
Abstract
Adults with myotonic dystrophy type 1 who require non-invasive ventilation (NIV) often have difficulty with adherence. Few risk factors for non-adherence have been identified, and these are mostly unmodifiable. As part of a quality assurance initiative, we sought to identify psychosocial barriers to NIV adherence to improve supports around isolation and mental health. We found that substance use was associated with non-adherence to NIV in our cohort. Cognitive impairment, the receipt of provincial income support, presence of a psychiatric condition, living alone, and marital status were not associated with NIV adherence. Interventions that limit the impact of substance use may improve NIV in this population.
Keywords
To the editor
People with myotonic dystrophy type 1 (DM1) often develop sleep-disordered breathing requiring non-invasive ventilation (NIV). Between 20 and 54% of people with DM1 will not use or stop NIV for reasons that are not fully understood. 1 This is important because 45% will die of respiratory failure, and non-adherence to NIV is associated with increased mortality. 2
A retrospective cohort study of people with DM1 by Boussaïd et al. showed the following characteristics are associated with adherence to NIV: symptomatic sleep-disordered breathing, a history of acute respiratory failure, professional education, absence of excessive mask leak, and well-functioning ventilators. 3 Unfortunately, this does not give the clinician much guidance on how to improve adherence for an individual patient, except to ensure the ventilator and mask are working appropriately. Subsequently, Vosse et al. showed that cognitive impairment, depressive symptoms, and CTG repeat length do not correlate with NIV adherence. 4 As part of a quality assurance initiative, we sought to determine if psychosocial factors might contribute to non-adherence to NIV in our patients. In this case, additional supports could be offered to address social isolation and mental health to improve adherence and reduce mortality.
We examined the charts of all patients with DM1 currently enrolled in our multidisciplinary clinic for adults with hereditary neuromuscular disorders in northern Alberta. We made use of the provincial electronic medical record, Connect Care, which is used by all hospitals and hospital-affiliated clinics in Alberta. We identified 97 patients with DM1, of which 41 were prescribed NIV and 56 were not. Of those prescribed NIV, 3 were prescribed continuous positive airway pressure (CPAP), and 32 bilevel positive airway pressure (BPAP), and both modalities were considered NIV for the purposes of this chart review. Two individuals had only recently started BPAP (within the last 2 months) and there was insufficient information to determine adherence. Of the remaining 39 people prescribed NIV, the mean age was 45 years at the time of last Pulmonary Medicine assessment (standard deviation 11 years), and 55% were female.
There were a variety of reasons that 56/97 patients were not prescribed NIV. Twenty-eight had preserved respiratory function. Ten were awaiting further diagnostic testing, mainly polysomnography. Seven had not yet had a respiratory assessment or had not been seen for years. Four refused diagnostic sleep testing (for unclear reasons), 2 refused to start NIV as they anticipated they would have claustrophobia, and 1 refused to start NIV for unsupportive spouse. Two were not offered NIV due to severe cognitive impairment. Two were invasively ventilated.
We extracted data regarding adherence and psychosocial parameters from the charts of the 39 patients prescribed NIV. Cost is not a consideration in this population as the equipment is publicly funded. To maintain funding, adherence is defined as at least 4 h per night for at least 70% of nights. 5 We extracted data on the following psychosocial parameters: presence of cognitive impairment, receipt of provincial income support, presence of a psychiatric condition, substance use, living alone, and marital status. Substance use was defined as ongoing use of tobacco, marijuana, or illicit drugs. Alcohol was considered “substance use” if it was described as problematic. Substance use was analyzed separately from other psychiatric disorders since substance use often requires targeted interventions from social workers and primary care providers and may require the involvement of specialized addictions counselors. The presence of cognitive impairment was collected to corroborate Vosse et al.'s finding that non-adherence goes beyond just a lack of understanding. 4 Intelligence quotient is not routinely obtained in our clinic, and the presence of cognitive impairment was determined from informal assessments as documented in the charts. The Bonferroni correction was used for statistical analysis to account for multiple hypothesis testing. Since 6 parameters were tested, a significant p-value would be 0.0083.
The findings are presented in Table 1. In our cohort, substance use was associated with non-adherence to NIV, and no adherent patients had active substance use. Non-adherent patients were less likely to have accessed provincial income support, but this was not statistically significant. Consistent with prior observations, cognitive impairment alone was not associated with reduced adherence. Only 3 patients lived alone, and marital status was not associated with adherence.
Psychosocial parameters and their association with adherence to non-invasive ventilation.
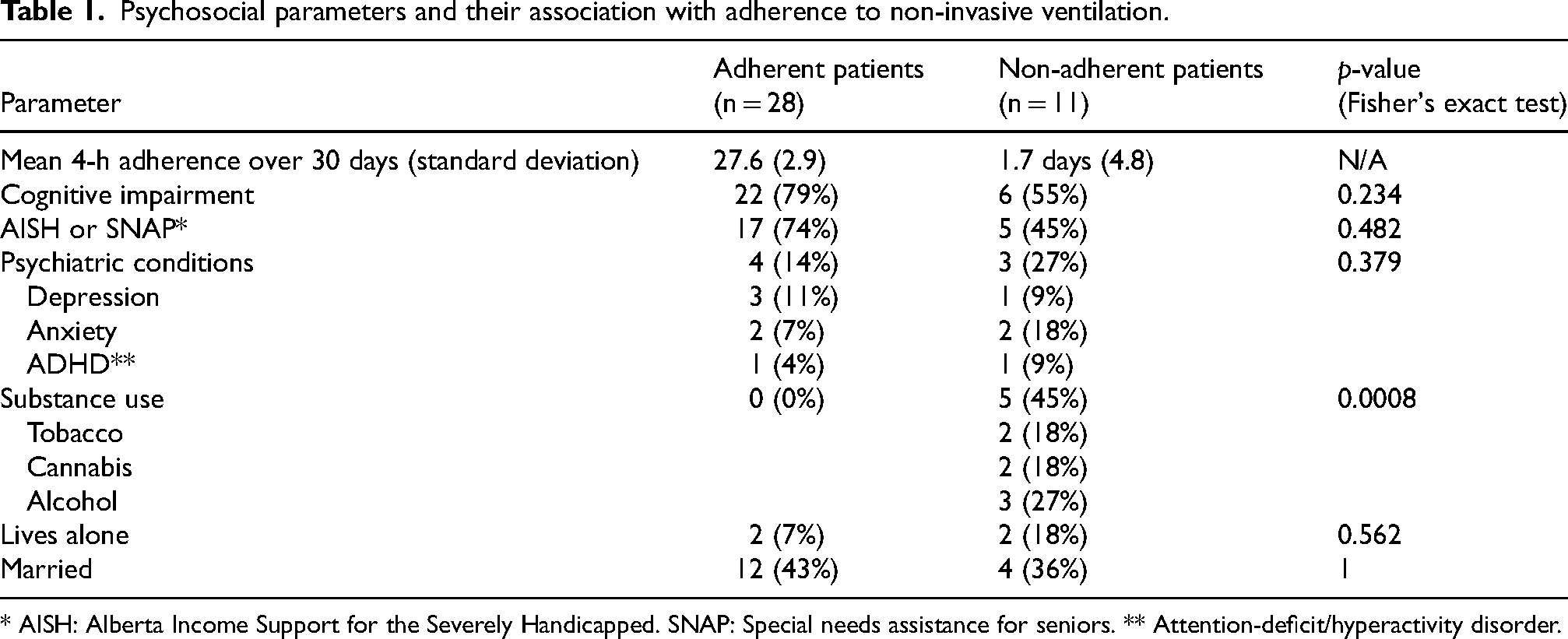
* AISH: Alberta Income Support for the Severely Handicapped. SNAP: Special needs assistance for seniors. ** Attention-deficit/hyperactivity disorder.
We further examined the charts of the 5 people with substance use who were non-adherent to NIV. Two were users of both tobacco and alcohol, 2 were users of cannabis, and 1 of alcohol. Three had comorbid psychiatric disorders (anxiety, depression, or ADHD). Cognitive impairment was described in the charts of 2 of them.
People with DM1 have increased levels of tobacco and illicit drug use, and those with a classic phenotype are at higher risk than those with a mild phenotype. 6 Beauchesne et al. reported that about 22% of patients with DM1 smoked cannabis at their centre. 7 Just over half had poor health status and smoked cannabis to relieve symptoms of DM1. In keeping with this observation, 24/97 people enrolled in our clinic had documented substance use, most commonly marijuana (15/97) and tobacco (14/97). In this respect, non-adherent patients were more like the average patient in our clinic than adherent patients, who had particularly low levels of substance use, and may represent a group with higher levels of social support and coping skills.
People with DM1 have coping strategies that focus more on emotional responses than problem-solving than the general population. 8 This reflects a sense of helplessness when facing a debilitating and progressive condition, in addition to the distinctive personality styles associated with DM1. The interaction between substance use, symptoms, and coping strategies in this population requires further study.
This chart review has several methodologic limitations. The cohort was relatively small, necessitating the grouping of multiple substances into a single category, and limiting the generalizability of the findings. Larger studies would be required to understand any putative association between individual substances and non-adherence to NIV. The rate of psychiatric comorbidities and substance use may be under-reported given these conditions are not the focus of clinic visits and may not be identified. For example, illicit drug use was not reported, and drug testing is not part of our clinical evaluation (recreational cannabis is legal in Canada). Very few patients lived alone, suggesting those who attended clinic had better social supports. The presence of cognitive impairment may be underestimated as it was not formally assessed. Our chart review was not designed to identify barriers to NIV initiation, only to adherence for patients already prescribed NIV.
Although this chart review has limitations, it raises awareness of the potential impact of substance use on the clinical course of people with DM1, and this may be under-recognized. Clinical trials in DM1 may need to account for substance use, which is a plausible confounding factor in NIV adherence and outcomes. Prospective studies are required to determine which substances may reduce NIV adherence, and if interventions tailored to this vulnerable group may improve their respiratory outcomes or quality of life. Hypothetically, these interventions may include referral to support groups, addictions counsellors/psychiatrists, and/or prescription of nicotine replacement therapy.
Footnotes
Acknowledgements
We would like to acknowledge Dr Cecile Phan who provided constructive comments on the manuscript.
Ethical considerations
The requirement for ethics approval was waived by the Human Ethics Research Board of the University of Alberta.
Author contributions
J.M. developed the concept and performed the data extraction and analysis. J.R.E. provided feedback on the clinical context and assisted in manuscript preparation. E.M. provided feedback on the clinical context and assisted in manuscript preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.