
Abstract
Background
Duchenne muscular dystrophy (DMD) is marked by cardiac and skeletal myopathy with disparate onset and progression suggesting distinct pathophysiologies. Nontargeted proteomics may elucidate the different disease pathways underlying skeletal muscle and cardiomyopathy progression and identify proteins that improve DMD risk stratification.
Methods and results
Sixty subjects were enrolled; 56 underwent cardiac magnetic resonance to determine left ventricular ejection fraction, late gadolinium enhancement, and myocardial circumferential strain. Of the 60 patients enrolled, 51 underwent quantitative muscle testing and 33 underwent actigraphy. Aptamer-based technology (SomaScan) evaluated 1128 proteins in plasma. The correlations between serum protein levels and cardiac or skeletal muscle indices were tested using a Spearman correlation test followed by multiple testing correction yielding q-values. The median age was 15.0 years (12.7–17.9 interquartile range). Of 1128 proteins analyzed, 208 correlated with only cardiac indices; 14 correlated with only skeletal muscle indices; 10 proteins correlated strongly with both indices. Protein functions included (1) calcium regulation, (2) cardiac remodeling, (3) cell homeostasis, (4) fibrosis, (5) inflammation, (6) lipid regulation, and (7) other.
Conclusion
Our nontargeted proteomics study identified serum biomarkers correlating with skeletal and cardiac progression in DMD. Candidate proteins—some uniquely associated with skeletal or cardiac indices and others overlapping—offer promising leads for studies to improve risk stratification and guide targeted therapies in DMD.
Introduction
Duchenne muscular dystrophy (DMD) is the most common neuromuscular disorder in boys, with an incidence of approximately 20 per 100,000 live male births. 1 This disorder arises from mutations in the DMD gene, resulting in reduced or absent dystrophin protein, which leads to increased muscle breakdown, progressive skeletal muscle weakness, and cardiomyopathy. 2 Affected individuals typically lose ambulation in early adolescence and often require assisted ventilation by late adolescence. 3 Notably, the progression of skeletal muscle degeneration does not directly correlate with cardiomyopathy; some patients progress in parallel, while others have divergent progression of skeletal muscle and cardiac disease. 4 This suggests either distinct pathophysiological mechanisms or protective mechanisms in some patients. Due to limited mobility, patients may not exhibit cardiomyopathy symptoms until later stages, making regular cardiac surveillance essential for early identification of those at risk. Detecting early-onset cardiomyopathy enables timely, targeted therapeutic interventions.
Currently, cardiac monitoring in DMD is primarily imaging-based, utilizing echocardiography and cardiac magnetic resonance imaging (CMR). However, both modalities have limitations compared to plasma biomarkers. Echocardiography is often constrained in DMD patients due to poor acoustic windows, which hinder accurate tracking of cardiac function. CMR provides a more accurate and reproducible assessment of cardiac function, with recent studies showing that rates of change in left ventricular ejection fraction (LVEF), 5 midcircumferential strain, and ventricular volumes on CMR correlate strongly with mortality risk in DMD. 6 However, CMR is costly, cumbersome, can lead to patient discomfort, and frequently requires patients to travel long distances to access pediatric CMR facilities.
Given the limitations of imaging-based cardiac monitoring, there has been a strong interest in identifying blood biomarkers that can assess cardiac function in DMD. Traditionally, this has been performed using focused, biologically plausible analyses. Cardiac biomarkers, such as N-terminal pro-b-type natriuretic peptide, brain natriuretic peptide, and troponin, are often not elevated until the later stages of cardiac disease. 7 Targeted approaches have identified several promising biomarkers, including Suppression of Tumorigenicity 2 (ST2). 8 However, given the significant overlap between groups and the influence of age on ST2, further validation of ST2 as a marker of DMD cardiomyopathy is necessary. Our group has previously demonstrated that matrix metalloproteinase-7 (MMP-7) correlates inversely with LVEF (ρ = −0.40, p = 0.012). 9 However, MMP-7 also appears to be elevated in the setting of progressive skeletal muscle disease. In addition, a focused approach to detecting biomarkers of DMD disease progression is costly and time-consuming. Advances in proteomics now enable the exploration of over a thousand biomarkers with small sample volumes, providing an opportunity to perform a nontargeted analysis to better explain the variable pathophysiology of skeletal and cardiac myopathies in DMD and improve clinical management of cardiomyopathy in DMD. 10 We hypothesized that a nontargeted proteomics analysis in a comprehensively phenotyped cohort of DMD patients could help determine similarities and differences in the protein expression pattern of DMD skeletal muscle and cardiomyocytes.
Methods
Enrollment
This cross-sectional study was approved by the Vanderbilt Institutional Review Board (Study approval numbers: 120929; 139979; 140776). DMD subjects were enrolled from the neuromuscular cardiology clinic from 2012 to 2018. Informed consent/assent was obtained for blood collection. All subjects had a clinical diagnosis of DMD confirmed with either genetic testing or a muscle biopsy. Patients with inadequate blood samples or with additional cardiac diagnoses that could confound biomarker analysis were excluded from the cohort. Sixty DMD subjects underwent blood collection and subsequent SOMAScan analysis. Four subjects did not undergo CMR and were excluded leaving the total subjects included in the study to be 56. Given difficulties with breath-holds in younger children, the youngest age enrolled was 7 years. There was no upper age limit set to increase the range of cardiac disease severity. Pertinent clinical data were collected from the subjects and from their electronic medical records. Enrolled DMD subjects underwent blood draw, CMR, quantitative muscle testing (QMT), and actigraphy within a short span of time (most on the same day).
Proteomics analysis
Plasma samples collected at time of CMR were analyzed using the SomaLogic SomaScan Assay 1.3k, which evaluates 1310 proteins. 10 The SOMAScan assay uses chemically modified single-stranded DNA aptamers that are optimized to enhance binding to protein epitopes with high specificity. Each protein has its own targeted SOMAmer reagent that functions as an affinity binding reagent that is subsequently quantified on a hybridization chip. Quality control procedures were then performed as per SomaLogic's quality control system, with 1128 proteins passing quality control testing. Protein levels were quantified using relative fluorescence units, reflecting relative expression across a broad dynamic range capable of detecting proteins down to femtomolar sensitivity.
CMR protocol
DMD subjects underwent CMR on a 1.5 Tesla Siemens Avanto or Avanto Fit scanner (Siemens Healthcare Sector, Erlangen, Germany). CMR protocol was performed as previously described. 11 In brief, balanced steady-state free precession cine imaging was used to obtain volumes and function. 12 Myocardial tagging was performed in the short axis at the base, level of the papillary muscles, and apex using a segmented k-space fast gradient echo sequence with electrocardiogram-triggering as previously described. 9
Intravenous gadolinium contrast (gadopentate dimeglumine, Magnevist®, Bayer Healthcare Pharmaceuticals, Wayne, NJ, USA, at a dose of 0.2 mmol/kg or gadobutrol, Gadavist®, Bayer Healthcare Pharmaceuticals, Wayne, NJ, USA, at a dose of 0.15–0.2 mmol/kg) was administered through a peripheral intravenous line. Late gadolinium enhancement 13 was assessed using single shot, segmented inversion recovery balanced steady-state free precession (bSSFP) with optimized inversion recovery, and phase sensitive inversion recovery bSSFP with an inversion time of 300 ms.
CMR postprocessing
All CMR postprocessing was performed blinded to clinical data by an image analyst with all analyses verified by an experienced cardiologist (JHS). Ventricular volumes and function were calculated using Medis QMass (MedisSuite 2.1, Medis, Leiden, The Netherlands). The presence or absence of late gadolinium enhancement (LGE), as well as location using the standard 17-segment model, 14 was qualitatively assessed. LGE severity was assigned using a modification of the global severity score reported by Menon et al., as previously described.9,15 In brief, the score was calculated using all available LGE images and ranged from 0 (no LGE) to 4 (severe LGE); reproducibility of this method has been previously demonstrated. 16 Percent LGE was calculated using the full-width half-maximum (FWHM) technique on the phase sensitive inversion recovery images as per our labs standard protocol. Analysis of myocardial tagged images was performed using harmonic phase methodology (Myocardial Solutions, Morrisville, NC) as previously described to calculate circumferential strain 17 at the base, mid, and apex and global circumferential strain (ECC). 18
Skeletal muscle indices
QMT
The QMT assessment was performed at the time of CMR and blood draw using MicroFET2 handheld dynamometer (Hoggan Scientific, Salt Lake City, UT, USA). Three values were analyzed: arm QMT, leg QMT, and total QMT. Arm QMT was the sum of flexion and extension values for both elbows in pounds. Leg QMT was the sum of flexion and extension values for both knees. Total QMT score was the sum of arm and leg QMT. While QMT typically increases linearly with age in healthy male children, in patients with DMD, it often plateaus around 7.5 years of age and then begins to decrease. 19 To account for this age-related discrepancy, QMT values were partially adjusted by indexing to age in subjects less than 20 years old and in subjects older than 20 years of age, QMT scores were divided by Killian et al. 20 This method was used as z-scores are not available for QMT. 20 This indexing of QMT scores helped account for the previously progressive loss of strength with age in patients with DMD, in contrast to the progressive gain in children without DMD.19,21
Accelerometry
Participants in the study wore triaxial accelerometers (GT3X+, ActiGraph, Pensacola, FL) on their wrist during their normal living activities for 7 days following CMR, blood draw, and QMT data. Data were collected 24 h a day, including during sleep and water-related activities. A recording was considered valid if it included ≥3 valid days with ≥2 weekdays and ≥1 weekend day, each with ≥6 h of monitor wear from 7:00am to 10:00pm. 22 Awake status was assessed using a validated algorithm for bedrest/wake identification. 23 Accelerometry data were collected at frequency of 30 Hz (30 observations per second for each axis) and were converted to vector magnitude (VM) counts calculated as a square root of the sum of squared recordings from the accelerometer axes using Actilife software (ActiGraph, Pensacola, FL). Total VMs and awake VMs were used for our analysis.
Statistical analysis
Demographics and clinical findings at time of CMR are described as median and interquartile range (IQR) or N (%). Spearman correlations were used to evaluate the correlation between pertinent cardiac markers (LVEF, strain, and percent LGE) and protein levels. Skeletal muscle biomarkers (arm QMT, leg QMT, total QMT, total VMs, and VMs awake) were also compared to protein levels. A Wilcoxon rank sum was used to evaluate differences in proteins for those with and without LGE. A total of 9104 Spearman correlations were conducted, corresponding to 1128 proteins tested against eight clinical indices (five skeletal and three cardiac measures). Benjamini–Hochberg corrected p-values (q-values) to correct for multiple comparisons. Significance was set at q-value <0.05. For the 10 proteins with the strongest correlation with LVEF and QMT, a linear regression analysis was performed to evaluate the effect of covariates; given the limited sample size, a total of three variables was chosen to avoid overfitting the models. Linear regression with LVEF as the outcome measure included age, use of cardiac therapies, and protein levels as the independent variables. Linear regression with QMT as the outcome measure included age, use of corticosteroids, and protein levels as the independent variables. Analyses were performed using R version 4.4.2.
Results
Demographics
Of the 56 DMD subjects with CMR included in this analysis, 51 underwent QMT and 33 had valid accelerometry data. Demographic data for these patients are reported in Table 1. The median LVEF was 56.5%, IQR (48%–59%). Figure 1 shows the age and LVEF distribution of our cohort. Most subjects (n = 51, 91%) had LGE present on CMR. Figure 2 shows the age and total QMT score distribution for our cohort.
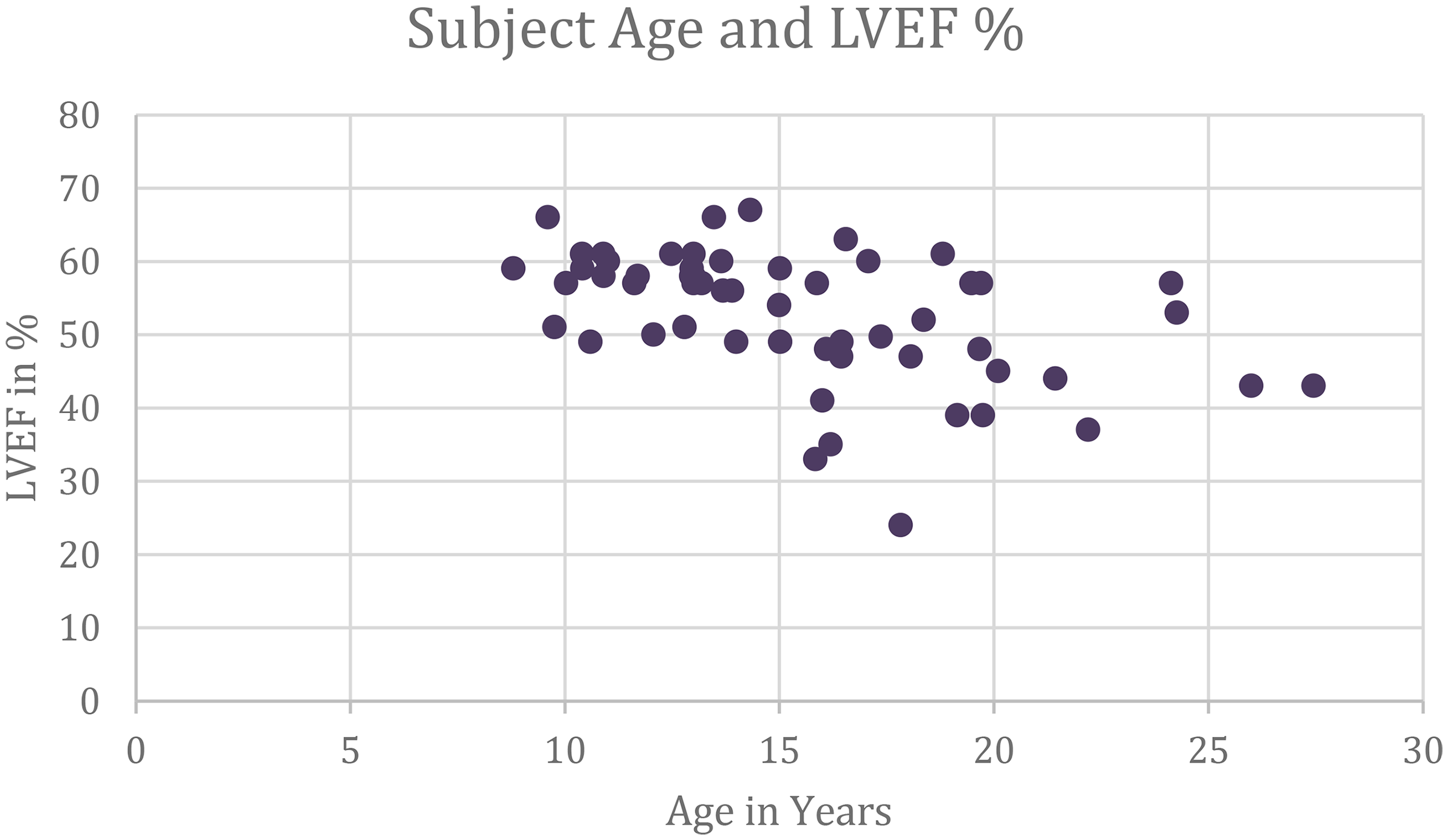
The distribution of subjects age and Left Ventricular Ejection Fraction.
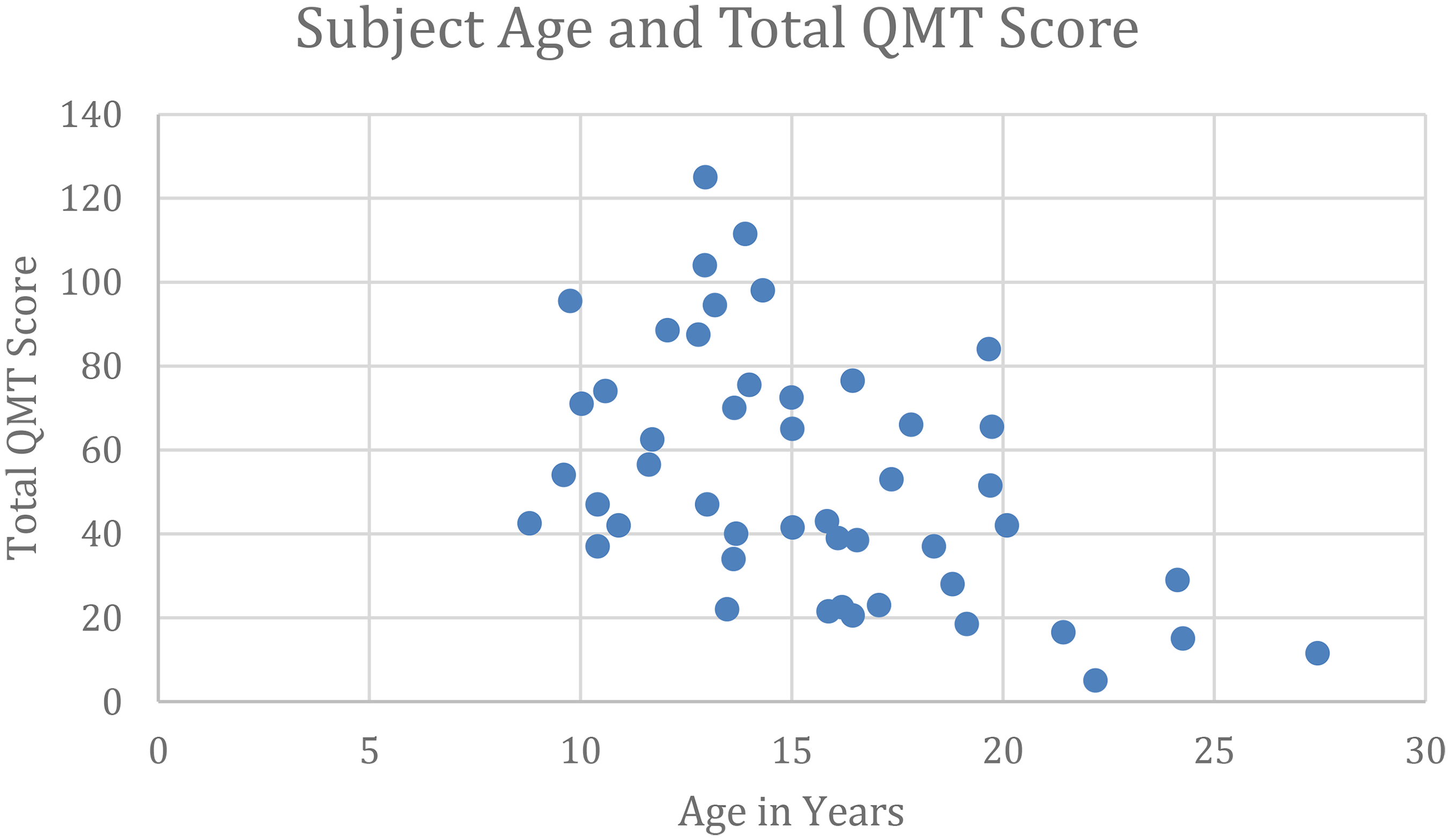
The distribution of subjects age and Total Quantitative Muscle Testing.
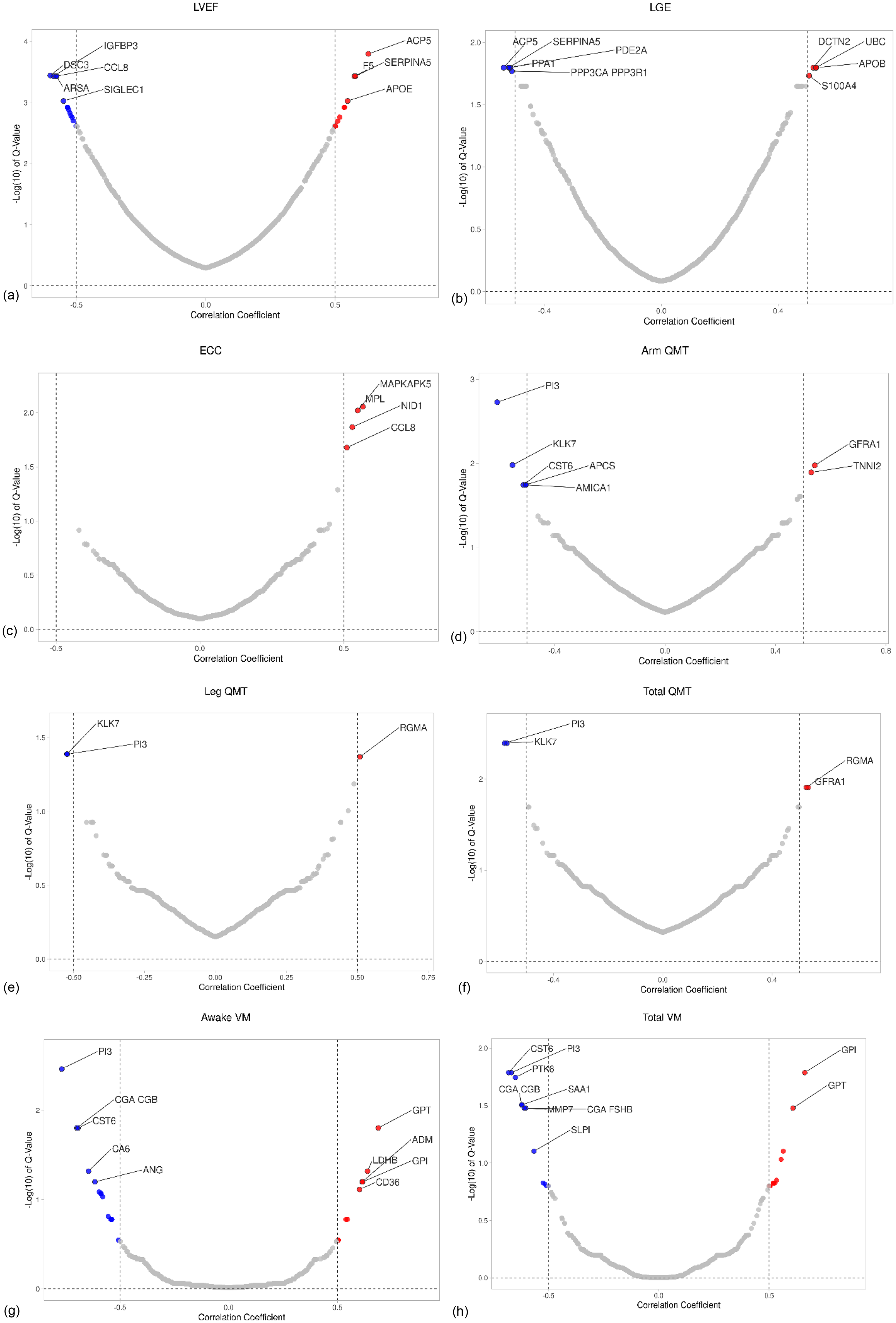
Demographics at time of blood draw (n = 56).
Proteomics analysis
Proteins correlating with indices for cardiomyopathy
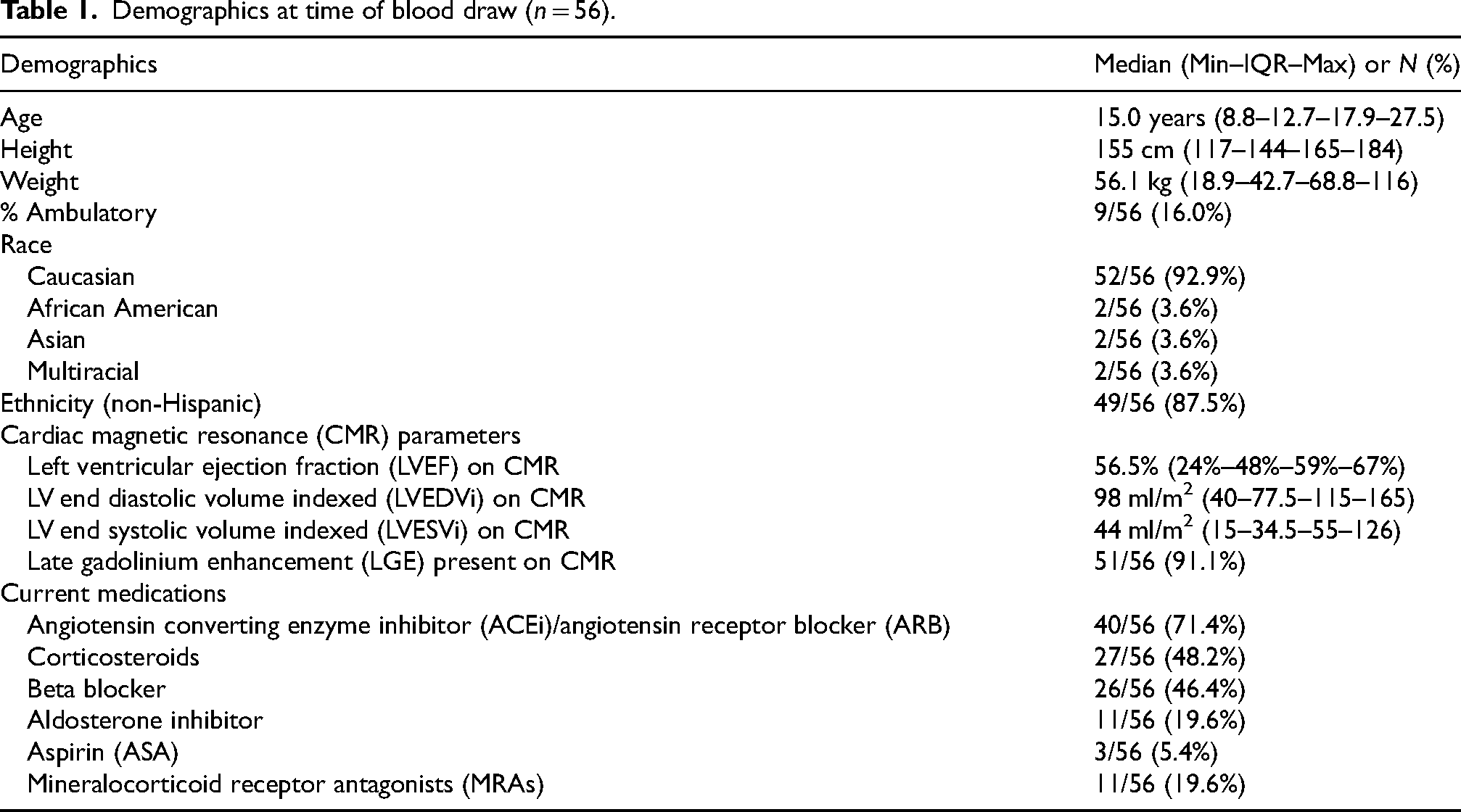
After quality control testing, 1128 out of 1310 proteins were included in the final analysis. Two-hundred-six proteins were significantly correlated with LVEF (ρ > 0.6 or ←0.6: 2, ρ = 0.4–0.6 or = −0.4 to 0.6: 95, ρ < 0.4 or >−0.4:109) (Figure 3(a)), while 54 proteins were significantly different in those with and without LGE (Figure 3(b)); only four proteins were significantly correlated with ECC (ρ = 0.4–0.6 or = −0.4 to 0.6: 4) (Figure 3(c)) and no proteins correlated with FWHM. In total, 218 proteins were significant for at least one of the cardiac indices (LVEF, ECC, or LGE) (Supplemental Table 1, proteins with lowest q-values included in Table 2). No proteins were significantly correlated with all three markers of function and fibrosis (LVEF, ECC, and LGE). However, four proteins were significantly correlated with both LVEF and ECC, and 42 were significantly correlated with LVEF and LGE (Figure 4).
Legend: scatter plot showing association between the correlation coefficient and the −log(10) of the q-values of serum proteins across cardiac and musculoskeletal indices. The x-axis represents the Spearman correlation coefficient between each protein and the corresponding cardiac or musculoskeletal index. The y-axis represents the -log10 transformed q-value. Each point represents a single protein measure by the SOMAScan platform. Proteins with significant q-values are denoted with green dots.
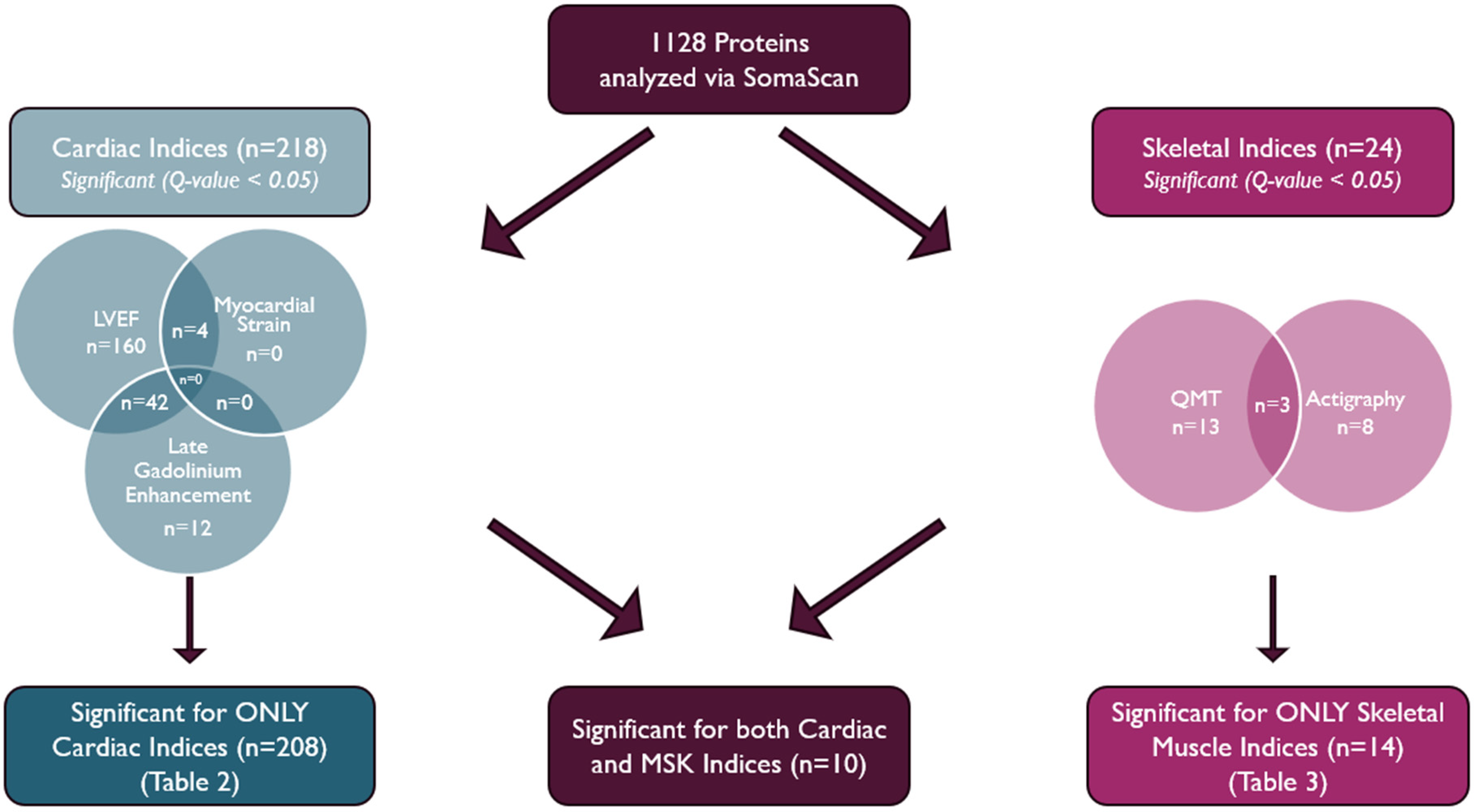
The number of proteins significant for only Cardiac indices, proteins significant for both Cardiac and musculoskeletal indices, and proteins significant for only musculoskeletal indices.
Top proteins that correlated significantly with cardiac muscle disease indices, LVEF, Ecc, or LGE.
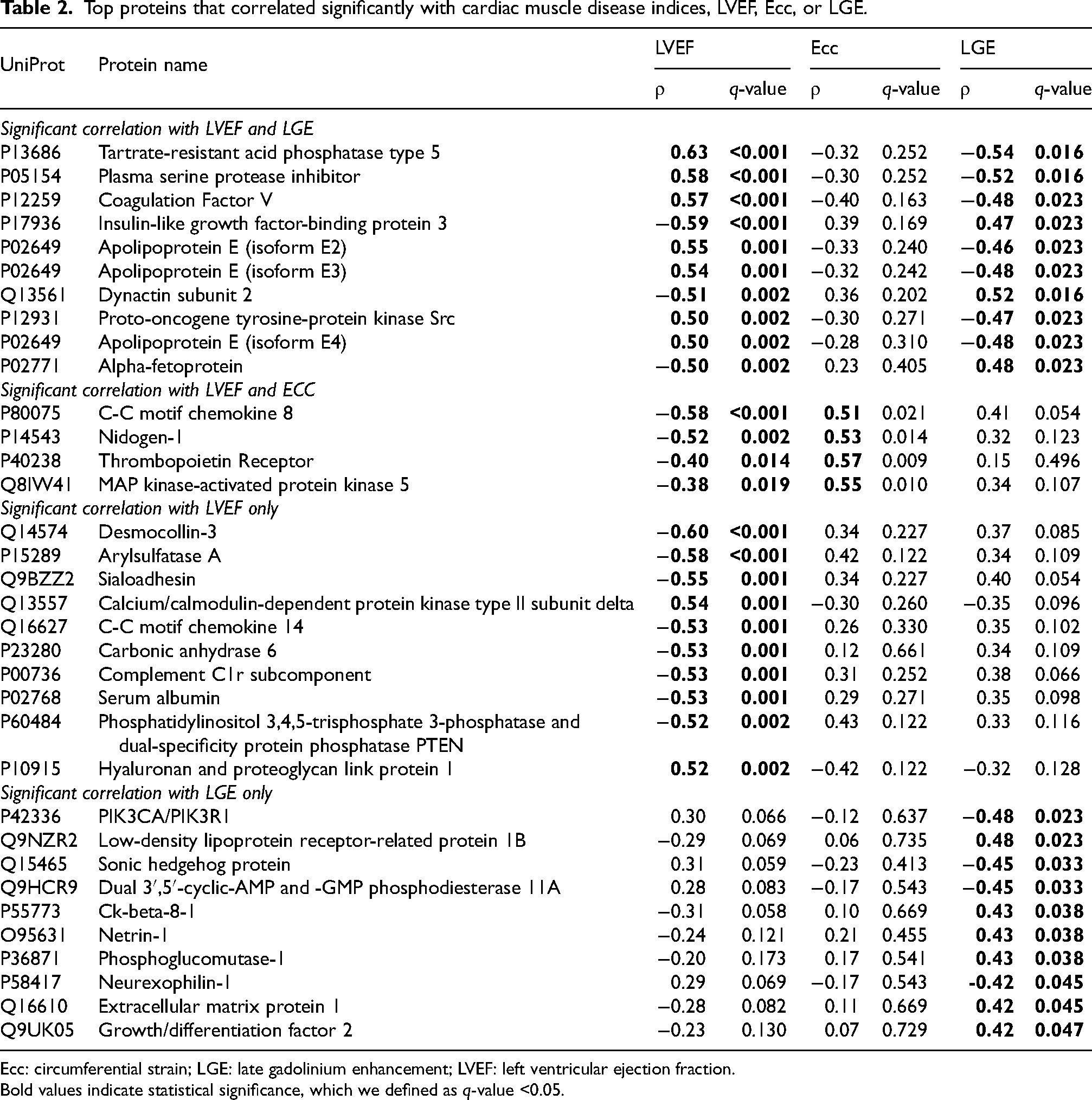
Ecc: circumferential strain; LGE: late gadolinium enhancement; LVEF: left ventricular ejection fraction.
Bold values indicate statistical significance, which we defined as q-value <0.05.
Proteins correlating with indices for skeletal myopathy
Of the 1128 proteins, 24 proteins were significant for at least one skeletal muscle index (QMT or accelerometry). Sixteen were significant for one of the QMT parameters (arm QMT, leg QMT, or total QMT; Figure 3(d) to (f)) (ρ > 0.6 or <−0.6: 1, ρ = 0.4–0.6 or = −0.4 to 0.6: 15), and 11 were significant for one of the accelerometry parameters (awake VMs or total VMs; Figure 3(g) and (h)) (ρ > 0.6 or <−0.6: 11) (Supplemental Table 2). Three were significantly correlated with both QMT and accelerometry parameters. (Table 3).
Proteins that correlated significantly with both QMT and actigraphy VMs.
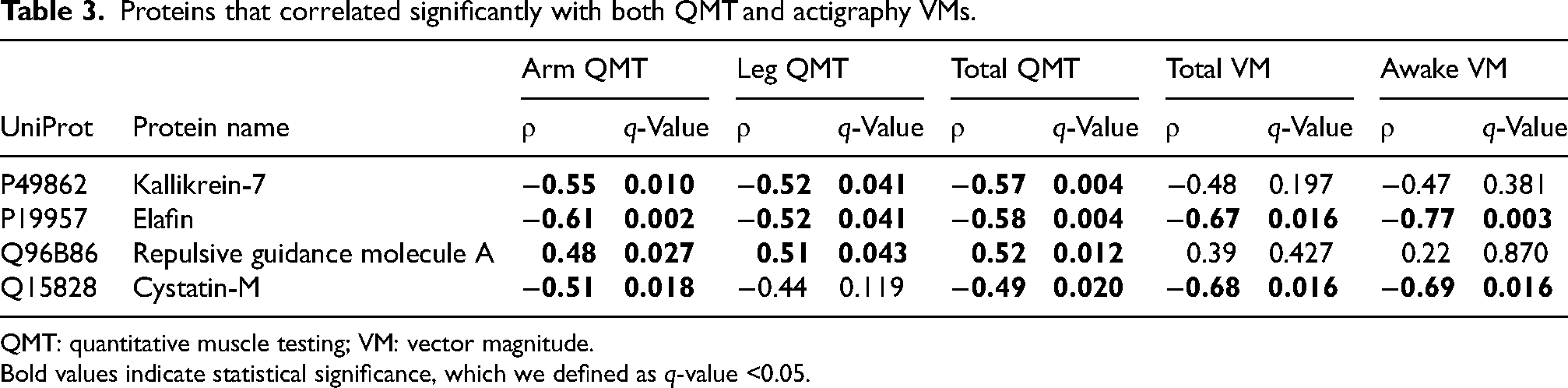
QMT: quantitative muscle testing; VM: vector magnitude.
Bold values indicate statistical significance, which we defined as q-value <0.05.
Proteins correlating with both cardiac and skeletal muscle biomarkers
Ten proteins were identified that were significant for at least one cardiac index and one skeletal muscle index: Carbonic anhydrase 6 (UniProt: P23280) (LVEF ρ =−0.53, Awake VM ρ = −0.65), Bone sialoprotein 2 (UniProt: P21815) (LVEF ρ = 0.50, Arm QMT ρ = 0.45), Cystatin-M (UniProt: Q15828) (LVEF ρ = −0.45, Arm QMT ρ = −0.51, Total QMT ρ = −0.49, Total VM ρ = −0.68, Awake VM ρ = −0.69), Serum amyloid P-component (UniProt: P02743) (LVEF ρ = −0.45, Arm QMT ρ = −0.51, Total QMT ρ = −0.46), Kallikrein-7 (UniProt: P49862) (LVEF ρ = −0.43, Arm QMT ρ = −0.55, Leg QMT ρ = −0.52, Total QMT ρ = −0.57), alanine aminotransferase (ALT) (UniProt: P24298) (LVEF ρ = 0.41, Total VM ρ = 0.61, Awake VM ρ = 0.69), Aldolase A (UniProt: P04075) (LVEF ρ = 0.41, Arm QMT ρ = 0.49, Total QMT ρ = 0.50), Elafin (UniProt: P19957) (LVEF ρ = −0.37, Arm QMT ρ = −0.61, Leg QMT ρ = −0.52, Total QMT ρ = −0.58, Total VM ρ = −0.67, Awake VM ρ = −0.77), glial cell-line derived neurotrophic factor family receptor alpha-1 (UniProt: P56159) (LVEF ρ = 0.34, Arm QMT ρ = 0.54, Total QMT ρ = 0.53), and Troponin I–fast skeletal muscle (UniProt: P48788) (LVEF ρ = 0.34, Arm QMT ρ = 0.53, Total QMT ρ = 0.50). ALT was ubiquitously expressed. The remaining proteins had minimal or no expression in the heart, with predominant expression in other tissues such as the liver, skin, salivary glands, brain, and esophagus.
Linear regression analysis
The 10 proteins with the strongest correlation to LVEF all demonstrated continued correlation after correcting for covariates of interest (Supplemental Table 3). Similarly, the majority of the proteins that correlated with total QMT also retained significance after correction for covariates (Supplemental Table 4).
Discussion
Our study is the first of which we are aware to employ a nontargeted, large-scale proteomics-based strategy—using the SomaScan platform—to identify serum biomarkers correlated with comprehensive cardiac phenotyping in patients with DMD. Several studies have investigated potential biomarkers for DMD using targeted approaches or evaluating SomaScan in cohorts without comprehensive cardiovascular phenotyping. This approach offers novel insights for early detection and therapeutic targeting. The identified serum biomarkers could serve as screening tools to identify DMD patients at higher risk for cardiomyopathy, thereby reducing reliance on costly and less accessible imaging modalities such as cardiac magnetic resonance imaging. Additionally, these biomarkers could be incorporated into longitudinal monitoring strategies to track disease progression and therapeutic response over time.
Prior work underscores the potential of large-scale proteomics in DMD. Hathout et al. performed one of the earliest comprehensive serum proteomics investigations in DMD, identifying proteins related to muscle degeneration, inflammation, and fibrosis, and thereby demonstrating the utility of nontargeted screening for biomarker discovery. 24 Anderson et al. employed a proteomics approach to explore eight proteins that were previously implicated in cardiac and skeletomuscular disease, identifying ST2 as a potential indicator of DMD-associated cardiomyopathy, which was also identified in this study as significantly associated with LVEF (ρ = −0.34, q = 0.037). 8 Building on these findings, our study systematically analyzes serum biomarkers that correlate with both cardiac and skeletal indices in DMD.
We identified several candidate serum biomarkers that significantly correlated with disease indices. Notably, while some proteins were uniquely associated with either skeletal or cardiac measures, 10 proteins overlapped between the two, suggesting distinct yet interconnected pathways in DMD progression. These findings underscore the complexity of dystrophin deficiency and highlight the promise of nontargeted proteomics in uncovering clinically relevant biomarkers for improved risk stratification and targeted therapies. However, it is important to consider that some proteins may reflect a cellular leak phenomenon due to ongoing cellular damage from the underlying disease. For instance, Aldolase A and ALT—both abundantly expressed in heart and skeletal muscle cells—may “leak” into the plasma as cell death increases, a phenomenon previously documented in DMD. While these proteins may be less useful as novel biomarkers for assessing disease severity, the fact that we detected elevation in these biomarkers further supports our nontargeted analysis.
Among the biomarkers significantly correlated with cardiac disease, several—such as Dickkopf-related protein 3, 25 metalloproteinase inhibitor 1, 26 glutathione S-transferase P, 27 and interleukin-13 receptor subunit alpha-1 28 —have been previously associated with heart failure. Piek et al. showed Dickkopf-related protein 3 plasma concentrations were higher in heart failure patients in comparison with age- and sex-matched controls without heart failure. 25 Tseng et al. found that metalloproteinase inhibitor 1 was associated with reverse remodeling in LVEF in subjects with decompensated heart failure with reduced ejection fraction. 26 Andrukhova et al. found that glutathione S-transferase P is strongly associated with heart failure and could serve as a sensitive and specific marker to predict the ventricular function in heart failure patients. 27 Finally, Amit et al. found interleukin-13 receptor subunit alpha-1 to be significantly downregulated in the hearts of patients with heart failure. Given these established associations and their correlation with cardiac indices in our DMD cohort, these proteins represent promising candidates for further investigation as biomarkers for cardiac disease in DMD. Among the biomarkers significantly correlated with skeletal muscle disease, repulsive guidance molecule A (RGMA) has been identified by other large scale serum proteomics to be associated with performance decline and clinical milestones in DMD. This finding further corroborates our study and supports RGMA's potential relevance as a biomarker of disease progression. 29 In the same study, Ikelaar N. A. et al. identified histone-lysine N-methyltransferase (EHMT2) to be a top protein candidate for predication of musculoskeletal clinical milestone. While EHMT2 did not meet significance threshold for our musculoskeletal clinical indices, it correlated significantly with both LVEF and LGE clinical indices. This further adds to EHMT2 candidacy as a potential biomarker for DMD disease progression. 29
While many of the pathways identified in our analysis have already been implicated in the progression of DMD cardiomyopathy—specifically calcium dysregulation, fibrosis, and inflammation—we found a significant number of proteins associated with lipid regulation/metabolism. These pathways have been reported in adult cardiomyopathy research but have not been implicated in DMD cardiomyopathy. 30 Interestingly, recently work evaluating whole genome sequencing has also uncovered lipid metabolism polymorphisms as important in the progression of DMD cardiomyopathy. 31 While exploratory, this work provides a potential roadmap to aid in understanding DMD cardiomyopathy progression and implicates novel pathways that could be leveraged for future therapeutics.
In our cohort, the proteins identified did not consistently correlate across LVEF, LGE, and ECC. Additionally, no significant associations were observed with FWHM. We suspect that this relates to the inherent variability in FWHM measures, in contrast to the more reproducible assessment of presence or absence of LGE.
Our study does have several limitations. First, we focused solely on serum ligand levels without assessing receptor expression, which can significantly influence biological outcomes. Moreover, protein expression at the tissue level may vary, yet our study did not include tissue samples—potentially omitting crucial contextual information. We performed an exploratory analysis with correction for covariates of interest. While most proteins retained their significant correlations, this analysis is limited by the smaller sample size. Future studies should investigate the effect of covariates of interest, particularly cardiac medications and corticosteroids, on biomarker expressions in larger cohorts. It is worthy of note that all our patients were on therapies that are consistent with the current guidelines. Finally, although our patient cohort was small, it did encompass a broad range of functional abilities and ages, providing valuable insights despite the limited sample size. Future studies incorporating receptor analyses, tissue-level investigations, and larger cohorts will be essential for validating and extending our findings.
In conclusion, our nontargeted proteomics study leveraging SomaScan technology identified serum biomarkers that correlate with both skeletal and cardiac disease progression in DMD. Building on prior large-scale investigations, we discovered candidate proteins—some uniquely associated with skeletal or cardiac indices and others overlapping—that underscore the complexity of dystrophin deficiency. Our findings offer promising leads for future studies aimed at enhancing risk stratification and guiding targeted therapies in DMD.
Supplemental Material
sj-xltx-1-jnd-10.1177_22143602261438533 - Supplemental material for Identification of novel protein biomarkers correlating with both cardiac and skeletal muscle indices in duchenne muscular dystrophy
Supplemental material, sj-xltx-1-jnd-10.1177_22143602261438533 for Identification of novel protein biomarkers correlating with both cardiac and skeletal muscle indices in duchenne muscular dystrophy by Mark Naguib, Katheryn E Gambetta, Jaclyn Tamaroff, William B Burnette, Rachel Harris, Meng Xu, Christopher Slaughter, Larry Markham, Christopher Spurney, Jonathan H Soslow and in Journal of Neuromuscular Diseases
Supplemental Material
sj-docx-2-jnd-10.1177_22143602261438533 - Supplemental material for Identification of novel protein biomarkers correlating with both cardiac and skeletal muscle indices in duchenne muscular dystrophy
Supplemental material, sj-docx-2-jnd-10.1177_22143602261438533 for Identification of novel protein biomarkers correlating with both cardiac and skeletal muscle indices in duchenne muscular dystrophy by Mark Naguib, Katheryn E Gambetta, Jaclyn Tamaroff, William B Burnette, Rachel Harris, Meng Xu, Christopher Slaughter, Larry Markham, Christopher Spurney, Jonathan H Soslow and in Journal of Neuromuscular Diseases
Footnotes
Acknowledgments
The authors thank the patients for their participation in the study. We also thank the multidisciplinary staff at the Duchenne Muscular Dystrophy Clinic at Monroe Carell Children's Hospital for their support and assistance with acquiring the plasma samples.
Ethical consideration and consent to participate
This study was approved by the Ethics Committee of Vanderbilt University. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Author contributions
Mark Naguib: concept design, figure design, drafting initial manuscript; Katheryn E Gambetta: manuscript editing; Jaclyn Tamaroff: manuscript editing; W Bryan Burnette: manuscript editing; Rachel Harris: manuscript editing; Meng Xu: statistical analysis and manuscript editing; Christopher Slaughter: statistical analysis and manuscript editing; Larry Markham: funding, manuscript editing, supervision; Christopher Spurney: manuscript editing, supervision; Jonathan H Soslow: concept design, funding, supervision, drafting initial manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fighting Duchenne Foundation and the Fight DMD/Jonah & Emory Discovery Grant (J. Soslow); the Food and Drug Administration Orphan Products Grant R01FD006649 (J. Soslow); the National Center for Research Resources, Grant UL1 RR024975-01; and is now at the National Center for Advancing Translational Sciences, Grant 2 UL1 TR000445-06 (G. Bernard); and by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number K23HL123938 (J. Soslow), R56HL141248 (J. Soslow), and R01HL167969 (J. Soslow, L. Markham, K. Hor).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: W Bryan Burnette: Received research funding and reimbursement for participation in an advisory board from Sarepta Therapeutics. Jonathan H Soslow: Boerhinger Ingelheim (consultant), Capricor (consultant), Dyne (consultant), Immunoforge (consultant), NS Pharma (consultant), Sardocor (DSMB), Sarepta (Consultant), Wave (Consultant). All the other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data to support the findings of this study are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.