
Abstract
We evaluated the safety and effectiveness of onasemnogene abeparvovec (OA) for 34 patients with spinal muscular atrophy (SMA) and tracheostomies enrolled in the RESTORE registry. Most patients (76.5%) received other SMA treatments before and/or after OA. Safety findings were consistent with OA's established profile. There were four fatalities, three caused by respiratory events unrelated to OA, one of unknown cause. Overall, patients exhibited positive motor outcomes, even in cases where the need for tracheostomy emerged after treatment. These real-world data support OA treatment for patients with SMA and tracheostomies and can inform future access, treatment, and care decisions.
Keywords
Introduction
Spinal muscular atrophy (SMA) is a rare, debilitating neuromuscular condition caused by biallelic deletions or mutations of the survival motor neuron 1 (SMN1) gene.1,2 In SMA, motor neuron death causes progressive weakness and atrophy in all skeletal muscle groups, affecting motor, respiratory, and bulbar function. For more severely afflicted individuals, this may result in an inability to breathe, cough, swallow, and communicate effectively, and lead to premature death.3,4 Respiratory support may therefore be required. Although non-invasive methods are generally preferred, sometimes expertise is limited or patients experience adverse events or continued respiratory instability.3,5 In such cases, tracheostomies may provide benefits by allowing direct airway access for more secure ventilation and effective airway clearance.3–5
Three disease-modifying treatments (DMTs) are approved for SMA: nusinersen and risdiplam, which are splicing modifiers of the survival motor neuron 2 (SMN2) “back-up gene,” and onasemnogene abeparvovec (OA), a one-time, intravenous, adeno-associated virus 9 vector-based gene replacement therapy that delivers a fully functional copy of human SMN cDNA into target cells.6–8 These treatments have demonstrated safety and efficacy in clinical trials; however, patients with tracheostomies were excluded.9–16
This evidence gap leads to concerns around the safety and efficacy of DMTs for this vulnerable patient population, and substantial real-world consequences. 4 Some studies equate tracheostomy placement after treatment with death, using this composite endpoint in association with treatment failure.9–11,13,14,17 In many countries, patients may need to choose between tracheostomy or treatment if tracheostomy is an exclusion or stopping criteria for DMT reimbursement. 18 However, it is possible that respiratory symptoms can occur independently while motor symptoms improve or stabilize. In clinical practice, safety concerns and low expectations regarding DMT benefits may influence treatment and care strategies.3,19,20 These health disparities may lead to missed opportunities for preventative care for this population.
Data are needed to enable evidence-based reimbursement criteria and guide treatment and care decisions for patients with SMA in need of respiratory support via tracheostomy. Thus, we evaluated the safety and effectiveness of OA for patients with SMA who received tracheostomies either before or after OA treatment in RESTORE, a large international registry.17,21
Methods
RESTORE (NCT04174157, registration September 12, 2019) is a prospective, multicenter, multinational, non-interventional registry of patients (N = 589; data cutoff date December 2023) with genetically confirmed 5q SMA. Detailed methods have been published.17,21 Data are presented here for patients grouped based on timing of tracheostomy placement relative to OA treatment.
Data for demographics and clinical characteristics, including presence of tracheostomy, were collected. Safety data were recorded during the observation period. Treatment-emergent adverse events (TEAEs), serious TEAEs, and TEAEs of special interest (transient thrombocytopenia, cardiac adverse events, hepatotoxicity, and thrombotic microangiopathy) were reported.
Patients were assessed for motor milestones and motor function using the Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND), Hammersmith Functional Motor Scale – Expanded (HFMSE), and Hammersmith Infant Neurological Examination – Section 2 (HINE-2), and categorized according to SMA treatment regimen.22–24 Patients were included in the effectiveness analysis if they had assessments at two or more time points for a specific motor test during the observation period (with at least one after OA administration).
Results
Patient population
RESTORE included 34 patients with tracheostomies (14 before OA, 20 after OA), of which 19 (55.9%) were male and 33 (97.1%) had two SMN2 gene copies. One patient had one SMN2 copy (Patient 10, Figure 1B). Although four patients were identified via newborn screening, all were symptomatic at diagnosis (Supplementary Table 1). The mean (SD) age at diagnosis was 4.14 (3.7) months for patients who received tracheostomy before OA (n = 14), and 4.05 (3.1) months for patients who received tracheostomy after OA (n = 20). Eight patients (23.5%) received OA monotherapy, and 26 patients (76.5%) received other DMTs (i.e., nusinersen, risdiplam) before and/or after OA.
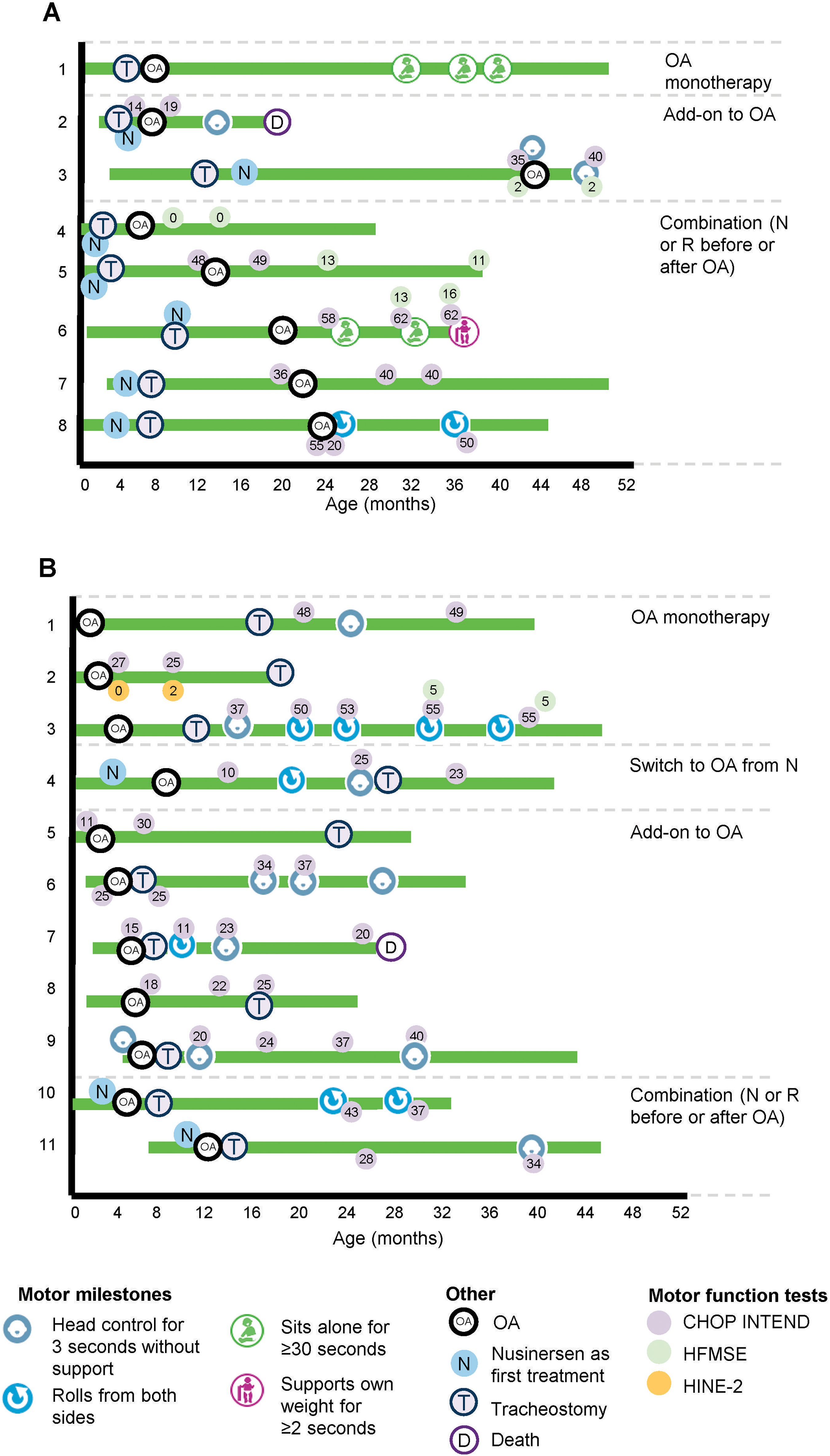
Patient journeys for patients with SMA and tracheostomy in RESTORE before (A) or after OA (B). Data as of December 2023. Includes patients who had assessments at two or more time points for a specific motor test, with at least one after OA. Patients were grouped based on timing of tracheostomy placement relative to OA treatment. Motor milestones were assessed according to the WHO MGRS and Bayley Scales of Infant and Toddler Development III. Motor function was assessed via CHOP INTEND, HFMSE, and HINE-2 scores. CHOP INTEND, Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders; HFMSE, Hammersmith Functional Motor Scale – Expanded; HINE-2, Hammersmith Infant Neurological Examination – Section 2; N, nusinersen; OA, onasemnogene abeparvovec; R, risdiplam; SMA, spinal muscular atrophy; WHO MGRS, World Health Organization Multicentre Growth Reference Study.
Safety
TEAEs of any grade and Grade 3 or greater were reported for 25 (73.5%) and 23 (67.6%) patients, respectively (Table 1). Four of the 21 serious TEAEs reported (19%) were considered OA-related. There were four deaths, three of which were due to respiratory failure and not deemed to be treatment related. The cause of death of the fourth patient is unknown. Two of the patients who died were assessed for motor function (discussed below).
OA safety for patients with SMA and tracheostomy from RESTORE.
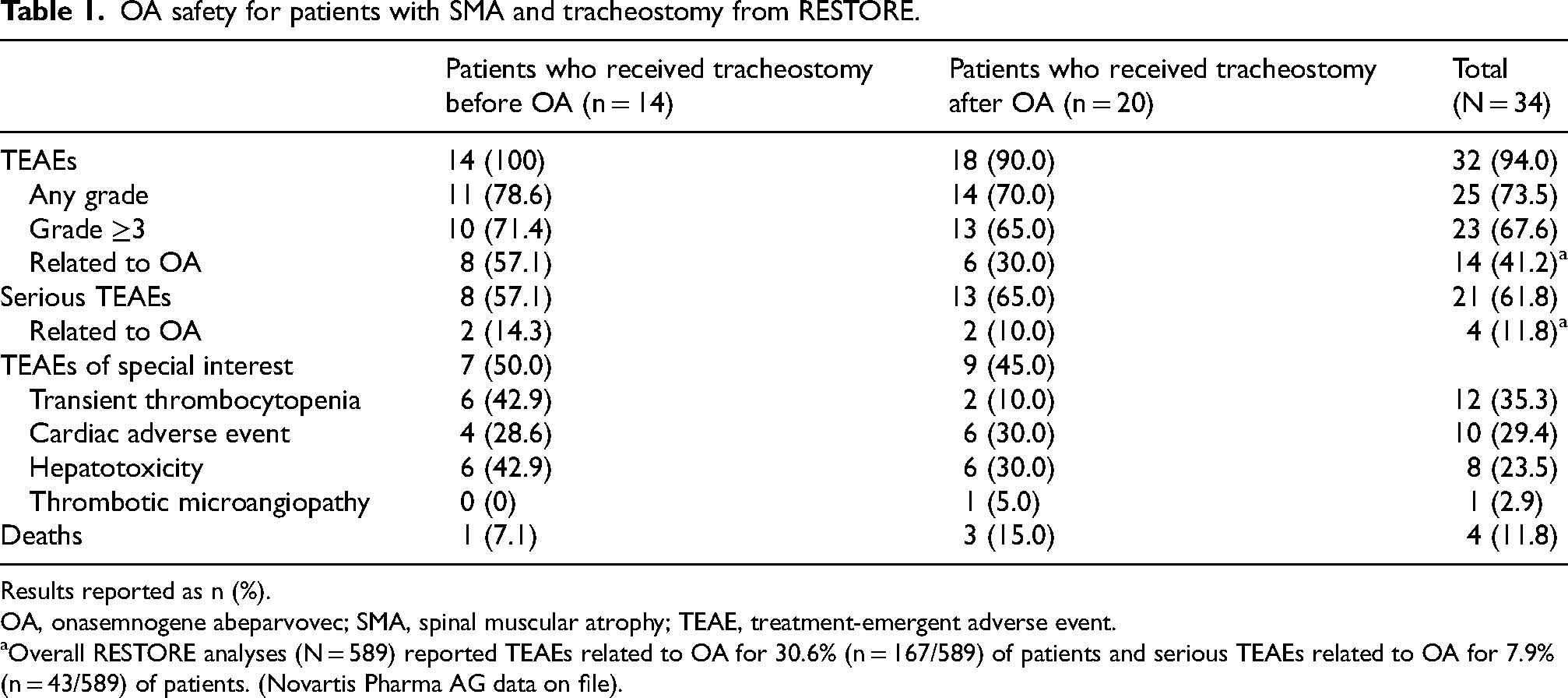
Results reported as n (%).
OA, onasemnogene abeparvovec; SMA, spinal muscular atrophy; TEAE, treatment-emergent adverse event.
Overall RESTORE analyses (N = 589) reported TEAEs related to OA for 30.6% (n = 167/589) of patients and serious TEAEs related to OA for 7.9% (n = 43/589) of patients. (Novartis Pharma AG data on file).
Effectiveness
Tracheostomy before OA
Of 14 patients with tracheostomies placed before OA, eight had assessments at two or more time points for a specific motor test. Of those, seven patients (87.5%) maintained or achieved new motor milestones and/or had stable/improved motor function test scores on at least one instrument after OA (Figure 1A). One exception was Patient 4, who recorded two HFMSE scores of 0 but was not assessed with CHOP INTEND. Two patients (Patients 5 and 8) demonstrated inconsistencies across instruments. One fatality was reported; Patient 2, who gained head control and a 5-point increase in CHOP INTEND, died at 20 months of age due to respiratory failure.
Tracheostomy after OA
Of 20 patients with tracheostomies placed after OA, 11 had assessments at two or more time points for a specific motor test. Of those, all patients (100%) maintained or achieved new motor milestones and/or had stable/improved motor function test scores on at least one or more instruments after OA (Figure 1B). Two patients (Patients 2 and 10) demonstrated inconsistencies across instruments. There was one fatality; Patient 7, who had an overall 5-point increase in CHOP INTEND, died at 28 months of age due to respiratory failure.
Discussion
Data from RESTORE indicate a positive safety and effectiveness profile of OA for patients with SMA and tracheostomies. Compared with patients without tracheostomies, no increased incidence of TEAEs was observed for those who received OA before or after tracheostomy, or for those who received combination versus monotherapy. 17 Although response was variable across treatment regimens, nearly all patients demonstrated a positive motor response ranging from stabilization to substantial improvement and the majority acquired new motor milestones, which is consistent with previous findings for patients with SMA and tracheostomies. 25 This positive motor response was also observed for those who received tracheostomy after treatment, even when considering only the motor assessments after tracheostomy placement, and demonstrates that emerging tracheostomy needs should not be equated with generalized treatment failure, as most patients continued to benefit from treatment. This finding contrasts with natural history data in which motor and respiratory function strongly co-vary, 26 and instead may suggest that tracheostomies could provide these patients with the additional support needed to safely cope with respiratory challenges and continue to thrive under treatment.
For the four patients who died, two had been assessed for motor performance and demonstrated improvements, suggesting that general treatment failure was not a factor in these deaths. Instead, these patients died due to respiratory events, indicating that respiratory crises may continue to pose substantial risks for some children with SMA and tracheostomies. 19 However, for patients without tracheostomies, real-world data and post-hoc analyses of OA clinical trial data generally confirmed stabilized or improved respiratory and bulbar function after treatment with OA,27–30 and a study of patients with tracheostomies demonstrated evidence for stable or reduced ventilatory support, airway secretions, and respiratory hospitalization rates, and stable or improved cough function after OA treatment.25,31 Together, these findings emphasize the importance of continued high-level multidisciplinary care, but also suggest that, with time, OA may reduce respiratory vulnerability and increase survival for children with tracheostomies.
Finally, our analysis revealed that all patients in RESTORE with tracheostomies were severely symptomatic at diagnosis and treatment initiation, indicating that, despite advancements in treatments and standards of care, tracheostomies continue to contribute to the clinical management of children with respiratory needs. In addition, all but one patient with tracheostomies had two SMN2 copies (the remaining patient had one SMN2 copy) and only four patients (12%) were diagnosed through newborn screening, compared with 61% and 46%, respectively, in the overall OA-treated RESTORE population (Novartis, data on file). This demonstrates an increased probability for tracheostomy need in severe genotypes, which can be reduced with early diagnosis and treatment initiation.
The main limitation of this study is that respiratory and tracheostomy-specific outcomes were not collected; therefore, evidence of OA treatment effects on these outcomes is lacking.
Other limitations include the small number of patients (most of whom were from the United States), incomplete baseline and follow-up data (including motor function tests), inconsistencies across various motor function tests and potential inconsistencies in testing methods, and limited follow-up period (<6 months) for some patients.
Conclusion
For patients with SMA and tracheostomies, unanswered questions regarding safety and continued effectiveness of DMTs have led to substantial real-world consequences such as limited treatment access. 18 These data from RESTORE indicate that patients with tracheostomies who were treated with OA demonstrated no increased safety risks compared with other children with SMA and, overall, exhibited positive motor outcomes regardless of whether they received other treatments before or after OA. Importantly, patients who received a tracheostomy after OA continued to respond positively to treatment, indicating that emerging tracheostomy needs after treatment should not be equated with general treatment failure. These findings suggest a positive benefit-risk profile for treatment in this population, which can guide future access, treatment, and care decisions.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251395173 - Supplemental material for Trach and treat: Safety and motor outcomes following onasemnogene abeparvovec in patients with spinal muscular atrophy and tracheostomies in the RESTORE registry
Supplemental material, sj-docx-1-jnd-10.1177_22143602251395173 for Trach and treat: Safety and motor outcomes following onasemnogene abeparvovec in patients with spinal muscular atrophy and tracheostomies in the RESTORE registry by Yasemin Erbaş, Laurent Servais, Perry B Shieh, Natalie L Goedeker, Megan A Waldrop, Ryosuke Bo, Dheeraj Raju, Kamal Benguerba, Sandra P Reyna, David Wolff and Richard S Finkel in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
The authors wish to thank the investigators, site coordinators and study teams, and, most importantly, the patients, families, and caregivers for their willingness to participate in RESTORE, which is sponsored by Novartis Pharma AG.
Ethical considerations
RESTORE is being conducted in accordance with established research principles, local treatment practices and regulations, and guidelines of the International Council on Harmonisation. All information obtained during the conduct of the Registry with respect to the patient's identity or state of health will be treated as confidential. Prior to any disclosure of protected personal information, a signed written agreement will be obtained from the patient or his/her legal representative.
Author contributions
As stipulated in the RESTORE bylaws, all publication topics were authored and approved by the members of the steering committee, and analyses were performed by statisticians employed by the CRO that manages the study data. All authors had access to and analyzed and interpreted the data, participated in the development and critical review of the manuscript, approved the final version of the manuscript submission for publication, and are accountable for the accuracy and integrity of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Novartis Pharma AG, Basel, Switzerland. Editorial and medical writing support were provided by Caryne Craige, PhD, of Kay Square Scientific, Butler, PA, USA. This support was funded by Novartis Pharma AG, Basel, Switzerland.
Declaration of conflicting interest
Data availability
The data sets generated and analyzed during the study are available from the RESTORE registry. These data sets are not publicly available, but are available from the corresponding author/RESTORE Steering Committee on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.