
Abstract
Objective
This investigation examines burden of comorbidity measured by the Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI) among inpatients based on age, sex, and race.
Methods
Cross-sectional analysis of 2012-2018 US NIS datasets. Participants were inpatients 55y+. ICD-9/10 codes for admitting diagnoses were used to calculate disease burden using the CCI and ECI. Unweighted mean CCI and ECI scores were compared across demographic variables.
Results
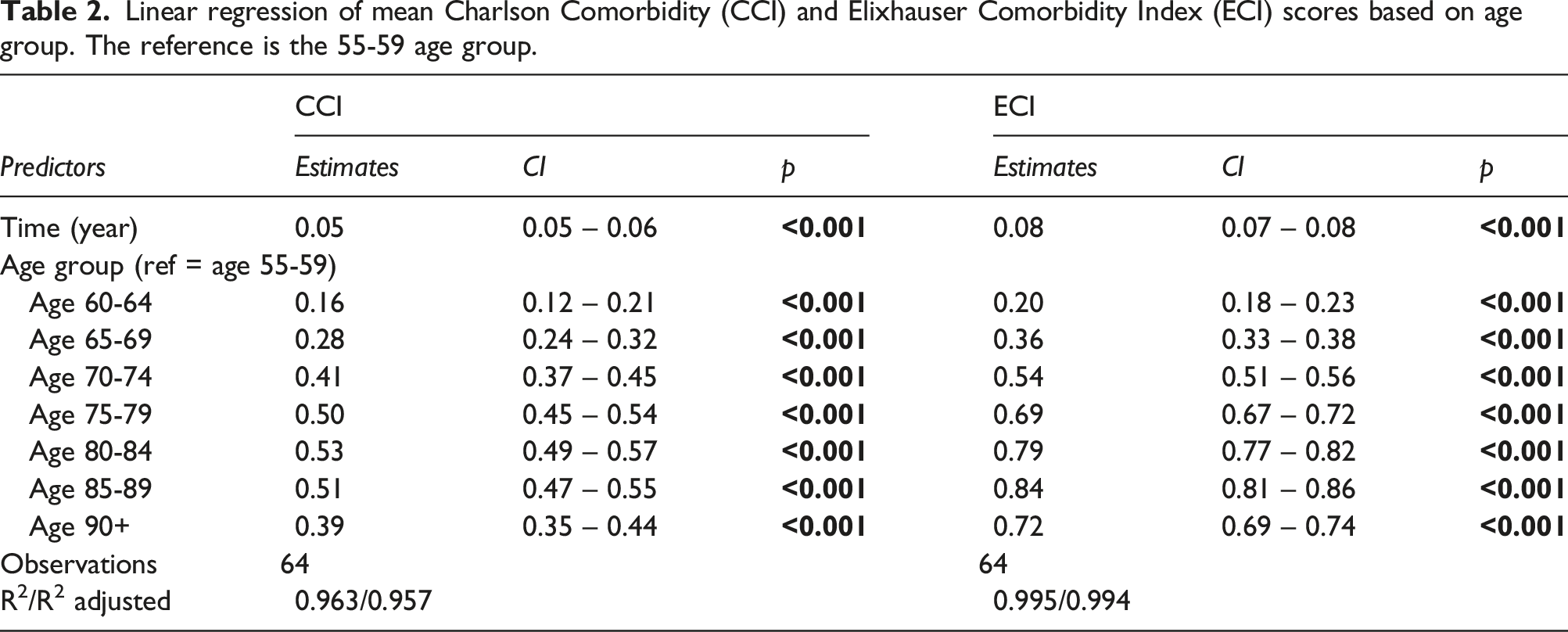
An increase in mean CCI and ECI scores across age, sex, and races (p<.001) was identified. Compared to the youngest age group (55-59y), all age groups had higher mean CCI and ECI adjusting for time (p<.001). Increases were greatest in older age groups until age 80-84 for CCI and 85-89 for ECI. The female group had lower CCI adjusting for time (p<.001) compared to males. There was no difference between sex groups in mean ECI (p=.409). Compared with the White group, all other race groups had higher mean CCI adjusting for time (p<.001). Black inpatients had the highest CCI followed by Native American inpatients. Findings were similar for ECI, but with no difference between Hispanic and White groups (p=.434).
Conclusions
Growing multimorbidity burden among adult inpatients across age, sex, and race supports the continued need for programs for preventing and reducing multimorbidity, especially among communities that experience health inequity including older, Black, and Native American patients.
Keywords
Introduction
Multimorbidity is the experience of having multiple chronic health conditions (or comorbidities) simultaneously. 1 Disease burden arising from multimorbidity has been a focus of researchers and healthcare providers alike due to its impact on patient outcomes and disease management. Studies show that multimorbidity results in increased risk of death, 2 functional decline and disability, 3 diminished quality of life, 1 psychological distress,4,5 polypharmacy 6 and elevated healthcare use and cost.7-9 Additionally, multimorbidity elevates risk of fragmented care and physiological complications affecting disease treatment efficacy.10-12 Evidence supports that multimorbidity prevalence among community-dwelling adults is common and that it is increasing across the age continuum.13,14 Key contributors to this growth are population aging, medical advances enhancing survival of individuals living with chronic health conditions, and changes in health policy. 15 Increasing multimorbidity not only negatively affects patients but also puts strain on the healthcare system through increased costs and utilization.
While many adults with chronic disease suffer from multimorbidity, older hospitalized patients are particularly at risk. Hospitalized patients are commonly sicker than those in the general population, yet, to the best of our knowledge, it has not been investigated if disease burden has changed across time among inpatients. To address this gap, this study aimed to determine the burden of multimorbidity among a large nation-wide sample of adult inpatients (55y+) admitted to American hospitals over a 7-year interval based on age, race, and sex.
Methods
Data source
The study sample was collected from the United States (US) National Inpatient Sample (NIS) database via the Agency of Healthcare Research and Quality (AHRQ). Data from calendar years 2012-2018 were used in the analysis. The NIS is the largest national all-payer inpatient care database housing data from over 4,000 non-federal hospitals from across the US. 16 The data collected each year and stored in the NIS datasets originated from hospitals across the US that voluntarily participated in providing data to the AHRQ for that particular year and represents more than 97 percent of inpatient discharges from community hospitals in the US. 16 While each year’s data provides a national sample, it could be originating from different hospitals.
The NIS datasets include hospital admission information, demographic information, and primary and secondary diagnoses for patients admitted from short and long-term care and rehabilitation facilities as well as the community. The data on diagnoses are provided as International Classification of Disease (ICD) 9th and 10th revision codes. 17 ICD code data for primary and secondary discharge diagnoses were used in analysis. ICD-9 codes were used to calculate comorbidity index scores for 2012-2014, and Q1-Q3 of 2015. ICD-10 codes were used to calculate scores for Q4 of 2015 and 2016-2018. The year 2015 is represented in 2 parts, 2015-Q1-3 and 2015-Q4, to ensure that all data was captured for this year despite the ICD-9 to -10 code switch in 2015-Q4. All study procedures for this retrospective cross-sectional analysis were exempted by the Institutional Review Board, thus informed consent was not needed to complete this study.
Study population
The population of interest for this analysis was US inpatients aged 55y+ due to the increased disease burden experienced by the older adult population. 18 We extracted ICD codes, race, and sex data for all inpatients 55y+ for each year, 2012-2018. The total combined sample size for all inpatients 55y+ was N=24,947,829. The mean CCI and ECI scores were calculated as described above and stratified by age group, race group, sex group, and year. Age grouping used 5-year intervals (55-59; 60-64; 65-69; 70-74; 75-79; 80-84; 85-89; and 90y+), race grouping included White, Black, Hispanic, Asian/Pacific Islander, Native American, and sex grouping included male and female.
Measures of disease burden
Two common comorbidity measures were used to quantify disease burden among hospitalized patients using ICD codes for each year across age groups, sex, and race. The Charlson Comorbidity Index (CCI) 19 identifies 17 conditions (acute myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular, dementia, chronic pulmonary disease, rheumatoid arthritis, peptic ulcer disease, mild liver disease, diabetes, diabetes with complication, hemiplegia or paraplegia, renal disease, cancer (any malignancy), moderate or severe liver disease, metastatic solid tumor, AIDS/HIV) and was used along with the Elixhauser Comorbidity Index (ECI) 20 which identifies 31 conditions (congestive heart failure, cardiac arrhythmias, valvular disease, pulmonary circulation disorders, vascular disorders, uncomplicated hypertension, complicated hypertension, paralysis, other neurological disorders, chronic pulmonary disease, uncomplicated diabetes, complicated diabetes, hypothyroidism, renal failure, liver disease, peptic ulcer disease, AIDS/HIV, lymphoma, metastatic cancer, solid tumour (without metastasis), rheumatoid arthritis / collaged vascular disease, coagulopathy, obesity, weight loss, fluid and electrolyte disorders, blood loss anemia, deficiency anemia, alcohol abuse, drug abuse, psychoses, depression). Both indexes combine the number of conditions yielding a summary score with higher scores indicating increased multimorbidity and risk for poorer health outcomes including increased length of stay, 30-day readmission, and mortality.21-24 Conditions for each index were not weighted but provide a count of the number of comorbidities as an overall assessment of disease burden.
Statistical analysis
The characteristics of the study sample were described using mean (95% CI) for continuous variables (age) and frequency (95% CI) for categorical variables (age group, sex, race). Differences between categorical variables were assessed using Pearson’s chi-square test. CCI and ECI summary scores were calculated using primary and secondary admission diagnoses using the R survey package, version 3.5.1. The summary scores were presented as means and SDs. Linear regression was used to examine the relationship between mean CCI or ECI scores with demographic characteristics (age, sex, race) and time.
Results
Characteristics of the sample population by year are presented. Mean age and mean Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI) scores by year, and number of hospitalizations per year based on age group, race group, and sex group.

Linear regression of mean Charlson Comorbidity (CCI) and Elixhauser Comorbidity Index (ECI) scores based on age group. The reference is the 55-59 age group.
Linear regression of mean Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI) scores based on sex group.

Linear regression of mean Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI) scores based on race group. The reference is the White group.

Compared to the male group, the female group had significantly lower mean CCI scores when adjusting for time (p<.001). Male group mean CCI scores increased peaking at 2.08, SD=1.54, while the female group increased peaking at 1.86, SD=1.47 (Supplemental Table 3). While there was a significant increase in mean ECI scores for male and female groups, there was no significant difference between the groups (p=.409; Table 3). Male group mean ECI scores increased peaking at 4.15, SD=2.24 while the female group increased peaking at 4.12, SD=2.24 (Supplemental Table 4).
All race groups had a significant increase in mean CCI and ECI scores (p<.001, Table 4). Compared to the White group, the Black/African American, Hispanic, Asian/Pacific Islander, and Native American groups had significantly higher mean CCI score adjusting for time (p<.001, Table 4). Findings were similar for mean ECI scores, except there was no difference between Hispanic and White groups (p=.434). The Black/African American group had the highest mean comorbidity scores (CCI 2.32, SD=1.55; ECI 4.54, SD=2.19) followed by the Native American group (CCI 2.17, SD=1.51; ECI 4.27, SD=2.18). The White group had the lowest mean CCI score each year analyzed while Asian/Pacific Islander group had the lowest mean ECI score each year (Supplemental Tables 5-6).
Discussion
Measuring multimorbidity provides an understanding of a patient’s disease burden and risk for outcomes including death, disability, and reduced quality of life.1-3 This study used unweighted mean Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI) scores to quantify multimorbidity among a large adult (55y+) inpatient sample for years 2012-2018. While evidence of change in multimorbidity among community-dwelling adults, and inpatients of specific races, has been reported previously,25,26 to our knowledge this is the first report of change in multimorbidity among a national sample of adult inpatients using two validated measures across age, sex, and race. The findings presented show that multimorbidity increased over time in this hospitalized cohort and there were unique trends across age, sex and race. It is possible that the results presented reflect changes to the hospital system policies restricting hospitalization to only the sickest patients each year analyzed. If only patients with higher multimorbidity were admitted, it might appear that hospitalized patients are sicker. Yet, there is strong community-based evidence supporting that multimorbidity is increasing among US adults, so the possibility that multimorbidity among inpatients is also increasing is likely considering most patients admitted came from the community.25,27
Evidence that older age is associated with higher rates of multimorbidity has been described previously.25,28,29 Our study generally agreed with prior work, we showed that most older groups had higher mean comorbidity scores than the younger groups except for the 90y+ group. However, we also identified that most hospitalizations in the sample were among the younger age groups and declined among the 80-84y and 85-89y age groups over time. This is consistent with initiatives for enhancing community-based healthcare services for older adults such as the Geriatric Resource Teams and the Community Aging in Place to aid in managing complex care needs outside of the hospital to reduce hospitalization.30,31 Future research should examine this topic to confirm a causal effect. Our analysis also uncovered a distinct increase in mean CCI score among the 90y+ group during the year 2015 following the ICD version 9 to version 10 code transition. This was largely due to the increased rate of hospitalization for dementia in this group (9.9% in 2015Q-3 to 34.6% in 2015Q4; data not shown). It is possible that change in coding for dementia contributed to this increase because younger age groups also showed a sharp increase after the ICD code transition. Furthermore, another study showed change in prevalence for multiple neurological conditions with this code transition. 32
Assessment of sex and multimorbidity over time revealed that there was an increase across male and female inpatients. Male inpatients had higher mean CCI scores than female inpatients each year. Yet this was not observed using the mean ECI, likely, because the conditions listed for each tool are different.19,20 Other research identified that women were more likely to report having multimorbidity than men. 13 Importantly, this prior study included women 18y+ and determined that lower income and smoking contributed to this finding. Our study did not differentiate female inpatients based on socio-demographic or behavioral risk factors, which could account for this difference. Additionally, females composed a decreasing proportion of overall hospitalizations from 2012-2018. Women are known to visit ambulatory care more often than men, 33 thus these results could signify that females are improving management of chronic disease using out-of-hospital care programs.
Research aiming to better understand racial health disparities has included a focus on assessment of multimorbidity burden among underrepresented groups. 34 Prior studies among community-dwelling adults showed that Black individuals experience multimorbidity earlier in life and are more likely than White individuals to have multisystem multimorbidity.34,35 Another study showed that Native American, Hispanic, and Black individuals are at increased risk of multimorbidity compared to White individuals. 36 The authors indicate that barriers to receiving healthcare and racial discrimination contribute to these findings and that better screening and care management are needed to reduce multimorbidity in minority populations. 36 Our findings further support the need for improved racial health equity by showing that the greatest increases in multimorbidity in the sample were among Black and Native American inpatients.
A key strength of this study is that, to the best of our knowledge, this is the first analysis of change in multimorbidity among US adult inpatients using two validated assessments to quantify disease burden. While the weighted CCI and ECI are often used to predict risk, our group used unweighted values for each comorbidity of the CCI and ECI to ensure the summary scores calculated provided an overall assessment of disease burden. Other work has examined change in multimorbidity by categorizing inpatients as multimorbid if they had 3+ conditions but without calculating a comorbidity summary score. 26 Furthermore, our analysis involved a very large and racially diverse sample that spanned hospitals across the US providing a strong assessment of the US adult inpatient population at large. Despite the strengths of this analysis, some limitations should be noted. This study used an inpatient sample dataset collected prior to the COVID-19 pandemic. The pandemic resulted in a shift to using telemedicine for outpatient services, which may have reinforced structural barriers to receiving community-based services in groups already experiencing health disparities thus influencing disease burden and hospitalization in these groups. 37 Additional research should examine changes to multimorbidity burden across demographic variables before and after the pandemic among inpatients to assess the impact. Furthermore, since the NIS datasets are de-identified, we are unable to determine if the same patient was admitted more than once to the same hospital during a single year of this study. Additionally, the hospitals that provided data for the NIS datasets from 2012-2018 might have been different, though each annual dataset provided a representative sample for the US inpatient population for that year. Finally, the NIS dataset categorizes sex as male or female, and thus does not provide information regarding transgender, non-binary, or other gender non-conforming individuals, precluding assessment of multimorbidity among these groups.
Conclusions
This study highlights that multimorbidity significantly increased overtime among a large sample of male and female adult inpatients of diverse races in the US. The findings highlight that multimorbidity increased most among older adult inpatients and minority underserved groups, especially the Black and Native American groups, supporting the need for continued growth of geriatric care and programs that aim to provide health equity to minority communities.
Supplemental Material
Supplemental Material - Changes in multimorbidity among hospitalized adults in the US
Supplemental Material for Changes in multimorbidity among hospitalized adults in the US by Christine Loyd, Lauren Picken, Richelle Sanders, Yue Zhang, Richard E. Kennedy, and Cynthia J. Brown in Journal of Multimorbidity and Comorbidity
Footnotes
Author contributions
CL – conceptualization, data curation, methodology, funding acquisition, investigation, supervision, resources, validation, project administration, visualization, writing – original draft, writing – review and editing, final draft approval. LP – investigation, data curation, writing- original draft, writing – review and editing, final draft approval. RS – investigation, writing- original draft, writing – review and editing, final draft approval. YZ – data curation, formal analysis, methodology, software, writing – original draft, final draft approval. REK – conceptualization, data curation, formal analysis, investigation, methodology, software, resources, validation, visualization, supervision, writing- original draft, writing- review and editing, final draft approval. CJB - conceptualization, methodology, validation, resources, writing- original draft, writing- review and editing, final draft approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The NIS databases are publically available and can be purchased from the US Agency for Healthcare Research and Quality.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.