them, the 3 were Midwives, 3 were Nurses, and the rest 3 were health extension workers.
Health Facility Barriers
Healthcare providers and health extension works mentioned several facility barriers impacting ANC service uptake during the COVID-19 pandemic which are majorly related to poor logistic supply, staffs’ reduced work appetite due to lack of risk allowance and other necessary accommodations, and patient overcrowding which is against the COVID-19 prevention measure of physical distancing.
“During this corona virus period, health care providers are facing huge challenges as staffs are assigned in different corona virus related tasks such as: isolation room, provision of health education, screening centers and etc. In this case, it is difficult for a single health care provider to provide antenatal care service alone and it would even be much more difficult on market days where most pregnant women often chose to visit antenatal care.” (
Interviewed maternal and child health (MCH) coordinators also stated that due to health system resource shifting toward prevention and control of COVID-19, various rural health facilities including ours are suffering from a serious shortage of essential drugs and supplies, and PPEs which are crucial for routine service provision.
“Since the corona virus pandemic, we are facing a serious shortage of essential drugs and supplies like: alcohol, iron, face mask, and other personal protective equipment. If we take, for example, shortage of personal protective equipment, without them, the risk of transmitting the corona virus will be increased. To decrease the risk of transmission, we usually compromise the routine antenatal care service. For instance, we may not perform physical examination or draw blood, even if necessary.” (
Some health care providers also mentioned that they are feeling de-motivated and losing their work appetite as the government gave no attention to health care providers, despite the fact that they are working in a COVID-19 risky environment without risk allowance, and other necessary accommodations.
“After working the whole day in the work place, at night I go home; imagine the risk I could bring to my family. Why would I take such a risk? Where the government is not even willing to pay a risk allowance, let alone arrange accommodation for staff. I have a family to support; I no longer have interest to work in this environment.” (
Interviewed health extension works also suggested that due to the overcrowding in the service waiting areas; clients are being told to wait outside in order to maintain physical distancing and reduce the risk of COVID-19 transmission.
“During my home to home visit for consulting the benefit of maternal service utilization for pregnant women, I have encountered many pregnant women complaining on antenatal care service, more importantly on the waiting area that pregnant women have to wait for a long time outside of the waiting area to get the service.” (
Perceived Poor Quality of Care During COVID-19
Pregnant women, based on the information they gained from their neighbor, friends or relatives, perceived the quality of maternal health service including ANC during the COVID-19 pandemic as poor. For instance, some pregnant women complained of inappropriate use of PPEs by health care providers.
“As my neighbor told me, healthcare providers often use the same glove for different clients, and they don’t use alcohol regularly; I think all they do care about is only for themselves. Some of them even move here and there but they don’t change their gloves before toughing you.” (
Other FGD participants argued that due to staff and material shortage as a result of the COVID-19, pregnant women may not receive adequate care during ANC visit.
“This days everyone is talking about CORONA virus, and I don’t think that healthcare providers have a time to treat pregnant women as usual. Thus, what is the point of visiting a health facility for antenatal care if you don’t have enough time to be treated and advised?” (
“I don’t think the health care facilities in this pandemic period have the necessary materials for providing antenatal care service. . .. . .the Medias, the government, and everybody is saying corona, corona, corona . . ...” (
Others also claimed to have encountered pregnant women who were miss-treated and disrespect by health care provider.
“I would not advice pregnant women to visit a health facility during this corona virus period. What I heard from those who visit a health facility is completely discouraging; health care providers often disgrace you and even insult you. Though, I don’t blame them for doing so since they are taking a high risk; just think about working in the corona virus period? Hum. . .they have a family too.” (
Government Measures Against COVID-19
Several FGD participants claimed that transport challenges, compulsory use of face mask and mandatory screening are affecting them from trying to access maternal health care during the pandemic.
“Now, transportation cost is doubled. For this reason, I am forced to pay for two seats. Besides, it’s mandatory to wear a face mask unless they don’t allow you to use the service. It is difficult for me to afford all those things where my income is decreased by the pandemic already.” (
Some complained about discomfort over face mask enforcement and mandatory screening for COVID-19.
“It is mandatory for every individual to use a face mask, but when I use a face mask, it becomes strange to me and I can’t talk and breathe freely. I also feel suffocated and my breath smells bad. For this reason, I often chose to stay home.” (
“Everywhere you move, there is corona testing; you don’t have an option for not to be tested and it is mandatory for everyone. The problem is that they test you in an open field where everybody can watch you. If, unfortunately, I become positive, I will be taken to hospital publicly, without keeping my secret.” (
Anxiety
Several FGD participants mentioned that they are anxious about social isolation following one’s visiting health facility.
“I have witnessed that women who visit a health facility for any reason were considered to bring the virus into the community; thus, people refrain from meeting them.” (
Others also explained various psychological and social costs of being quarantined.
“I am afraid of visiting a health facility in this pandemic period because health care providers test every one coming to the clinic and who knows. . .I may end up in quarantine just because my body become hot due to reasons other than corona. If so, who would care for my children, while I’m in quarantine for about 2 weeks?” (
“I don’t want to know my test results, because I can’t with stand the stress of being positive for corona virus. I have heard a story of many individuals who had attempted suicide.” (
Risk Minimization
Most of the FGD discussant perceived that health facilities area potential source of infection for COVID-19 due to unclean facilities’ settings, and overcrowding.
“I don’t think that health facility environment is neat at this time. I doubt that they might not frequently clean surfaces, walls, chairs, and materials needed for treatment. If I go to health facility, I may contact with those unclean materials and get infected with the virus.” (
“Health facilities give service for all clients coming from different areas; this results in overcrowding and makes it easier for corona transmission. Thus, rather than going to health facility, I prefer seeking advice from health extension worker.” (
Other participants outweighed the risk of getting COVID-19 following facility visit over the benefit that mothers and babies would get from ANC service.
“Pregnant women who didn’t visit antenatal care could deliver safely without any problem, but if she gets infected with corona, she will be seriously ill and may not even survive. So, I would advise pregnant women not to visit health facility in this dangerous time.” (
“How would one compare the benefit that the baby gets from antenatal care service utilization with the risk of getting corona by visiting health facility? In my opinion, the virus is much more serious than the problem that may occur to the baby from not using antenatal care service.” (
Discussion
This is among the few qualitative studies intended to explore factors influencing maternal health service uptake during the COVD-19 pandemic period in rural Ethiopia. The study explored several health facility, psychosocial, and individual factors which are related to the current pandemic and responsible for not attending ANC among pregnant women during the pandemic period.
In this study, health care providers explained different facility barriers related to poor logistics, staff redeployment, and lack of incentive package affecting the provision of ANC service during the pandemic. This claim is corroborated by other literatures suggesting that COVID-19 pandemic disrupted the provision of essential services including maternal health services due to the engagement of staffs in COVID-19 related tasks, and inadequate financing as countries made major resource shifting toward COVID-19 prevention and control.14,29-32
Maternal perception of poor quality of care during COVID-19 was explained as the main reason why pregnant women didn’t attend ANC. Sharing their concerns that pregnancy related issues during the pandemic period may not be given sufficient attention as it was before. They also mentioned that health care providers may not use PPEs appropriately, clients may not be given adequate contact time and may get miss-treated, and health care providers also may not have the eagerness to work at this time. Indeed, these concerns of the participants’ are substantiated by other findings affirming the presence of significant change in maternal health service quality after the pandemic.17,31,33
Recent studies established the fact that the implementation of various COVID-19 prevention modalities by several countries has resulted in decline in household income, living cost inflation including transportation cost, and this makes it tougher for pregnant women to access a health facility. In line with the existing literatures, our study also demonstrated that government’s restriction measures such as the use of face mask, compulsory screening and increment in transportation cost played an important role in influencing mothers not to the access ANC service. This implies that the measures that are being taken against COVID-19 are causing an unforeseen consequence on maternal service utilization.14,16
Anxiety resulting from fear of being positive and fear of being quarantined were cited as an excuse for not attending the ANC during the current pandemic period. Similarly, other studies also evidenced that the uncertainty, fear, and high levels of stress around the pandemic are making pregnant women not to utilize health care facilities.19,34,35 Some of the participants reported to have witnessed pregnant women experiencing stigma following their health facility visit. This shows that the community supposes that pregnant women who had gone to a health facility would have already been infected by the virus. Thus, pregnant women refrain from visiting the health facility anticipating the stigma that would follow.
Other participants stated that they could spare themselves from the pandemic by minimizing the risk of exposure to the virus. They assumed that visiting the health facility in this pandemic period is unsafe due to the overcrowding in the waiting area, uncleanness of the health care facility’s environment, and etc. Pregnant women abandonment of maternal health care service as part of COVID-19 risk minimization was also described by other previous study.36,37
Conclusion
The covid-19 pandemic has caused a significant disruption in the health system and health behaviors of the community, notably in low-income countries with already weak health system. The COVID-19 prevention and control modalities seem to exacerbate the existing poor maternal health service utilization. Health Resource shortage, cost of transportation following movement restriction had a negative impact on ANC uptake. Anxiety, perceived poor quality of care, and pregnant women’s risk minimization strategy were among the client factors that affect the ANC uptake. Hence, health facilities have better adapt their capacities to the changing need of COVID-19 through deployment of additional health force, availing logistics, and other supplies. Also, health education programs should be designed to reduce the mental impact of COVID-19 on pregnant women and attempts should be made to preserve the quality of maternal health service during the pandemic period.
Limitations
This study needs to be seen in light of the following limitation. The fact that the study was entirely qualitative, it was impossible to quantify the extent of the problem. Moreover, given the nature of the study, it makes it difficult to identify which factors influence ANC service uptake the most among others.
Footnotes
Acknowledgements
The authors would like to thank Mizan-Tepi University for technical support and ethical approval, study participants, and data collectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The datasets collected and analyzed for the current study is available from the corresponding author and can be obtained upon reasonable request.
Ethical Consideration
Ethical clearance was obtained from the internal ethical review board of Mizan-Tepi University, reference number Ref HSE/00429/2020. Official permission letter was also obtained from Bench-Sheko Zone administration health office. After explaining the purpose of the study written consent was obtained from each of the study participant. Confidentiality and anonymity had been ensured throughout the execution of the study by taking only the required information without using the name of the participants.