
Abstract
Adult SMA REACH is a
Introduction
Spinal Muscular Atrophy (SMA) is a rare neuromuscular disease that causes progressive weakness in the limbs and trunk and atrophy of the muscles. The hallmark of the disease is the degeneration of anterior horn cells in the spinal cord, giving rise to the characteristic muscle atrophy of varying degrees. 1 The most common form of SMA which accounts for over 95% of cases is the autosomal recessive form that results from a homozygous deletion in the survival of motor neuron 1 (SMN1) gene – also known as 5q SMA. This form of SMA is one of the most common genetic causes of childhood mortality, however the phenotype of the disease is largely variable and is classified into five main types (type 0 to 4) based on age of onset and achieved motor milestones. 2 An almost identical copy of the SMN1 gene, SMN2 also contributes to the phenotypic classification, with the clinical severity inversely correlating with the SMN2 gene copy number. 3
Although a monogenetic disease, SMA is generally perceived as a complex disease due to the highly variable phenotypic spectrum and multiple system involvement and as such it requires a multidisciplinary care approach to be successfully managed. In addition to neuromuscular specialists, patients require a combination of respiratory, nutritional, and orthopaedic care alongside mental health support to aid in the decline of psychosocial wellbeing that is sometimes experienced by adults contemplating the progression of their disease. 4 As new treatment options become available, the size of the adult SMA population will continuously grow, therefore establishing a standardised and structured approach to the management of adults is essential. 5
In recent years, the treatment landscape in the SMA setting has rapidly evolved with 3 disease modifying therapies (DMT's) now available. 2 Onasemnogene abeparvovec (Zolgensma) is the first and only approved gene therapy in SMA but is not available for older children or adults. 6 In 2019, The National Institute for Health and Care Excellence (NICE) communicated the conditional approval of Nusinersen followed by the conditional approval of Risdiplam in 2022 under a Managed Access Agreement (MAA) in England, Wales and Northern Ireland.7,8 The commencement of an MAA allows for time limited access to new therapies that have shown promise but lack sufficient evidence to be made routinely available on the NHS whilst further evidence is compiled. 9 The label also included treatment for adult patients however consensus on the management of SMA, particularly the development of standards of care (SoC), has focused primarily on the paediatric population with evidence suggesting a lack of co-ordination in the provision of such care in adults.10–13 In light of the rapidly developing therapy landscape, it was evident that there was an urgent need to establish stronger clinical networks and real-world data (RWD) collection to monitor and gain a better understanding of the impact of novel treatments on the natural history of the disease, particularly in the adult population where expectations of treatments were largely unknown due to lack of available data.14,15
Adult SMA REACH is a
The aim of this paper is to describe the operational complexity and key considerations involved in establishing a RWD collection study and clinical network in the UK; detailed baseline data of the study population will be described in a separate paper.
Methods
Pre-existing initiatives
Prior to the set-up of Adult SMA REACH, there was no formal clinical network in the UK for adult patients living with SMA. However, a paediatric network and data collection study was established by Professor Muntoni known as SMA REACH UK which led to improved knowledge of SMA in the real-world setting.16–23 Adult SMA REACH works collaboratively with SMA REACH UK and allows for transition from the paediatric to adult database, ensuring continuity in the collection and analysis of their data between paediatric and adult services.
Adult SMA REACH also works collaboratively with the UK SMA Patient Registry to ensure the patient voice compliments the clinical data collected. The UK SMA Patient Registry was established in 2008 and collects patient reported data from individuals living with SMA in the UK & Ireland using the TREAT-NMD SMA Core dataset (https://www.sma-registry.org.uk/).24,25 Registration is patient initiated via an online portal and in April 2022, the collection of patient reported outcome measures (PROMs) was introduced in the registry to supplement clinical and genetic data held therein. This initiative and the close collaboration between Adult SMA REACH and the Patient Registry allowed the inclusion of PROMs in the MAA for both Nusinersen and Risdiplam.
Aims of the data collection study
Develop a standardised data set for the UK adult SMA population in close collaboration with paediatric SMA REACH UK to capture natural history data and the impact of new therapies and interventions.
Implement a data collection research study across the Adult SMA REACH network's sites to collect data leading to a better understanding of the natural history of adult SMA and evolving phenotypes.
Data collection study: Study design and set up
We conduct a multi-centre observational longitudinal RWD collection study for adult patients (≥ 16 years) with genetically confirmed 5q SMA. Adult SMA REACH is coordinated by the John Walton Muscular Dystrophy Centre within Newcastle University but is Sponsored by The Newcastle Upon Tyne Hospitals Foundation Trust following the UK Policy Framework for Health and Social Care Research. 26 The project has received approval from the North East - York Research Ethics Committee and the Health Research Authority (HRA). Adult SMA REACH follows the International Conference on Harmonisation Good Clinical Practice (ICH GCP) guidelines which is the international standard for the conduct of research involving human participants. 27 All NHS Trust across the UK that provided a neuromuscular specialist service and were delivering either Nusinersen or Risdiplam were selected for participation in the study.
Governance structure
Adult SMA REACH has a steering committee (SC) composed of site representatives including representation from the multidisciplinary team, representatives from paediatric SMA REACH and patient representatives; industry representatives are not permitted. The purpose of the SC is to:
Advise on strategic direction, opportunities, and priorities for the registry. Provide input and guidance if requested on publications, posters, presentations, or other materials. Review all data requests to Adult SMA REACH, requesting further information or providing approval where appropriate (and if in-line with the interests of Adult SMA REACH). Promote Adult SMA REACH where applicable.
The SC meets every 6 months and ad hoc for data requests or similar. In order to access anonymised data, individuals must submit a data request form that outlines the purpose of the request including specific data points to be obtained, how the data will be used and a basic statistical analysis plan. Data requests must receive votes by two thirds of SC members in order for the request to be processed. Out of the SC votes received, two thirds must be in favour for the data request to be approved. A fee for industry enquiries is applied to ensure sustainability of the data.
The governance policies include a data request process approved by the steering committee and a publication policy approved by all members of the network. The full data access policy and Standard Operating Procedure (SOP) can be found in the Supplementary Materials.
The Adult SMA REACH project receives financial support from Biogen and Roche. In accordance with the funding agreements, these companies have no involvement in the governance or scientific direction of the project and do not have access rights to the data.
Education, training and networking
As part of the network and data collection study activities, Adult SMA REACH provides comprehensive training on data collection that covers the entire data cycle, from data generation in clinics to data entry in the database. The team also offers face-to-face (F2F) and remote training sessions on the motor outcome measures required for data collection. These sessions are available to both new and existing evaluators, including those from newly activated sites or newly appointed staff. All F2F training sessions are CPD-accredited. In addition, regular reliability calls are held to assess and improve inter- and intra-rater reliability among physiotherapists across the network. Allied Healthcare Professional (AHP) networking days are jointly organised with the paediatric SMA REACH UK team to provide interactive and informative sessions for participating evaluators. The main objectives of these training activities are to ensure standardisation of data collection and to identify and address challenges in the assessment of SMA patients.
Annual networking meetings are also held to update the project and representatives from the participating sites, SMA REACH UK (paediatric), patient advocacy groups, regulators and industry are invited to attend. Due to Covid-19 restrictions, these meetings have been held remotely however the first kick off meeting was held pre-pandemic in 2020 and thereafter the first F2F meeting was held in November 2023. To raise awareness, increase engagement and improve the sustainability of the project, the project team have presented a number of posters at a range of both national and international conferences.
Data collection and IT platform
Adult SMA REACH collects data using an online database called NND (National Neuromuscular Database) developed by CERTUS technology which is accessible through an NHS environment. In recent months, work has been undertaken to develop a new database built within Newcastle University by the Research Software Engineering team. The new platform is hosted via Microsoft Azure and Adult SMA REACH data is stored securely in the UK by cloud services provided by Azure. Access to the database is via a secure portal, is password protected and is limited to restricted users participating in the project who have been granted access by the central coordination team. The new platform is planned for launch imminently.
Both the CERTUS database and new platform developed by Newcastle University comply with ISO 27001 Information Security Management System (ISMS) and the UK Data Protection Act 2018 governing the rights and duties of companies to safeguard personal data. 28
The dataset has been agreed by the network and is aligned with the international consensus for SMA registries (TREAT-NMD, iSMAC) and includes the mandatory items for both MAAs. The dataset comprises data collected during routine clinical visits from demographic data, treatment data to outcome measures. The full list of data items is detailed in the Supplementary Materials. The visit schedule is every 6 months for treated patients and annually for non-treated patients. Continuous data collection for patients who have transitioned from childhood to adulthood is facilitated with an automatic linkage of the Adult SMA REACH database and SMA REACH UK database. When patients move from the paediatric SMA REACH UK study to the Adult SMA REACH study, a new consent is obtained prior to transition on the database and before any adult clinical data are entered.
Data quality is ensured by the continuous and systematic monitoring of data. Data management techniques include the creation of a data model for the dataset structure and an in-house software developed to automate the identification of quality issues such as missing values, plausibility and inconsistencies in data. Data query reports are generated with the assistance of the in-house software and are sent quarterly to the participating sites.
The overall infrastructure of Adult SMA REACH, including the flow of data from participating adult neuromuscular centres into the data collection study and how key related initiatives such as SMA REACH UK and the UK SMA Patient Registry interact with Adult SMA REACH is illustrated in Figure 1.
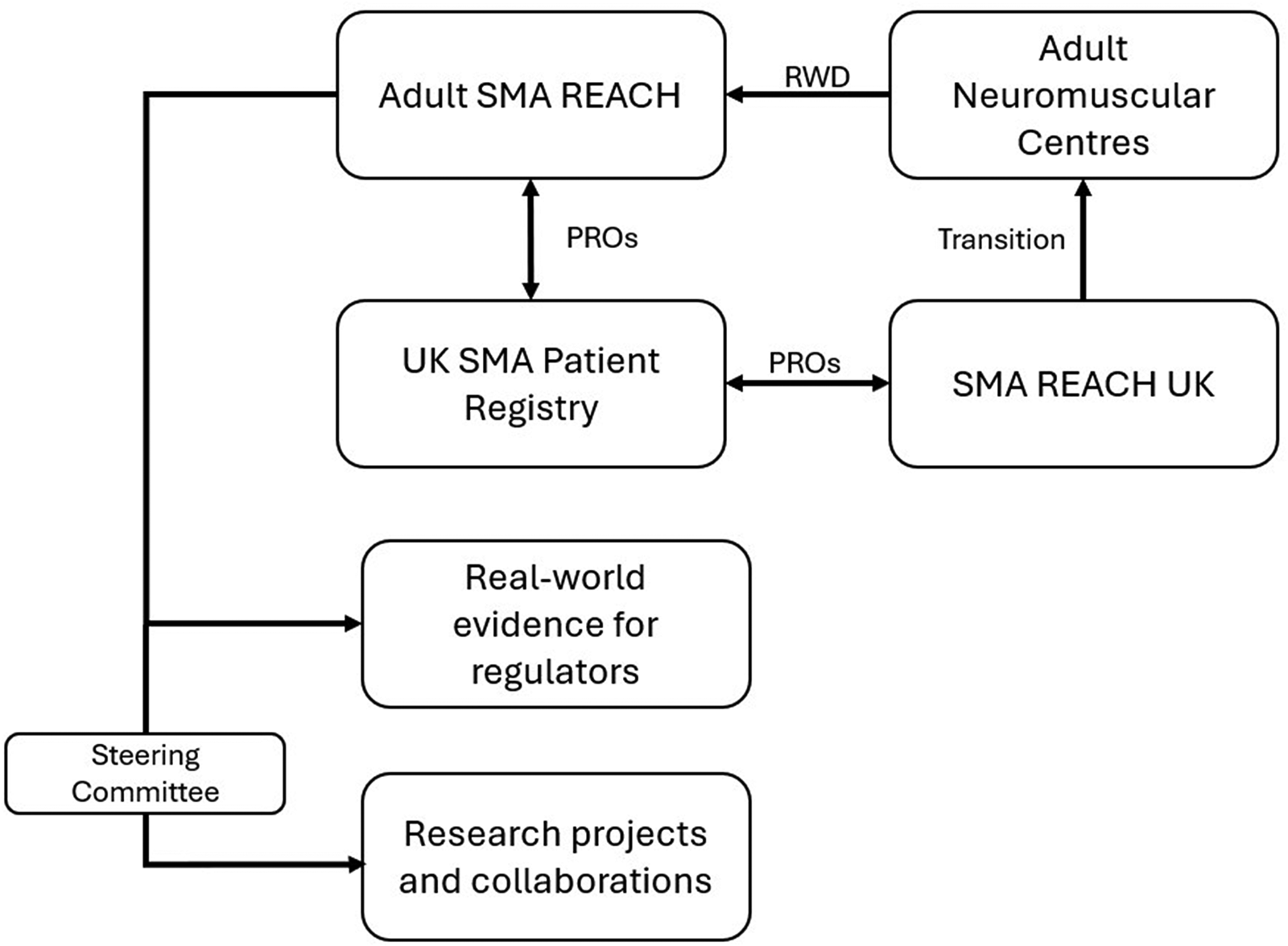
High-level structure of the Adult SMA REACH project showing the flow of data.
Monitoring visits
In order to ensure that the project is conducted in line with ICH GCP guidelines and that data collected is accurate and high quality, a combination of remote and onsite monitoring has been carried out. The data monitoring plan specifies an annual monitoring schedule focused on remote oversight. Nonetheless, under a risk-based framework, onsite monitoring may be initiated on an ad hoc basis when deemed necessary. The process of preparing the final data cuts under the MAA's prompted the initiation of onsite monitoring. During onsite monitoring visits, tailored training was provided to address findings identified through remote monitoring. Following onsite monitoring visits, reports were provided to study teams with a summary of findings and a structured action plan of how to address these in both the short and long term. Visits were conducted following a standardised framework and findings were categorised as minor, moderate or critical.
Managed access agreement requirements
Adult SMA REACH was chosen by NICE and pharmaceutical companies as the tool to collect RWD that can support the approval of Nusinersen and Risdiplam through the MAA. The participation in the MAA for Nusinersen and Risdiplam required the identification of baseline and follow-up visits following specific definitions in each MAA in spite of it being a RWD collection study. Only data from patients that met the MAA baseline definitions, that is a visit which could be identified as a baseline visit (- 6 + 3 months from date of first dose of Nusinersen, -/+ 6 months from date of first dose of Risdiplam), and data from the follow-up visits (6 monthly) could be included in the analysis. Some data items and the visit schedules were also mandated by the MAA. Both MAAs also included a Statistical Analysis Plan (SAP) developed by the individual pharmaceutical companies that when possible were aligned, although some aspects did differ.
The period of data collection for Nusinersen started once the MAA was approved in July 2019 which was prior to the set-up of the project, therefore sites were encouraged to collect SMA SoC data in the clinical records.10,11 However, Risdiplam data collection started in January 2022, and sites started collecting the data using the paper study forms until the database was launched in October 2022.
Data has been reported to NICE throughout the data collection period and has included updates on the progression of data collection and entry in addition to the quality of collected data.
Results
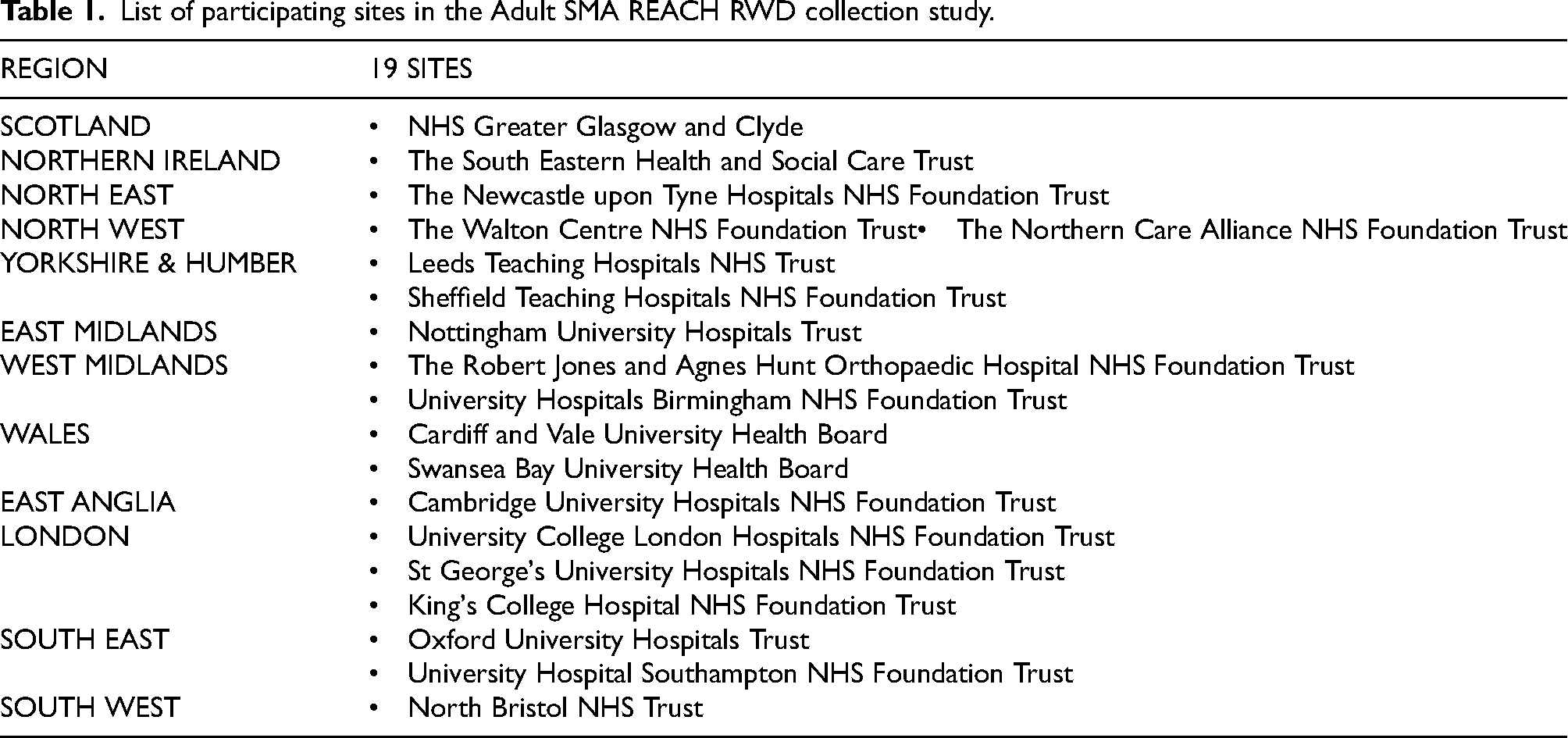
Currently there are 19 sites participating, 15 from England, 2 from Wales, 1 from Scotland and 1 from Northern Ireland. In July 2022 the first centre was activated, and the rest of the centres were activated in cascade, the last one in November 2025. Table 1 below represents the current sites participating in the project, the regional distribution of patients is shown in Tables 2 and 3. It is important to note that the site in Northern Ireland was activated after the data cut for this manuscript; consequently, no data from patients enrolled at this site are presented here.
List of participating sites in the Adult SMA REACH RWD collection study.
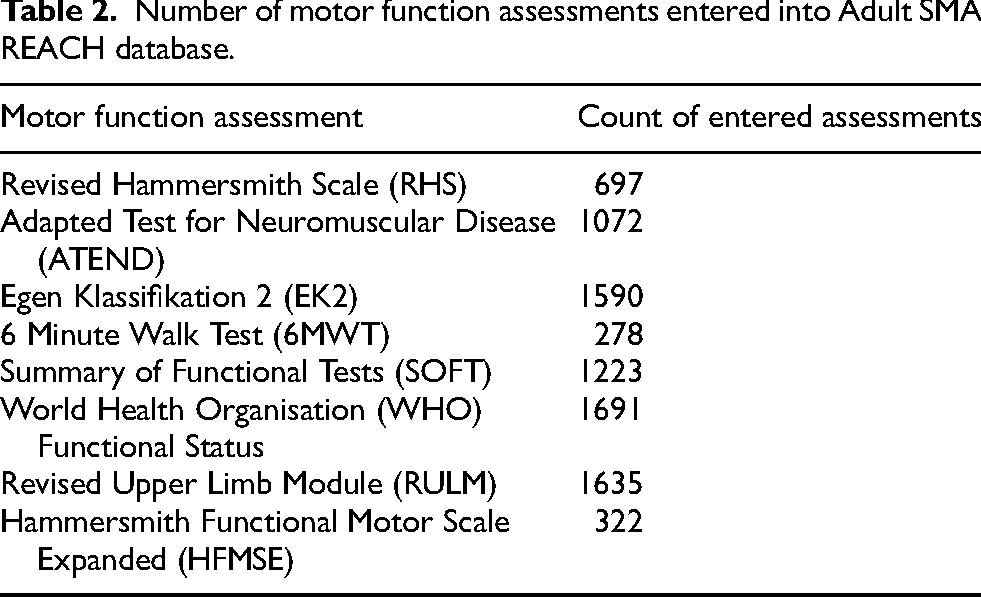
Number of motor function assessments entered into Adult SMA REACH database.
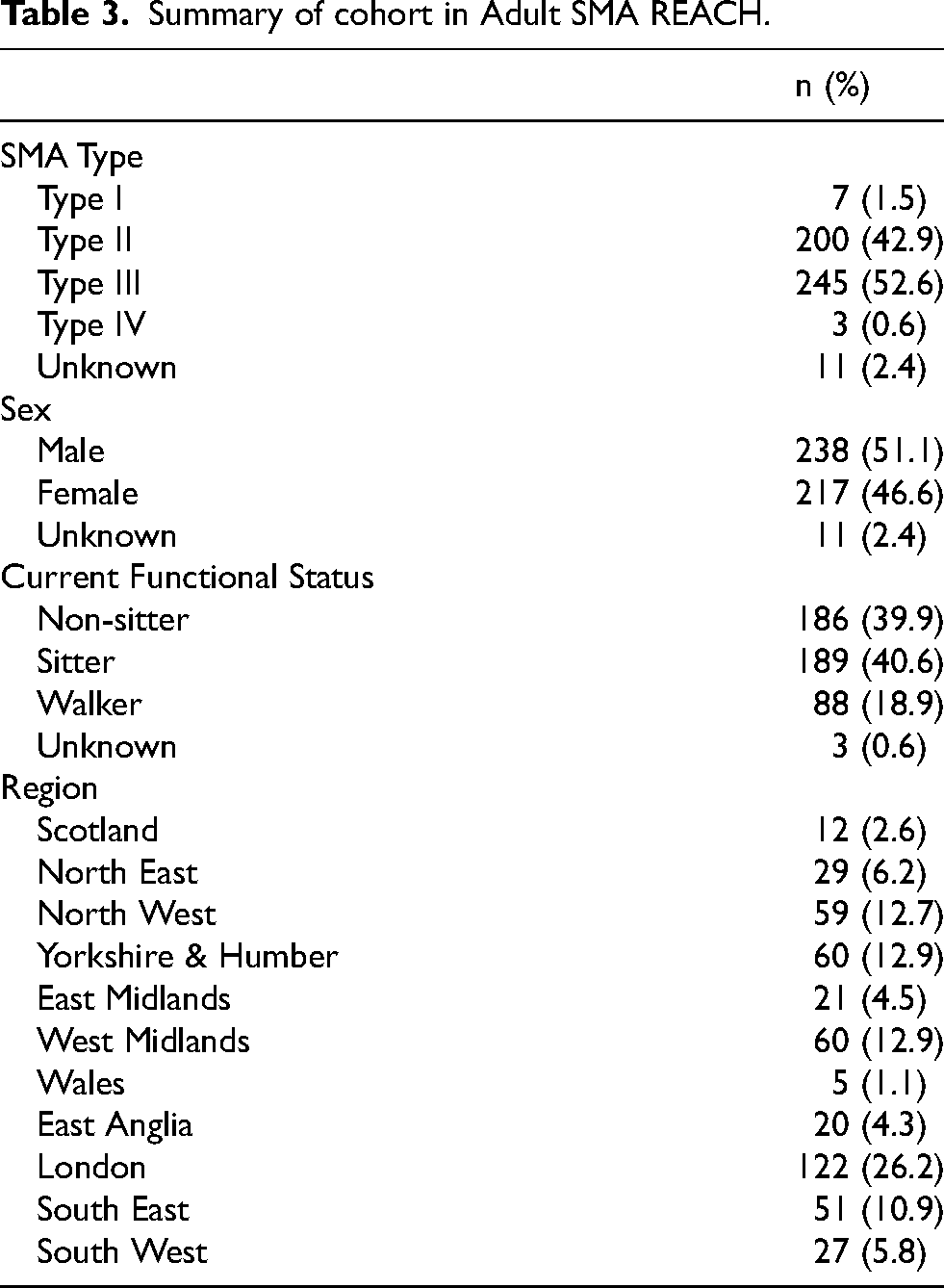
Summary of cohort in Adult SMA REACH.
The network is comprised of a range of different health care professionals such as neurologists, physiotherapists, nurses and care advisors in addition to diverse research teams involving data managers, clinical trial coordinators, project managers and admin support staff. Patient organisations, industry and regulators also form part of the network and are actively involved in supporting its key aims.
As of 01/04/2025 the database contains data from 466 patients and 2255 visits, with more than 8000 motor function assessments (see table 2). The population is comprised of mostly SMA Type 2 and SMA Type 3 patients with an almost equal split of males and females (see table 3). A total of 98 patients have transitioned from the paediatric SMA REACH UK database to the Adult SMA REACH database; of these, 88 have at least one recorded visit in an adult clinic.
Figure 2 shows the rate of patient recruitment from the launch of the database, with a period of initial rapid growth in patient numbers followed by a plateau. The number of patient visits entered has continued to steadily grow over the duration of the study.
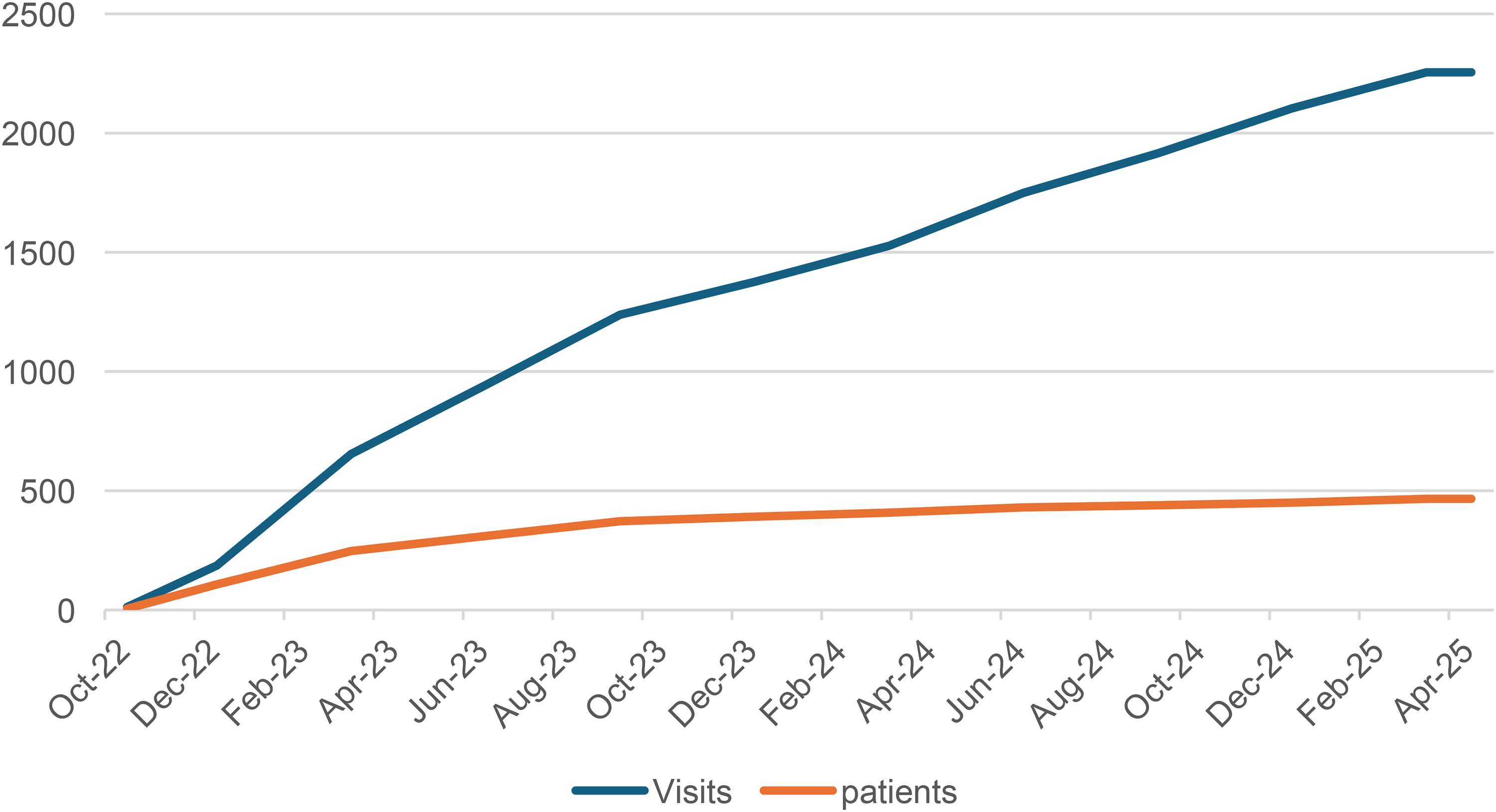
Adult SMA REACH recruitment history and visit entry progression from time of database launch in October 2022 until most recent data cut in April 2025.
For the purposes of MAA, the final data cut for Nusinersen and Risdiplam was scheduled for June and August 2023 and the final report was delivered in November and December 2023 respectively. From 104 patients, 94 were included in the Nusinersen analysis, after applying the Nusinersen MAA criteria. For the Risdiplam analysis, data was obtained from 223 patients and 176 were included after applying the Risdiplam MAA criteria. Results from both analyses are confidential until final resolution. The completeness of different data items across the longitudinal timepoints imposed by the MAA are displayed in Table 4.
Longitudinal data completeness.
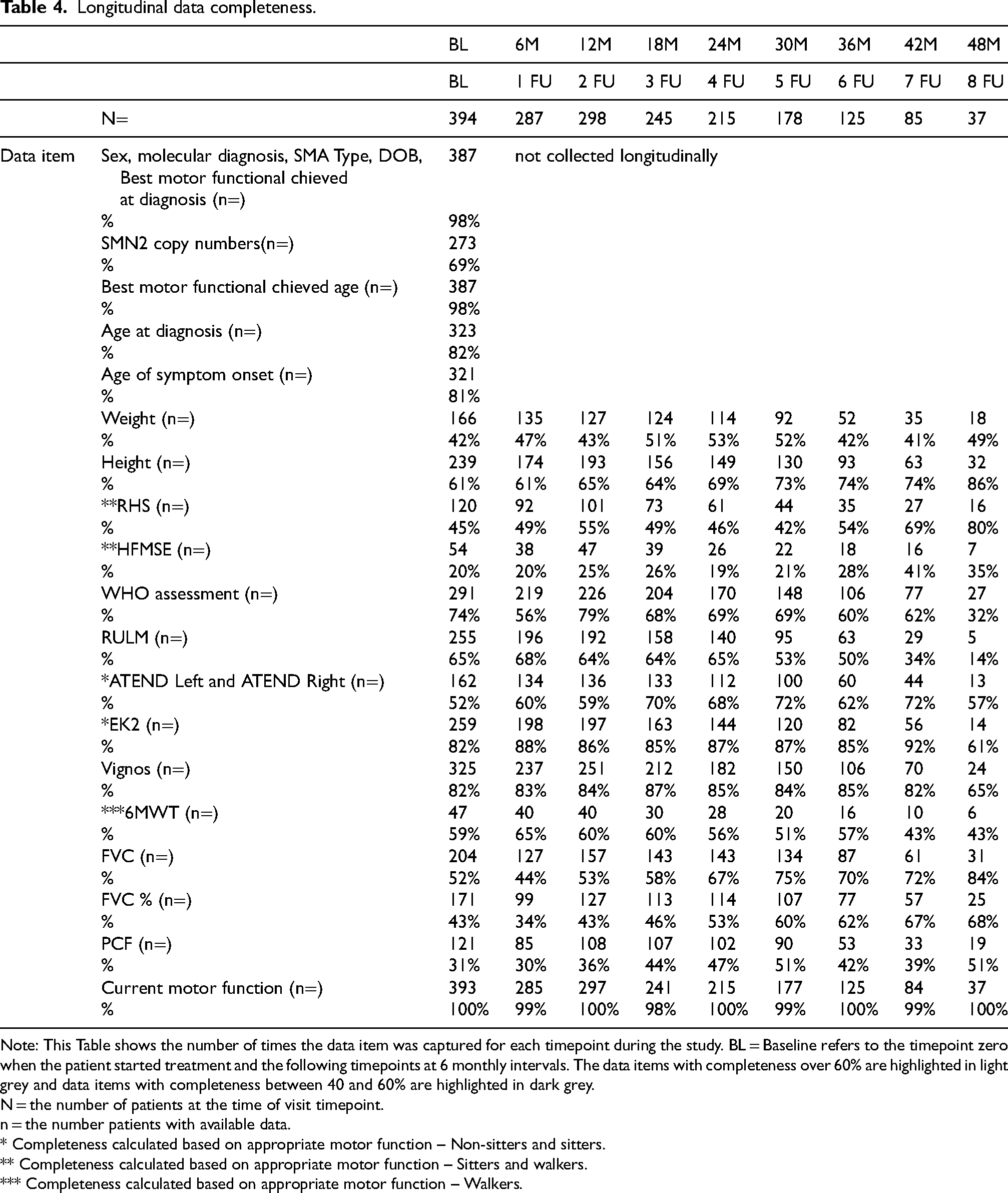
Note: This Table shows the number of times the data item was captured for each timepoint during the study. BL = Baseline refers to the timepoint zero when the patient started treatment and the following timepoints at 6 monthly intervals. The data items with completeness over 60% are highlighted in light grey and data items with completeness between 40 and 60% are highlighted in dark grey.
N = the number of patients at the time of visit timepoint.
n = the number patients with available data.
* Completeness calculated based on appropriate motor function – Non-sitters and sitters.
** Completeness calculated based on appropriate motor function – Sitters and walkers.
*** Completeness calculated based on appropriate motor function – Walkers.
On-site monitoring visits have been performed for 13 sites at present. The main objective of these visits was to check site compliance with ICH GCP, to address repetitive data quality issues and perform source data verification (SDV) to assess the credibility of data. The visits also provided an opportunity for each site to discuss any barriers or issues impacting study delivery such as lack of staffing/capacity at site, lack of understanding of research processes and lack of infrastructure/clinic space to be able to carry out required assessments. The most frequent issue identified was lack of capacity and staffing required to deliver the study, both in regard to the collection of required data in clinic and the ability to enter collected data to the database. 9/13 sites reported lack of staffing as one of the leading issues impacting study delivery and performance with the largest participating site having a patient to staff ratio greater than 26:1. The study was delivered with direct support from dedicated research teams at only 6/13 sites. At the remaining sites, the study was delivered directly via clinical staff without research experience, resulting in gaps in knowledge around governance processes and study documentation that should be filed at site. The Investigator Site File domain of the monitoring visit which assessed the relevant study related documentation filed at site including GCP certifications for staff was rated critical or moderate at 5/13 sites.
Formal feedback was obtained following both the physiotherapy specific network day and the annual networking meeting held F2F for the first time in 2023. The events were well attended with 47 participants from both the adult and paediatric network attending the physiotherapy network day and 60 participants attending the annual networking meeting. Feedback and comments received were very positive with the majority of attendees reporting that the content delivered was extremely useful. Outputs from the physiotherapy network day included identifying the need for a respiratory sub-group within the SMA REACH network, including the need to establish guidelines for respiratory testing across the sites. In addition to this, it was highlighted that a workshop on temporomandibular joint dysfunction (TMJ) and contracture management in SMA patients would be beneficial. It is evident that these events provide an invaluable opportunity to raise challenges faced amongst the network in the assessment and management of SMA patients and to then create a plan to address these gaps in knowledge to further standardise care provision across the UK.
Discussion
The Adult SMA REACH database is currently the only of its kind in the UK. It is the largest clinician reported SMA specific repository and is able to support researchers and academics with their work. There is no clear age-stratified prevalence data for the UK SMA population; however, it is estimated that SMA affects approximately 1 in 11,000 live births, with up to an estimated 1600 children and adults currently living with SMA across the UK. Between January 1, 2019, and November 1, 2024, a total of 507 patients with SMA (213 [42%] with SMA type 1, 188 [37%] with SMA type 2, and 106 [21%] with SMA type 3) were registered in the SMA REACH UK database.13,29 This figure, combined with registrations in Adult SMA REACH (466 patients), represents a substantial proportion of the estimated national SMA cohort. It should be noted that 98 patients have transitioned from the paediatric to the adult registry, so there is potential overlap between these figures.
The Adult SMA REACH structure reflects a possible model that can be adopted to inform on the impact of new therapies in a relatively short time frame through the establishment and utilisation of a national network in collaboration with the SMA REACH UK team. Particularly in the rare disease sector with geographically dispersed patient populations, initiatives such as Adult SMA REACH are vital for the avoidance of data silos which fragment and undermine research efforts. 30 The success of such a project relies on the multidisciplinary expertise across the network and a dedicated project team within the coordinating site to provide direction, raise awareness of the initiative and disseminate outputs to support its sustainability.
The collaborative aspect of this project is fundamental in building such networks; it has allowed for both the identification of barriers to standardised care provision and the sharing of best practise amongst the network of how best to support adult SMA patients, particularly through the transition phase where it is documented that patients with chronic illness or disability can be lost to follow up during poorly managed transitions.31,32 Historically, many SMA patients have disengaged from services upon reaching adulthood due to fragmented care pathways through the transition period, as the application of therapies and evolution of disease management consensus has primarily focused on paediatric populations. Among the positive outcomes, Adult SMA REACH has helped to improve engagement from adults who before now have felt relatively neglected according to reports in the literature about adult SMA patients’ perception of healthcare.32,33 The close collaboration between Adult SMA REACH and SMA REACH UK has further improved the overall transition process for SMA patients in the UK. The linkage between both databases and initiatives has not only facilitated the continuity in data collection from paediatric to adult services, but it has also provided an interface for paediatric and adult clinical teams to collaborate, create harmonised care pathways and discuss how best to support patients through the period of transition.
Additionally, the project also delivered the final reports for the MAAs for both Nusinersen and Risdiplam in line with the imposed timelines ultimately illustrating how RWD can be leveraged to accelerate therapy approvals and support regulatory decision making. Regulatory guidance and opinion on the use of RWD for this purpose has evolved in recent years with advent of several regulator supported initiatives including a RWE programme and framework published by the FDA and the IMI GetReal initiative endorsed by the EMA. 34 Concerns around the use of RWD for regulatory decision making are usually centred around selection bias, unrecognised baseline differences and low-quality data.35,36 The use of multivariate regression models in the analysis of RWD offers a partial solution to address the challenges of confounders in RWE. 37 The nature of RWD means that data quality will always be a limiting factor when directly comparing to data collected in clinical trials, however there are approaches which can help to mitigate this.34,36 The Adult SMA REACH project introduced a standardised dataset that aligned with the international consensus for SMA registries (TREAT-NMD, iSMAC) alongside standardised functional outcome measures. This not only improved its interoperability but also the ease at which the data could be monitored and cleaned utilising data modelling techniques. The establishment of a national clinical network including investment into comprehensive training for SMA assessors and networking opportunities to share best practice was a key driver in ensuring the RWD collection study was able to fulfil its purpose and provide dependable RWE to support the approvals of Nusinersen and Risdiplam in the UK.
The most significant challenge the project faced which had a marked impact on data collection activities was the establishment and delivery of a research project within a clinical setting during a pandemic. Typically, research projects are delivered by dedicated research staff within NHS Trust's, and academics who have good working knowledge of GCP and requirements to execute research projects. As data collection for the purpose of both MAA's was incorporated into the data collection study, the project was delivered through the clinical teams, of which many had never undertaken any research and were unfamiliar with the research obligations and approval processes involved. 38 In addition to this, the pressure on the NHS has grown significantly in recent years, especially following the pandemic, therefore clinical capacity to manage usual day to day duties in addition to research was limited. 39 The effect of this was considerable delays in the activation of sites and large backlogs of data which had to be entered retrospectively to the Adult SMA REACH database to comply with the MAA aspect of the data collection study.
During the onsite monitoring visits, it was reported that the most common barrier affecting study performance was lack of capacity at sites both in regard to the collection of data and entry of data. The Adult SMA REACH study was registered on the NIHR Clinical Research Network (CRN) Portfolio to be eligible for support from the study support service which is a standard national framework of support to help plan, place and perform high quality research. 40 However, this support was not utilised fully, likely due to lack of knowledge from the participating sites on how to access this support and also due to local processes for how this support is distributed amongst studies in each Trust. Improved and more frequent communication at an early stage of the project with participating clinical teams to reiterate this support would have been beneficial. Other rare disease initiatives in the UK which aim to do this are the DMD and BMD Hubs, which both prepare and upskill clinical sites for research and trial delivery.41,42
The MAA data that was collected through Adult SMA REACH imposed cumbersome and lengthy assessments not only for clinicians but patients too. A feedback survey on stakeholder experience of the MAA's revealed that patients reported high levels of anxiety and a feeling of a need to ‘perform’ in their appointments as to not reach stopping criteria and jeopardise their access to treatment. 38 Whilst MAA's provide opportunity for patients to access treatments early on, the effect on their mental health, particularly for patients who feel they experience a benefit but show no measured improvement in their assessments, is a point to consider.
The impact of the Adult SMA REACH project on care provision for adults in the UK, and its ability to generate real-world evidence (RWE) to support regulatory decision-making within only five years, highlights the relevance and potential of disease-specific registries in the rare-disease setting. A similar initiative, SMArtCARE in Germany, Austria and Switzerland, demonstrates how this model can be applied internationally and further reinforces the value of structured clinical networks in producing high-quality RWE that can be integrated into regulatory frameworks for therapy approvals. Although the two initiatives share common goals, they differ slightly in scope and population focus. SMArtCARE encompasses all ages with 5q-SMA and operates as a multi-national academic registry, whereas Adult SMA REACH focuses specifically on the adult population (≥16 years) within the UK and is embedded within an NHS-led network. 43
Furthermore, Adult SMA REACH integrates closely with the UK SMA Patient Registry to capture patient-reported outcomes, whereas SMArtCARE functions as a standalone platform capturing clinician-reported longitudinal data. Despite these structural differences, both initiatives illustrate how coordinated networks, standardised outcome measures, and multi-centre engagement enable the generation of robust RWE that can address evidentiary gaps in rare diseases and directly support regulatory, reimbursement and clinical-guideline development.
Conclusions
Projects like Adult SMA REACH are possible examples/inspiration for RWD collection and post marketing authorisation; it allows for the identification of gaps in SoC and provides an opportunity to support sites facing barriers to implement care standards. RWD inherently comes with challenges and consideration must be given to ensuring the data is standardised and high quality. Where low patient numbers do not always allow for the ‘gold standard’ randomised controlled trials, natural history and RWD may provide evidence to advance therapy approvals.44–47
Future directions
The Adult SMA REACH project is now in a position to grow, as a ready-made infrastructure to inform research questions in the UK, it is already currently supporting a pregnancy study to evaluate the impact of Nusinersen on pregnant women with SMA (Sponsored by Biogen Global, NCT0578975) and an educational project that aims to increase SMA awareness in primary care and community services. The project is also looking to integrate a comprehensive PPIE program as its scope expands, allowing adults and caregivers to feel included in the conversation again and tailor the direction of the project to what is actually required by the community. The project will continue to support the development and implementation of updated SoC and further work on this will continue under the SMA Care UK project (https://smauk.org.uk/sma-care-uk/).
The sustainability of this project is reliant on funding and collaboration with the multiple stakeholders. We aim to take this project beyond 2027 and continue to inform on the natural history of SMA and further monitor the long-term efficacy and safety of new treatments. We hope to identify trajectories in adults living with SMA taking into consideration the available DMT's, non-drug interventions, shed light on multisystem involvement in SMA and further support the implementation of care standards across the UK.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261433509 - Supplemental material for Adult SMA REACH: A UK clinical network and real-world data collection study for adults living with spinal muscular atrophy
Supplemental material, sj-docx-1-jnd-10.1177_22143602261433509 for Adult SMA REACH: A UK clinical network and real-world data collection study for adults living with spinal muscular atrophy by Jess Page, Elena Karkkainen, Sonia Segovia, Samantha Fitzsimmons, Jose Verdu-Diaz, Lindsay Murphy, Grecia Benesperi, Aleksander Carver, Laura Simms, Stephanie Tanner, Giorgio Tasca, Dionne Moat, Jassi Michell-Sodhi, Robert Muni Lofra, Chiara Marini-Bettolo and on behalf of the Adult SMA REACH clinical network in Journal of Neuromuscular Diseases
Supplemental Material
sj-xlsx-2-jnd-10.1177_22143602261433509 - Supplemental material for Adult SMA REACH: A UK clinical network and real-world data collection study for adults living with spinal muscular atrophy
Supplemental material, sj-xlsx-2-jnd-10.1177_22143602261433509 for Adult SMA REACH: A UK clinical network and real-world data collection study for adults living with spinal muscular atrophy by Jess Page, Elena Karkkainen, Sonia Segovia, Samantha Fitzsimmons, Jose Verdu-Diaz, Lindsay Murphy, Grecia Benesperi, Aleksander Carver, Laura Simms, Stephanie Tanner, Giorgio Tasca, Dionne Moat, Jassi Michell-Sodhi, Robert Muni Lofra, Chiara Marini-Bettolo and on behalf of the Adult SMA REACH clinical network in Journal of Neuromuscular Diseases
Footnotes
Acknowledgments
We would like to thank the Adult SMA REACH clinical network, SMA REACH UK, the UK SMA Patient Registry, and the participating sites for their contributions to the project. Additionally, we would like to acknowledge our Steering Committee who have provided invaluable guidance on the strategic direction of the project. We would also like to thank Biogen and Roche for funding this project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Adult SMA REACH is jointly funded by Biogen UK and Roche UK.
Biogen Idec, Roche Products,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Adult SMA REACH clinical network
The National Hospital for Neurology and Neurosurgery, University College London Hospitals Foundation Trust. St George's University Hospitals NHS Foundation Trust. The Newcastle upon Tyne Hospitals NHS Foundation Trust. King's College Hospital NHS Foundation Trust. The Northern Care Alliance NHS Foundation Trust. University Hospital Southampton NHS Foundation Trust. University Hospitals Birmingham NHS Foundation Trust. Sheffield Teaching Hospitals NHS Foundation Trust. Oxford University Hospitals Trust. North Bristol NHS Trust. Nottingham University Hospitals Trust. Cardiff and Vale University Health Board. NHS Greater Glasgow and Clyde. Cambridge University Hospitals NHS Foundation Trust. The Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust. The Walton Centre NHS Foundation Trust. Leeds Teaching Hospitals NHS Trust. Swansea Bay University Health Board. South Eastern Heath and Social Care Trust.
Chiara Marini Bettoloa, Adult SMA REACH CI & Consultant Neurologist Channa Hewamaddumab, Consultant Neurologist James Lillekerc, Consultant Neurologist Maria Elena Farrugiad, Consultant Neurologist Mariacristina Scotoe, SMA REACH UK PI & Consultant Paediatric Neurologist Clare Galtreyf, Consultant Neurologist Robert Muni Lofraa, Consultant Physiotherapist Portia Thormang, Head of Advocacy and Community Jess Pagea, Adult SMA REACH Project Manager Claire Fitzpatricke, SMA REACH UK Senior Research Coordinator Katie Nevinb, Clinical Specialist Physiotherapist
John Walton Muscular Dystrophy Research Centre, Newcastle University & Newcastle Hospitals NHS Trust. Sheffield Teaching Hospitals NHS Foundation Trust. The Northern Care Alliance NHS Foundation Trust. NHS Greater Glasgow and Clyde. The Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health. St George's University Hospitals NHS Foundation Trust. Spinal Muscular Atrophy UK
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.