
Abstract
Background:
During the Covid-19 pandemic, delays in providing medical services, dissatisfaction, criticism toward health workers (HW) and the risk of burnout of HW in Italy have been documented. No studies have contrasted the point of view of HW and users on the quality of care and respect for human rights in health facilities.
Objective:
To compare the perception of users of their satisfaction with the care provided with the perception of HW of their satisfaction with work as well as the perception of the respect of HW “s and users” human rights.
Methods:
The “Well-Being at work and respect for human rights questionnaire” (WWRR) was administered on a sample of users (142) and HW (154) in four outpatient health care facilities of a hospital in Sardinia, Italy.
Results:
Users showed higher scores than HW on their satisfaction with the care received (p < 0.0001), the perception of respect for their human rights (p < 0.0001), and availability of resources for care (p < 0.0001). The HW scores were higher than 50% of the maximum in all items, but a relatively low score was reported on the HW’s satisfaction of the resources and the respect for their rights.
Conclusion:
The satisfaction for care and respect for human rights in the outpatient health services was higher than expected. The relatively low score by the HWs in relation to the satisfaction with the resources and perception of respect for their human rights could be a wake-up call. The study does not involve emergency rooms, wards, or Covid units.
Introduction
In Italy the Covid pandemic has had a stronger negative impact than elsewhere: in the first wave in 2020, Italy recorded a mortality rate among the highest in the world. Moreover, during the fourth wave, in late winter 2021, there was an increase in infected cases among the highest in the world despite a fair portion of the population having been vaccinated. 1 HW and users of health care facilities (even for other illnesses than Sars-Cov2 infection) were among the most exposed to the risk of contagion and stress related to the pandemic.
HWs paid a high price, according to Italian National Institute for Insurance in 2020, with 70,000 work accidents affecting HWs registered due to the COVID-19 pandemic COVID-19, and 60% of the fatal cases affecting nurses. 2 A considerable number of scientific articles have documented the level of stress of HW in Italy during the pandemic and highlighted how the risk of anxiety, depressive symptoms, and post-traumatic stress disorder were closely linked with the fear of getting sick and the perception of organizational inefficiencies.3–6 The awareness of being discriminated against by users and the community was another important element related to stress for HW. 7 HW, especially those who worked on the front line, often became the target of the population’s dissatisfaction about the organizational inefficiencies of the health system, of which the same HW were paradoxically victims. If in the early weeks of the pandemic, HW were praised by media and by the community as “heroes,” the attitude toward them quickly changed. With the time, from being considered heroes, HW started being identified as the culprits of the failures of the health system in addressing COVID-19 and they were the subject of numerous cases for compensation filed by citizens. 8
Citizens in need of treatment for medical conditions other than Covid also suffered during the pandemic. A recent survey in Italy has measured the reduction of healthcare access during the period of lockdown due to the pandemic between April and May 2020. 9 About 32.4% of citizens needing health care faced a delay of the scheduled medical service, 1.5% of the interviewed community sample declared to have avoided access to an emergency department when in need (while rows of hours and days were reported for the access to emergencies room, saturated by requests related to Covid) and 5.0% took medications for health problems without any physician’s advice. Patients suffering from chronic conditions were from those who suffered more delays in medical services and were the most prone to self-medication. 9
However, no studies to our knowledge have to date contrasted the point of view of HW and users of health services on the quality of care and respect for the rights of citizens and health workers during the pandemic.
Before the pandemic, a study planned in Sardinia, Italy, and carried out during lockdown, measured how HW perceived the quality of their work; how users perceived the health services received and how satisfied they were with the organization of the health services and respect for the human rights of workers and users in care services.10,11 The study, in accordance with the principles of the Convention on the Rights of Persons with Disabilities and the program of the World Health Organization Quality Rights aimed at comparing the condition of mental health services with other health care services, placing at the center of the assessment the quality of care, the respect for human rights and the active role of service users.12–15
The pandemic and the issues it has brought about to all health care networks has produced a framework in which the evaluation of HW and users in health services not for mental health (which in the initial program was to serve only as a comparison for mental health) has become of more importance.
Starting from a database built for a different main objective but which also allows us to investigate the issues under discussion, the study is conducted to verify the alleged conflicting and/or ambivalent point concerning the health care received by users who use health services and HW8,16 of four outpatient health facilities during the Covid pandemic in an Italian region. In this context, it is useful to investigate and compare both perspectives: the satisfaction of the care received by users and the job satisfaction or perception that HW were satisfied with their work and, finally, the perception that workers “and users” rights were respected.
Methods
Study design
A cross-sectional comparison.
Study sample
A sample of volunteer HW and users from four health outpatient centers working in a hospital of southern Sardinia (pain therapy, dermatology, endocrinology ophthalmology) was recruited. The questionnaires were administered at the collaborating centers with the consent of the head of the health centers to whom the authorization of the ethics committee had been presented. The request to participate was addressed to all HWs, over the course of May 2021. The HW employees from the national health system (“Servizio Sanitario Nazionale”—SSN) working in the four facilities as well as all medical doctors and psychologists in training for achieving the specialization but with a defined responsibility of care, employees of external agencies to the SSN but who provided professional work in the four facilities were recruited for the study. In total 168 HW were selected for the study.
The recruitment of users was carried out on all users who showed up for treatment to the four facilities on the same day of the week of each week of May 2021.
The exclusion criteria for the users were: being on their first visit into that care facility and being in a situation of a serious health crisis they made it difficult and not advisable for the person’s health condition to fulfill the questionnaire and the compilation of the questionnaire. With this methodology, 161 users were contacted and asked to participate.
Study tools
Each participant, after signing the declaration of informed consent (see below), was asked to fulfill:
(a) A questionnaire collecting data about age, gender, place of employment and occupational role. The less frequent professions (e.g. nutritionist, agent of security, or social worker) were grouped into the category “other” to save anonymity, for the same reason the diagnosis of the users was not recorded to avoid that the crossing of the data could allow the identification.
(b) The “Well-Being at work and respect for human rights questionnaire” (WWRR),17,18 both in the user and the patient versions. The WWRR was built and validated inspiring on the World Health Organization’s QualityRights initiative.12–15
The WWRR questionnaire aims to measure the perception of the respect for human rights (for both patients and health workers), the organizational climate at work, and the well-being and satisfaction of care/work. In the first five items, answers are coded according to a 1–6 Likert scale, with a score of 1 is for “Not satisfied at all” and a score of 6 for “Completely satisfied.” The item 6 measures the perception of the adequacy of resources in the workplace, the coding of answers is inverse in item 6 which 1–5 Likert scale, with the score of 1 for “Completely satisfied” and score 5 for “Not satisfied at all” Item 7 inquiries about which categories of health professionals the interviewee thinks it would be most useful to add in his health service, only one possible answer is admitted. A detailed description of the tool is done in the article about validation. 17
Statistical analysis
Statistical analysis was conducted comparing the mean score of answers in each item of health users and workers by means of one-way ANOVA. The answers to item 7, as well the descriptive statistics of the sample, were analyzed by means of non-parametric chi-square tests (with Yates’s correction when needed).
Ethics
The Independent Ethical Committee of the “Azienda Ospedaliera Universitaria di Cagliari” (University Hospital of Cagliari), approved the protocol of the study. The survey was conducted in agreement with the guidelines of the Declaration of Helsinki of 1995 and its revisions. 19 All participants were required to sign an informed consent. It was explained that the data would be collected in an anonymous database and that the participant was free to abandon the research and not complete the questionnaire at any moment he wanted. Any explanation requested by participants was provided by a contact present in each of the participating centers.
Results
The study included 296 participants, 154 HW (52 medical doctors (33.3%), 73 nurses (46.8%), 29 “other” (18.6%)), and 142 users. Of the 168 HW selected, 10 (5.9%) were absent by illness and weren’t contacted, 4 (2.4%) refuse to participate. Of the 161 users contacted 19 (11.8%) refused to participate, no one could not participate due to serious health conditions. The characteristics of the study sample according to sex, age (>49 vs <50), and education (subdivided in degree, high school, <9 years of school education) are shown in Table 1. The two study groups showed unbalanced age, with less old adults (42.2% vs 65.5%, OR = 0.38 (95% CI 0.24–0.61)); by education with more graduates (33.3% vs 15.5%, OR = 2.78 (95% CI 1.58–4.89)), and less people with <9 years of education (18% vs 48.6%) OR 0.24 (95% CI 0.14–0.41) among HW. The distribution by sex was balanced into two sub-sample.
Socio-demographic characteristics of the study samples.

Table 2 shows the comparison of the mean score of answers on items 1–6 of WWRR into two sub-groups. Users show more optimistic answers in all six items than HW. Item 1 (mean score 5.13 ± 1.26 against 4.15 ± 0.98 of mental health workers, F = 52.167, p < 0.0001) shows that users were more satisfied with the health services in which they were cared than how HWs were satisfied with their work, even if HW reached a score of 69.2% of the maximum score available. Item 2, (mean score 4.97 ± 1.12 against 4.09 ± 1.37 of mental health workers, F = 36.248, p < 0.0001) shows that, in average, each user that fulfilled the questionnaire believed that all users of the service were more satisfied with the care received than each HW believed in average, even if HWs reached a score of 68.2% of the maximum score available. Item 3, (mean score 4.85 ± 1.36 against 3.24 ± 1.33 of mental health workers, F = 105,941, p < 0.0001) shows that users were more satisfied with the work organized in the health care facilities in which they were cared than HW, in this item HW reached a score of 54% of the maximum score available. Item 4 (mean score 5.37 ± 1.16 against 4.53 ± 1.30 of mental health workers, F = 34.187, p < 0.0001) shows that users were more satisfied with the level in which the human rights of users were respected in the health facilities than HW did, even if HW reached a score of 75.5% of the maximum score available. Item 5 (mean score 4.94 ± 1.08 against 3.88 ± 1.48 of mental health workers, F = 48.552, p < 0.0001) shows that users were more satisfied with the level in which the human rights of health workers were respected in the health facilities than HW did, even if HW reached a score of 64.6% of the maximum score available. Item 6 concerning the adequacy of the resources for care in the health facilities, shows users were more satisfied than HW (mean score 2.31 ± 0.96 of users against 3.10 ± 0.94, F = 51.127, p < 0.0001). This item which provided an inverse coding with respect to the others, the HW score does reach 58% of the maximum achievable score.
Comparison on answers at item 1–6 of WWRR about health workers and users of mental health services of South Sardinia.
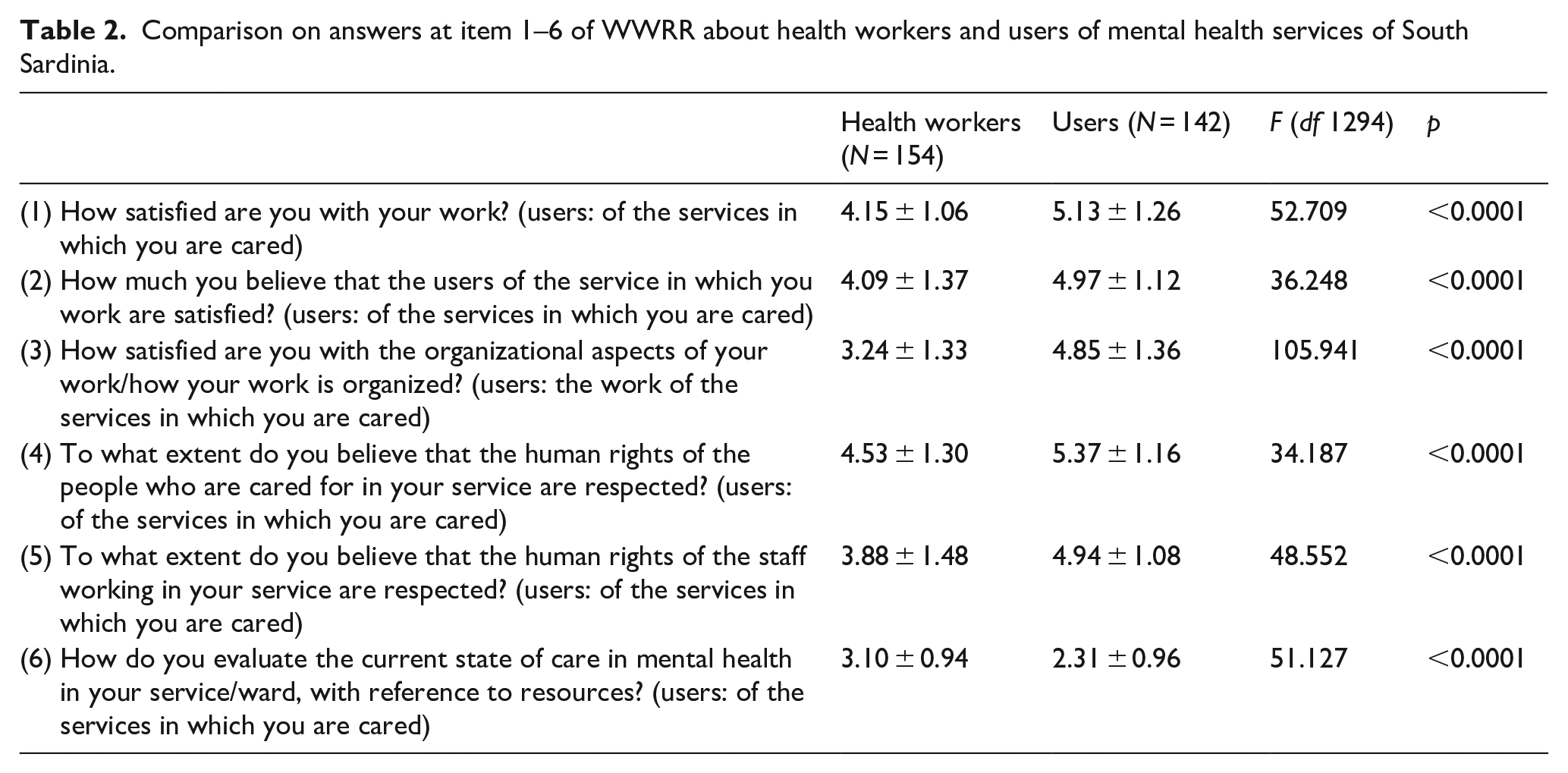
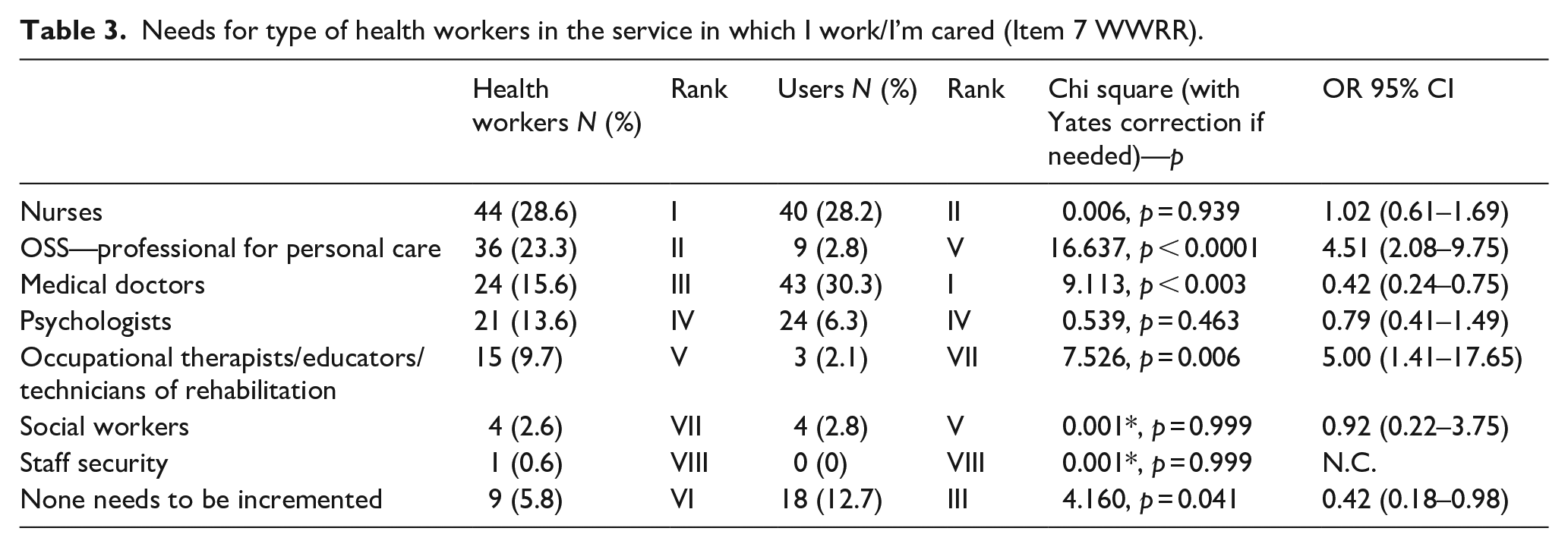
Table 3 shows which professional figures the two groups would like to increase in health services (item 7 of the WWRR). The HW judged as more important to increase the presence (in the order) of nurses, personnel to personal care and doctors, while the users (always in the order) of doctors, nurses but the third choice is the answer that is not deemed necessary to augment any professional figure. In the two groups, differences emerged in the responses regarding “professional for personal care” (HW 23.3% vs users 2.8% OR 4.51, 95% CL 2.08–9.75); Medical Doctors (15.6% HW vs 30.3% users, OR 0.42, 95% CL 0.24–0.75); Occupational Therapists/Educators/Technicians of Rehabilitation (9.7% HW vs 2.1% users, OR 5.00, 95% CL 1.41–17.65); and “None needs to be incremented” (5.8% vs 12.7% users, OR = 0.42, 95% CL 0.18–0.98).
Needs for type of health workers in the service in which I work/I’m cared (Item 7 WWRR).
Discussion
The results of our research highlight a more than sufficient level of satisfaction of HW of their job and of work organization, of the perception that the rights of users and workers are respected in health services, of the adequacy of resources, although in these two aspects the scores achieved by the responses to the WWRR were slightly higher than half the maximum achievable score. Users expressed high levels of satisfaction and higher than HW for the care received, about the belief that all users are satisfied with the care, about the perception of respect for the human rights of users, and HW in health care services. The fact that the samples are not balanced for some variables could question the validity of these results. However, it should be considered that the people who most frequently go to care agencies for pain pathology (i.e. for oncologic disease) o to outpatient endocrinology units (i.e. for diabetes) are very often elderly. Elderly people in Italy have a lower level of education than non-elderly adults 20 and large proportion of HW in Europe have graduated from universities (i.e. medical doctors and nurses). For this reason, we did not conduct the statistical analysis after standardization by the demographic variables, even if unbalanced, because the differences were typical of the population from which the samples were drawn. The data presented in this article are important because they came from the first study in which the point of view of users and HW is compared and because the research was conducted after the first two waves of the pandemic when a strong condition of vulnerability and risk was suspected in all HW even in those not directly involved in Covid treatments. 7
In early 2020, Italy was preparing to tackle the pandemic with moderate optimism about the efficiency and potential responsiveness of its national health system. First-line exponents of politics and science had expressed to media opinions about how the Italian healthcare system would be able to respond adequately because “an excellency worldwide” according to “well-reputed rankings.”21,22 In line with these points of view, even the official plans to combat the pandemic hinted that the emergency could be faced with adequate resources and skills. 23 The reality wasn’t that bright, with the decrease of percentage value of expenses allocated to the healthcare system in the years preceding the pandemic in comparison with other EU countries. The health expenditure in Italy in 2016 has fallen to 8.9% of GDP against 9.9% mean income for other Union European countries, and 11.5% in France, a country with similar mean income, which in that year per capita health expenditure was 3870 Euro against 2475 in Italy. 24 Protests rose by users’ organizations,25,26 but even well-founded issues documented by agencies specialized in health service evaluation. 27
Under the impact of the pandemic, HW became dramatically aware of the organizational weakness and of the scarcity of resources that afflicted the Italian healthcare system, 28 daily facing the scarcity of personal protective equipment and diagnostic tests.15,29
However, the data from this study seem to highlight that there is a sort of mutual trust between users and HW in all care facilities that were evaluated by the research in May 2021. At least in the four facilities for outpatients (dermatology, oculists, pain therapy, and endocrinology) investigated, the perception of organizational well-being, job satisfaction (by HW), or satisfaction with the care received (by users) seems sufficiently high although not at excellent levels, even if the satisfaction of the users is even, and in some questions paradoxically, higher than that of the HW.
However, it must be emphasized that the responses to the WWRR of the same sample of these same structures were compared with those of a sample of mental health workers, a health sector that in Italy has a territorial extra-hospital organization, which was the main objective of the same research. 11 In this comparison, it was found that workers engaged in mental health had codified with greater satisfaction all the items of the WWRR and with scores that touched the maximum values on all items except in item 6 on resource satisfaction. 11 These data had been interpreted as due to the fact that in a moment of particular stress due to the pandemic, HWs working in mental health facilities felt less at risk because working in a community context, in small health facilities well linked to the territory resources for informal and informal support and with well known users (as is now a habit dating back decades in Italy) than those who, working in a hospital, had suffered the most from the impact of the pandemic in terms of greater risk to be infected, to infect their relatives and receiving less support.
It should also be emphasized that the results of our study do not concern hospital units with beds, nor units specifically dedicated to the treatment of Covid, or emergency rooms. 30 Therefore, it is possible that in those frameworks it was detected greater dissatisfaction of users and HW than in units for outpatients. This hypothesis will have to be verified in future studies specifically conducted.
The limitations of this survey were: the self-selected and non-probabilistic nature of the sample without randomization (even if with a really high rate of adhesion); the focusing on only one region of the country and only on outpatient units and finally but probably this was the main limitation, that the protocol wasn’t planning to verify the aim of the present study as the main objective. The study was planned to measure the differences between mental health and non-mental health facilities, then the spread of COVID-19 pandemic made the results in non-mental health facilities, relevant.
The results have underlined that the level of job satisfaction (by HW), the satisfaction of care received (by users) and the perception of respect for human rights in outpatient health services in Italy during the Covid pandemic was higher than expected according to the cited literature concerning HW and their perception. Even if the relatively low score scored by the HW in relation to the satisfaction with the available resources and, above all, for the perception of respect for their human rights could be considered an alarm bell also in this setting.
Thus, this survey may be a starting point for a multicentered, national project conducted on representative samples of different frameworks as inpatients units, emergencies units, and Covid units. This would make it possible not only to define the structures at risk but also to identify the organizational factors of resilience.
Conclusion
In the four facilities for outpatients (dermatology, oculists, pain therapy, and endocrinology) investigated, the perception of organizational well-being, job satisfaction (by HW), or satisfaction with the care received (by users) it seems sufficiently high although not at excellent levels, even if the satisfaction of the users is even, and in some questions paradoxically, higher than that of the HW. The fact that the answers of the HW gave lower scores than those of user (and with the scores to the questions on the perception of respect for the human rights of HW and the adequacy of resources of HW just above average) does not contradict the suspicion raised by many researchers of dissatisfaction and risk of burnout of HW in Italy. However, this level of dissatisfaction and mistrust in the organization was not as marked as expected in the HW of the four outpatient care facilities examined. This survey may be a starting point for a multicentered, national project to be conducted on representative samples of different frameworks as inpatients units, emergencies units, and Covid units. This would make it possible not only to define the structures at risk but also to identify the organizational factors of resilience.
Footnotes
Author contributions
MC Ideas; formulation or evolution of overarching research goals and aims; GC Preparation, creation and presentation of the published work;
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study is supported by Legge 7, Regione Sardegna, 2017, Italy. This article is carried out as part of the research project funded with the resources of the P.O.R. SARDINIA F.S.E. 2014-2020—Axis III “Education and Training, Thematic Objective: 10, Specific Objective: 10.5, Action of the Partnership Agreement: 10.5.12” Call for funding of research projects—Year 2017.
Data and material availability
The research data related to the study would be made available by the corresponding author on reasonable request.
Ethical approval
The Independent Ethical Committee of the University Hospital of Cagliari, Italy approved the protocol of the survey. The study has been carried out in agreement with the guidelines of the 1995 Declaration of Helsinki and its revisions.
Significance for public health
The data underline that the satisfaction for care and respect for human rights in the outpatient health services was higher than expected demonstrating a good level of link between the community health network and other support networks in Italy. The relatively low score by the HWs in relation to the satisfaction with the resources and perception of respect for their human rights could be a wake-up call.