
Abstract
Background
Neuromuscular diseases (NMDs) encompass a diverse range of disorders that impair muscle function, often leading to progressive weakness and loss of independence.
Objective
This systematic review aims to synthesize research on how virtual reality (VR) and gamified rehabilitation approaches enhance patient engagement and outcomes, ultimately reshaping rehabilitation practices for individuals with NMDs.
Methods
Studies were identified from an online search of PubMed, Web of Science, and Embase databases with a search time range from 2014 to 2024. This review has been registered on Open OSF (n) RCNHE.
Results
Robotics, VR, and biofeedback, in turn, enriched by gamification, represent the improvement of motor function, motivation, and psychosocial well-being within rehabilitation concerning NMDs. Using emerging technologies seems promising to improve engagement, delay functional decline, and enhance quality of life.
Conclusions
This systematic review identified that VR and gamification provide the potential to enhance rehabilitation outcomes in patients suffering from NMDs. The future will doubtless have more subjects included and optimization of interventions to best personalize treatments, hence best practice recommendations can be made towards wider clinical implementations.
Introduction
Neuromuscular diseases (NMDs) represent an heterogeneous group of disorders that impair muscle function, often due to peripheral nervous system dysfunction involving muscles, neuromuscular junctions, or motor neurons. 1 Most NMDs are often characterized by slow progression, leading to muscle weakness and, in advanced cases, respiratory or cardiac failure. 2 These include muscular dystrophies, motor neuron diseases, peripheral neuropathies, and myasthenias. Prevalence rates vary amongst the conditions. For example, Duchenne Muscular Dystrophy (DMD) occurs in approximately 1 in 3500 to 5000 male births worldwide, while Becker Muscular Dystrophy is less common.3,4 On the whole, NMDs are diagnosable at any age, though many forms are diagnosed early in childhood, such as in DMD, while other forms, such as amyotrophic lateral sclerosis, do not appear until adulthood.5,6 NMDs’ rehabilitation focus on managing symptoms and improve quality of life, mobility, and functional independence. 7 Since many NMDs are progressive, rehabilitation often requires adjustments over time. 8 A multidisciplinary approach is therefore necessary, based on physical therapy, occupational therapy, respiratory care, and sometimes speech therapy. 9 In this perspective, rehabilitation through VR can become an additional possibility. 10 Nowadays, the rehabilitation of NMDs using VR is gaining wide importance because it enhances patient engagement, personalizes therapy, and opens new dimensions for improving motor function.11,12 VR-based rehabilitation offers immersive, adaptive environments that simulate real-life activities, addressing the repetitive and physically demanding nature of traditional rehabilitation, especially for NMD patients.13,14 Numerous studies highlight VR's ability to improve motor functions, balance, and coordination in NMD patients, including those with muscular dystrophy, peripheral neuropathies, and amyotrophic lateral sclerosis (ALS).15,16 Mondellini et al. investigated immersive VR applications designed for cognitive training in patients suffering from NMDs. 17 The findings presented that the VR exposure was very engaging and effective in terms of cognitive stimulation, and might support motor rehabilitation due to the improvement in cognitive-motor integration. The patients were noted to be more motivated and took active participation, which is one of the major key factors of long-term rehabilitation. 17 A systematic review of the trends of robot-assisted and VR-assisted neuromuscular therapy was performed by Baur et al. in 2018 by going through multiplayer health-related games. 18 The results pointed out the many advantages of multiplayer VR systems, promoting social interaction, collaboration, and competition among patients, thus enhancing motivation and adherence to rehabilitation programs. 18 This review suggests that robotic-assisted VR is also a more holistic programme that addresses both motor and cognitive recovery, making rehabilitation more appealing and successful for these neuromuscular patients. 18 Another critical aspect of VR rehabilitation is its ability to provide real-time feedback by recording movement patterns, muscle activity, and balance. This aspect is essential to allow the clinician to follow the patient's improvement more closely, to make any necessary adjustments to the exercises and, consequently, to improve the therapeutic outcome.19–21 These can then be used to perform personalized treatment plans, hence rehabilitation is more purposeful and efficient. 22 Gamified VR transforms repetitive exercises into engaging challenges, significantly boosting patient motivation and active participation. 23 It involves challenges, rewards, and levels, all of which are included in VR to make traditional rehabilitation exercises interactive, and more playful than therapeutic. This is important for patients who often experience fatigue and lack of motivation due to their clinical condition. 24 This is particularly useful in paediatric populations where interest in therapy can be difficult to maintain. 25 The effectiveness of enhancing rehabilitation programmes has been demonstrated in several studies, as a patient may be more compliant with their therapy if it is fun. 26 Therefore, gamification within VR enhances therapeutic processes and supports neuroplasticity for better recovery of motor function in individuals with NMDs. 27 In support of the above, Deutsch's study shows great efficacy of VR and gamification in the rehabilitation of NMDs. 27 It focuses on how the use of VR and gaming systems can improve walking and mobility in people with musculoskeletal and neuromuscular conditions. 27 Moreover, Deutsch's study concludes that traditional rehabilitation can be quite monotonous and less engaging for patients, so by integrating gaming elements into therapy, patients are encouraged to participate more actively in their rehabilitation process. 27 The results show that exposure to VR games leads to increased mobility and, depending on the NMD, walking, as the interactive and fun nature of these games acts as a stimulus that makes patients more willing to practice and continue their rehabilitation programmes. 28 It should also be mentioned that gamified VR environments strongly enhance motor learning through repetition in a highly motivating and conduction-enhancing environment. 29 This particular aspect is very important, since conventional repetitive rehabilitation exercises can easily become boring and demotivating, leading to reduced participation and less effective rehabilitation. 30 Moreover, VR allows patients to target certain movements that are specifically chosen within the personalized rehabilitation program: with targeted practice, they refine their movements, improving precision and control, by performing actions applicable to real-life motor skills. 31 The VR setting itself reduces the possibility of injury, as patients can safely explore their limits in ways that are often not possible in traditional settings.32–34 A synthesis of the aspects of VR and gamification in neuromuscular rehabilitation is shown in Figure 1.
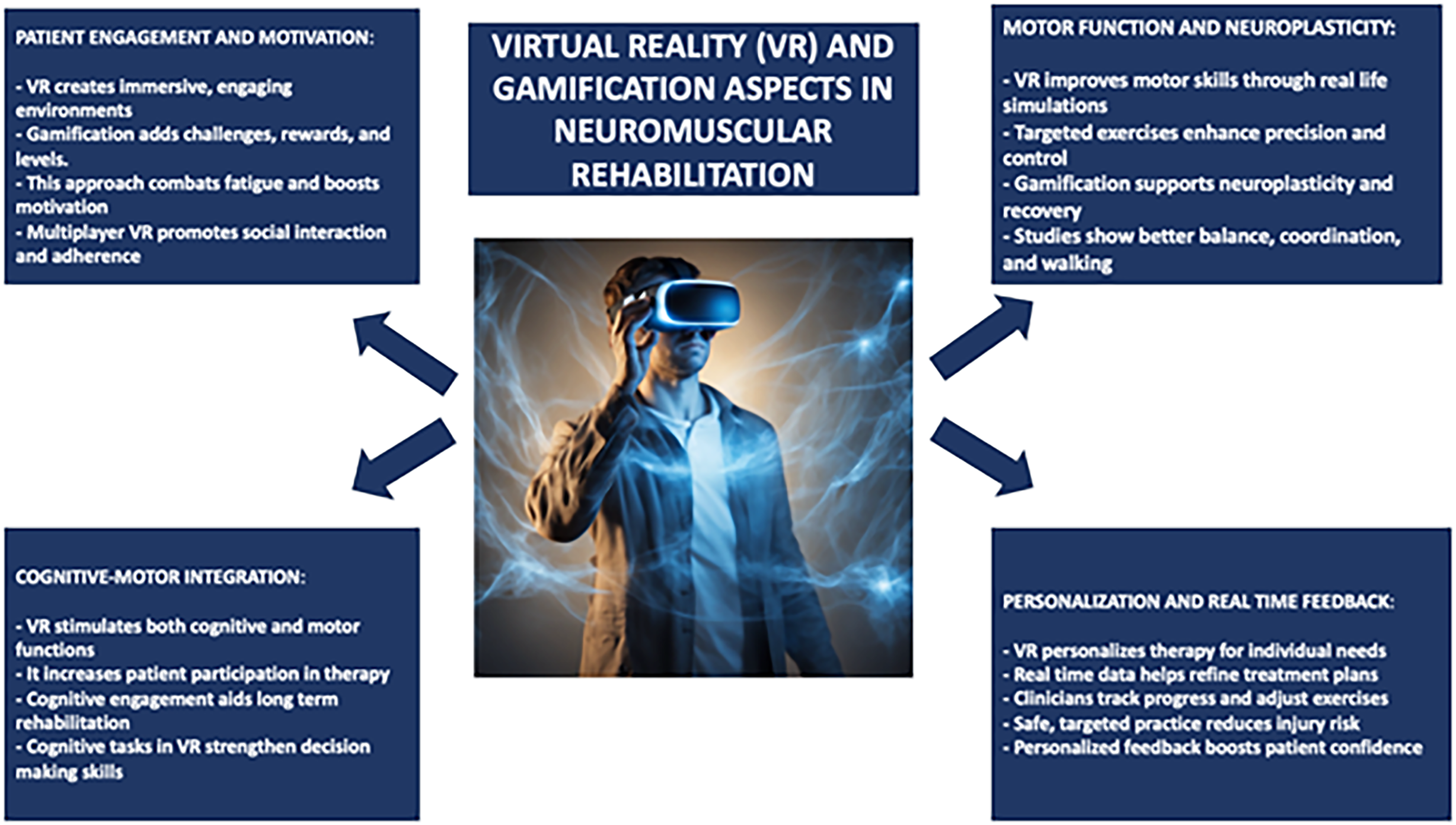
VR and gamification aspects in neuromuscular rehabilitation.
The current systematic review aims to synthesize the existing research on
Materials and methods
Search strategy
A comprehensive literature search was performed using PubMed, Web of Science, and Embase databases, employing the keywords: (All Fields: “Neuromuscular Diseases”) AND (All Fields: “Virtual Reality”) OR (All Fields: “Gamification Rehabilitation”) with a search time range from 2014 to 2024. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram was applied to outline the process (identification, screening, eligibility, and inclusion) for selecting relevant studies, as illustrated in Figure 2. Titles and abstracts from the database searches were independently reviewed. Articles were evaluated for their relevance based on predefined inclusion criteria. All titles and abstracts meeting these criteria were fully screened. Multiple teams of experts independently selected articles and analysed data to minimise bias, and disagreements were discussed until consensus was reached. This review has been registered on Open OSF (n) RCNHE.
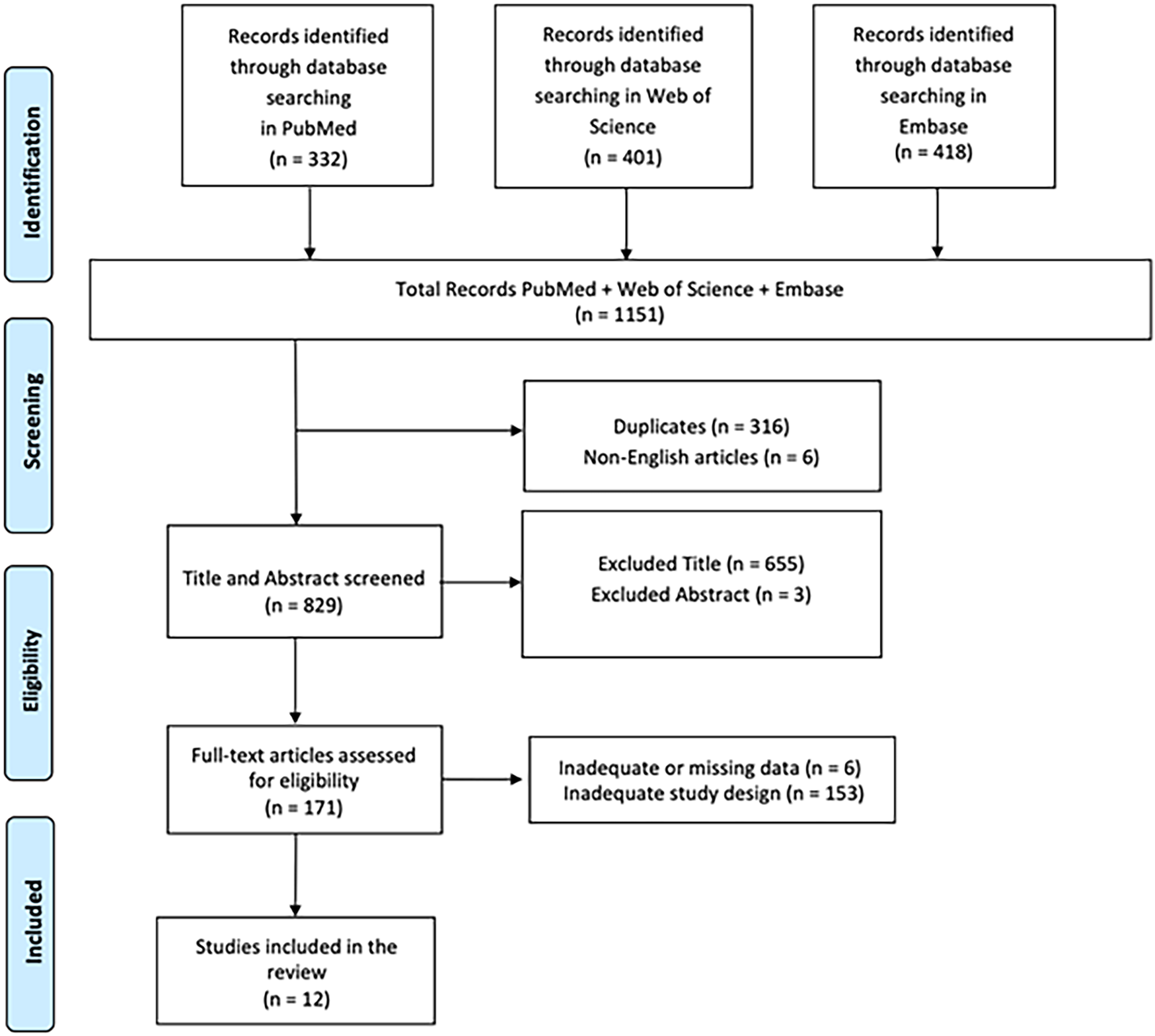
PRISMA 2020 flow diagram of evaluated studies.
PICO evaluation
We applied the PICO model (Population, Intervention, Comparison, Outcome) to create our search terms. The population consists of patients suffering from different NMDs and enrolled in rehabilitation programmes. The intervention will be VR, technological tools and gamified techniques newly designed to enhance the rehabilitation process. Comparisons will be performed with traditional rehabilitation, without such advanced technologies. Each outcome would therefore be considered in terms of improving functionality, patient participation and rehabilitation efficiency.
Inclusion criteria
We only included studies conducted in human populations and published in English that met the following criteria: (i) original or protocol studies of any type; and (ii) articles investigating how VR, technologies, and gamified rehabilitation approaches influence patient outcomes and engagement in NMD rehabilitation.
Exclusion criteria
A study was excluded if it lacked data or information on how VR, technology and gamified rehabilitation approaches influence patient outcomes and engagement in NMD rehabilitation. Systematic, integrated or narrative reviews were also excluded, but their reference lists were reviewed and included if relevant. Articles written in languages other than English were also excluded.
Results
Quality of included studies – risk of bias
We assessed the risk of bias using appropriate tools based on the design of the included studies.
Of the twelve studies, three were randomized controlled trials (RCTs).35–37 For these, we used the updated Cochrane Risk of Bias (RoB 2) tool, which covers five domains: (i) bias arising from the randomization process, (ii) bias due to deviations from the intended intervention, (iii) bias due to missing data on the results, (iv) bias in the measurement of the outcome and (v) bias in the selection of the reported result (Figure 3). 38 Our assessment identified numerous studies with moderate risk of bias and modest methodologies. In all three studies, we identified some concerns due to deviations from the intended intervention (D2).35–37
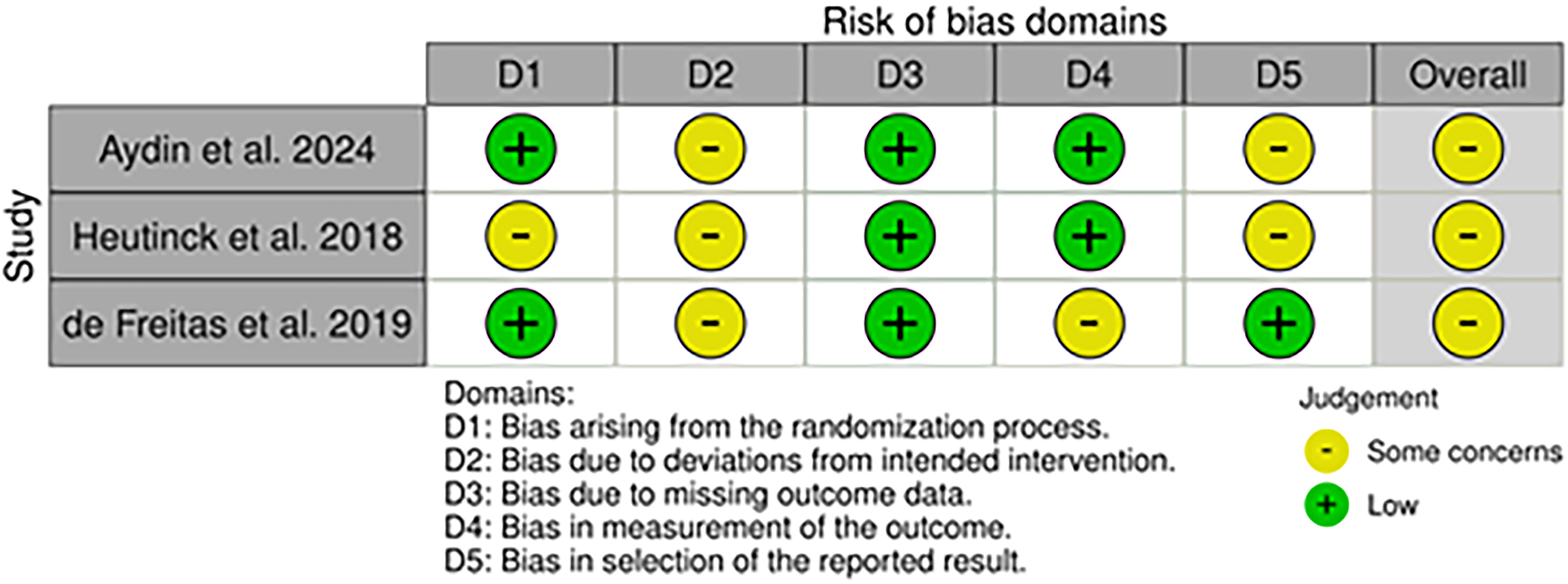
Risk of bias (RoB2) of included RCT studies.
We applied the ROBINS-I tool and identified nine non-randomized studies: two were comparative studies,39,40 one quasi-experimental study, 41 one mixed methods study, 42 one feasibility study, 43 one experimental study, 44 one cross-sectional study, 45 one interventional study, 46 and one evaluation study. 47 Moreover, ROBINS-I assesses bias in seven areas: (i) bias due to confounding, (ii) bias in participant selection, (iii) bias in classification of interventions, (iv) bias due to deviations from intended interventions, (v) bias due to missing data, (vi) bias in outcome measurement, and vii) bias in selection of the reported outcome (Figure 4). 48 However, the ROBINS-I ratings of the nine studies indicate a generally moderate methodological quality, although each study has notable areas of concern. Garmendia et al. demonstrate a lower overall risk of bias, reflecting relatively strong internal validity and robust study designs. 45 However, Malheiros et al., 39 Barragan et al., 41 Quadrado et al., 40 Eckert et al., 43 Silveira et al., 44 Maresca et al. 46 and Al-Mfarej et al., 47 demonstrate a moderate overall risk of bias thanks to selections of participants. Malheiros et al., 39 Maresca et al., 46 and Al-Mfarej et al. 47 present a moderate risk in domains D1 (bias due to confounding) and D6 (bias in outcome measurement), while Barragan et al. 41 showed a moderate risk also in D3 (bias in the classifications of interventions). Barragan et al., 41 Quadrado et al., 40 Oldford et al., 42 and Eckert et al. 43 presented serious risks in D1 (bias due to confounding). Only Oldford et al. 42 had a serious risk in D1, D2, and D7 (bias in the selection of results). In contrast, all studies except Barragan et al., 41 had a low risk of bias in D2 demonstrating a good methodology in selecting participants. Eckert et al. 43 and Silveira et al. 44 present a moderate overall risk of bias, suggesting more substantial methodological limitations. Eckert et al. 47 show a moderate risk in D2, D4, and D6, while Silveira et al. 48 show a moderate risk in D1, D2, D4 (bias to deviations from intended interventions) and D5 (bias due to missing data). These areas highlight potential data integrity, measurement, and reporting accuracy vulnerabilities. Overall, while most studies show a moderate risk of bias in several domains, specific areas such as confounding variables, outcome measurement, and participant selection remain critical to examine to ensure the reliability and validity of the study results.
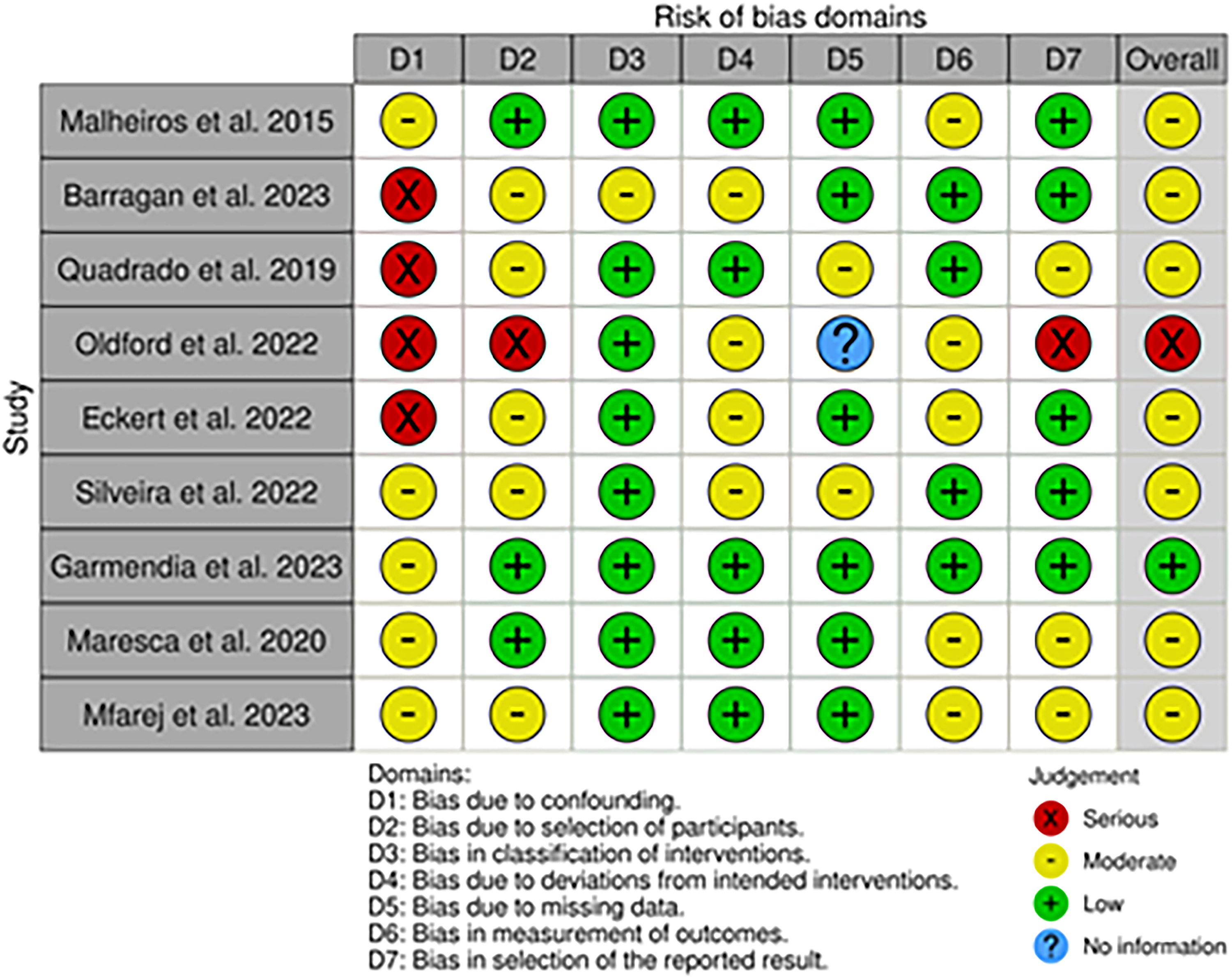
Cochrane risk of bias in non-randomized studies of interventions (ROBINS-I).
Synthesis of evidence
In total, 1151 articles were found: 316 articles were removed due to duplication after screening; 6 articles were excluded because they were not published in English; 658 articles were excluded based on title and abstract screening. Finally, 159 articles were removed, based on screening for inadequate and untraceable study designs (Figure 2). Therefore, twelve research articles met the inclusion criteria and were included in the review. These studies are summarized in Table 1.
Summary of studies included in the research.
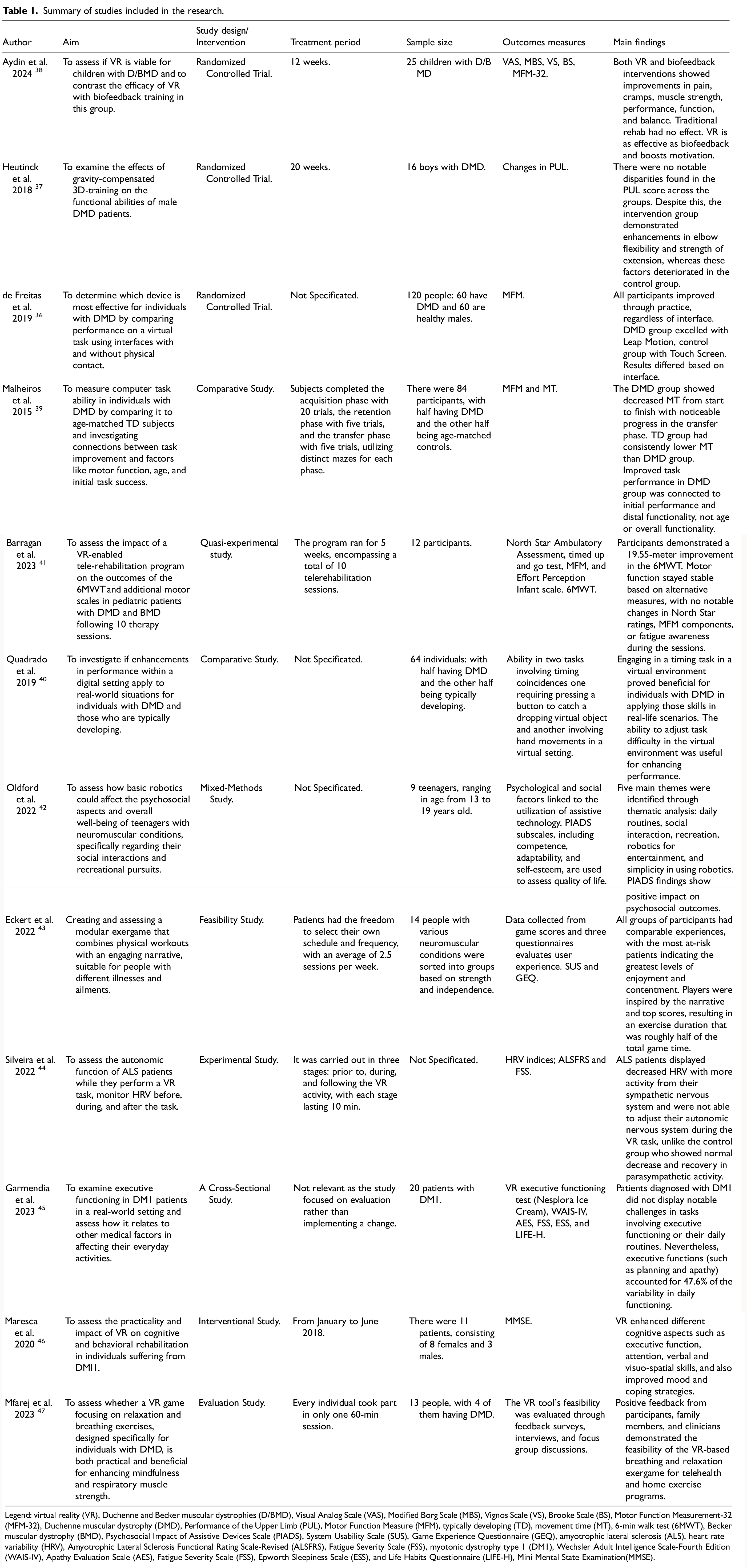
Legend: virtual reality (VR), Duchenne and Becker muscular dystrophies (D/BMD), Visual Analog Scale (VAS), Modified Borg Scale (MBS), Vignos Scale (VS), Brooke Scale (BS), Motor Function Measurement-32 (MFM-32), Duchenne muscular dystrophy (DMD), Performance of the Upper Limb (PUL), Motor Function Measure (MFM), typically developing (TD), movement time (MT), 6-min walk test (6MWT), Becker muscular dystrophy (BMD), Psychosocial Impact of Assistive Devices Scale (PIADS), System Usability Scale (SUS), Game Experience Questionnaire (GEQ), amyotrophic lateral sclerosis (ALS), heart rate variability (HRV), Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised (ALSFRS), Fatigue Severity Scale (FSS), myotonic dystrophy type 1 (DM1), Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV), Apathy Evaluation Scale (AES), Fatigue Severity Scale (FSS), Epworth Sleepiness Scale (ESS), and Life Habits Questionnaire (LIFE-H), Mini Mental State Examination(MMSE).
The studies discussed in this review examine how VR, technologies, and gamified rehabilitation approaches influence patient outcomes and engagement in NMD rehabilitation. Five papers explored robotics, gamification, and VR in neuromuscular rehabilitation42–46; while seven papers analyzed gamified VR and biofeedback techniques in the rehabilitation of Duchenne and Becker muscular dystrophy.35–37,39–41
The intersection of robotics, gamification, and VR in neuromuscular rehabilitation
The progressive potential of robotics and VR in improving the psychosocial and cognitive aspects of NMD rehabilitation is emerging through several research studies. This aspect is further enhanced by the use of gamification to increase engagement and motivation in such patients. Oldford and colleagues emphasize the positive impact of simple robotics on psychosocial well-being and quality of life in adolescents with NMD. Adolescents often lack access to social and recreational activities, but robotics can offer new ways for them to be engaged. Through a mixed-methods approach, they found that robotics can improve socialization, leisure, and personal adaptability. Thematic analysis revealed benefits such as ease of use and leisure activity. Participants reported improvements in competence, adaptability, and self-esteem. The study suggests that tailored robotics can promote social inclusion at home, with the potential for gamified rehabilitation to enhance engagement. 42 In another paper, a modular exergame method was proposed, focusing on personalized physical exercises to be integrated into motivational stories. The study was called “Blexer-med”, and used the principle of motion capture with various adaptability in neuromuscular conditions. Four exercises can be adapted via a therapeutic web platform, used for personalized interventions. Tested on 14 patients with various states of strength and independence, the research showed consistency in experiences between groups, the most fragile subjects showed the highest satisfaction. The gamification components (score, storyline) motivated players to use it on average 2.5 times per week for 20 min. The gameplay was an active exercise for about half of the time; the concept was viable, but improvements in 3D design are needed for greater engagement and enjoyment. 43 In an experimental study, the feasibility of using VR as an intervention for ALS patients is explored. The ALS patients were tasked to analyze the autonomic functionality concerning performing the VR task using their upper limbs. Heart rate variability (HRV) was measured before, during, and after the 10-min VR task. The findings indicated that there were significant differences in HRV between the ALS patients and healthy controls. There was diminished HRV, along with sympathetic nervous system predominance, in ALS. Healthy controls showed normal autonomic responses during the task and recovery. This study postulated that VR therapy may have an effect on the autonomic functioning of ALS patients and be a novel rehabilitation approach; however, further research is needed on the effectiveness of VR in ALS rehabilitation. 44 A cross-sectional study examined executive performance in a group of myotonic dystrophy type 1 (DM1) patients using the VR test Nesplora Ice Cream, complemented with additional cognitive and self-report measures. 45 Although no significant difficulties in executive tasks or daily functioning in DM1 patients were detected, this research underlined the contribution of both “cold” (cognitive) and “hot” (emotional) executive functions to daily life. 45 Planning ability and levels of apathy emerged as significant predictors of functional performance, accounting for 47.6% of the variance. 45 This represented the first study using VR in the evaluation of executive functions in DM1, hence potentially opening discussions concerning the true extent of impairment in this population. 45 Maresca et al. explored the use of VR training in cognitive and behavioral rehabilitation in patients with DM1. 46 Eleven patients underwent a neurorehabilitation program using the traditional form of cognitive therapy and training with the Khymeia VR Rehabilitation System. 46 Changes in executive function, attention, verbal and visuospatial skills, mood and coping were significantly improved. The fact that VR is highly interactive, offering immersive experiences and gamification, is likely to have contributed to increased engagement and motivation. These results show that cognitive rehabilitation using VR can improve both cognitive and behavioural outcomes, thereby improving the quality of life of these patients. 46 Robotics and VR, enriched by gamification features, therefore have a great potential to further both psychological and cognitive rehabilitation in neuromuscular patients and could point to future directions in individualized and more engaging therapeutic interventions.
Gamified VR and biofeedback: a promising path for Duchenne and Becker muscular dystrophy treatment
Scientific literature reports, with an increasing number of cases, VR and biofeedback as new approaches to the treatment of Duchenne and Becker muscular dystrophy in children, thus opening new frontiers for motor skills and patient compliance. A randomized controlled trial explored the use of VR training and biofeedback in children with Duchenne and Becker muscular dystrophies. 35 Children participated in a randomized controlled trial for 12 weeks: group 1 VR training, group 2 biofeedback training, and group 3 control. Changes in muscle strength, pain intensity, cramp severity, functional performance, and balance were significant in both groups when using either VR or biofeedback compared to their matched controls, who did not experience any changes. 35 In turn, VR proved no worse than biofeedback but had one advantage in maintaining children's motivation for rehabilitation. Thus, such results confirm that VR and biofeedback are promising approaches to enhance rehabilitation for children with Duchenne and Becker muscular dystrophies. 35 A second randomized controlled trial investigated the effect of gravity-compensated 3D training on upper extremity function in boys with DMD. Boys with DMD who used dynamic arm support during VR gaming for 20 weeks showed improvements in elbow range of motion and extension strength compared to controls who received standard care. Although upper limb scores remained stable, these results highlight that this strategy may postpone deterioration in functional capacity by using improvements in range and strength. 35 VR training with dynamic arm supports may help maintaining upper extremity function, suggesting its potential value in a rehabilitation strategy in DMD. 37 De Freitas et al. studied using three VR interfaces, Kinect®, Touch Screen computer, and Leap Motion®, to improve motor performance in DMD patients. The total sample included 120 participants, with DMD patients and controls. 36 The results indicated an overall improvement with practice for all participants, but those with DMD performed worse than controls. More importantly, the improvements observed with the Leap Motion interface in the DMD group were found to be significantly better than other interfaces, allowing for better distal function and adaptability. 36 This would therefore indicate that Leap Motion-based VR systems could be a valuable and engaging tool in rehabilitation regarding functionality in daily activities in people with DMD. 36 A comparative study investigated the performance of computer tasks in people with DMD and compared their performance with that of age-matched typically developing controls, as well as exploring associations between motor function and performance. The results highlighted that participants with DMD improved their performance on repeated trials, with movement times remaining significantly longer than those of typically developing participants. Importantly, DMD participants showed a reduction in movement time from the initial to the transfer phase, thus indicating that learning and adaptation had taken place. The initial performance of the task in DMD individuals was positively correlated with their distal motor function but not with age or overall motor function. This study highlights how computational tasks may enable motor learning and point to future areas of gamification for rehabilitation approaches in DMD patients. 39 Barragan and colleagues further studied the impact of VR-based telerehabilitation on the 6-min walk test and other motor scales in children with Duchenne and Becker muscular dystrophy. The results indeed showed a significant increase in the 6-min walk test of 19.55 meters after 10 telerehabilitation sessions, while other motor function scores remained stable. While these virtual sessions were designed to be fun and engaging, they tended to reduce the perception of fatigue over time, demonstrating that the gamification aspect of such telerehabilitation program was successful in maintaining functional capacity. 41 Additionally, Quadrado et al. examined whether skills learned in the virtual environment could be transferred to a real-world task by individuals with DMD. 40 The results of the performance and outcome measures of the temporal coincidence task – in one task using a real button press and in another with a virtual hand movement – suggest that practice in the virtual environment improved real-world performance in individuals with DMD. This means that skills learned in virtual environments transfer to real-life task performance and task complexity, which can be manipulated to optimise learning and adaptation. Thus, VR-based rehabilitation may have immediate benefits and optimise functional outcomes in patients with DMD. 40 A final study investigated the effectiveness of a VR breathing and relaxation exergame targeting respiratory muscle exercises and mindfulness training in individuals with DMD. The exergame was developed to integrate real-time physiological feedback and telehealth functionalities, allowing remote interaction between patients and clinicians. Thirteen participants demonstrated improvements assessed by the system in terms of relaxation and respiratory control. Gamification of the intervention increased engagement with the exercises and provided a more enjoyable experience. Feedback from participants, family members, and clinicians indicated that it was feasible for use in the home environment and within telehealth applications, increasing the potential to improve care access and quality of life in individuals with DMD. 47 These results emphasize the possibility of using VR interventions to improve rehabilitation results, ensuring that motivation is maintained and enhancing motor learning skills for dealing with NMDs, thus improving overall quality of life.
Discussion
This systematic review highlights new approaches, such as combined VR, biofeedback, and gamification, a new direction in rehabilitation treatment. 49
The studies in this review demonstrate the greater capabilities of VR, biofeedback, and robotics in improving motor functions, motivation, and psychosocial well-being in patients with NMDs, including Duchenne and Becker muscular dystrophies.35–37 The VR training in combination with biofeedback remarkably enhances muscle strength, functional performance, and balance, keeping children motivated throughout the rehabilitation course. Features like interactive storytelling and real-time feedback further enhance the gamification, engagement, and consistency of the exercises. Gains in motor learning and increased cognitive function might indicate that these technologies can be applied to delay functional deterioration and improve the general quality of life in such patients.39–47 The reported findings describe several advances in the use of VR, robotics, and gamification in neuromuscular rehabilitation, extending the existing literature in several key ways. In addition, these findings highlight broader psychosocial and cognitive benefits, confirming the potential of VR and gamification to enhance motor function and engagement.50,51 In addition, when combined with gamification, robotics can promote social inclusion and adaptability for young people with NMD who would otherwise be excluded from social and recreational activities. For example, the findings of Oldford et al. alone show how robotics can become a rehabilitation tool that tends to increase self-esteem, competence and psychosocial well-being, but the integration of robotics with VR and gamified elements may improve rehabilitation outcomes.
52
Furthermore, the development of modular exergames, such as “Blexer-med”, which proposes personalised physical exercises through gamification elements, may offer new perspectives for adaptive rehabilitation.
53
The inconsistency in patient satisfaction, especially in the most fragile patients, underlines the importance of tailoring rehabilitation tools to patients’ needs. This personalization, alongside gamification, is mandatory to sustain motivation, even though, to date, it is rarely applied in an adaptive format.
54
Studies on ALS and DM1 patients provide new insights into how VR rehabilitation may affect autonomic functions and executive performance.
55
The ALS study, measuring HRV during VR tasks performance, shows how VR may influence autonomic responses.
56
If confirmed on a larger number of cases, this may have major implications in ALS rehabilitation. Similarly, the fact that a VR test, such as “Nesplora Ice Cream”, has been applied to patients with DM1 opens new discussions on emotional and cognitive rehabilitation integration, considering the impairments in executive function in this population.
57
The results of DMD are also highly valuable. Treatment with dynamic arm supports and VR aimed at preserving the function of the upper extremities is a promising approach for functional deterioration.
58
In addition, the Leap Motion interface studies confirm that VR is not only entertaining for patients, but can also be designed to improve some fine motor skills, such as distal adaptation.21,59 However, the review also points out some limitations, such as the small sample size of many of the studies analysed, which may reduce the generalisability of the results, and the fact that the methods and technologies discussed are clearly at an early stage of development, suggesting the need for further refinement before wider application.
However, the review also points out some limitations, such as the small sample size of many of the studies analysed, which may reduce the generalisability of the results, and the fact that the methods and technologies discussed are clearly at an early stage of development, suggesting the need for further refinement before wider application. Another limitation is the lack of long-term outcomes about the effectiveness of VR and gamification in terms of functional improvement and motivation
The focus on the
Conclusions and future directions
This systematic review
Footnotes
Acknowledgments
None.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Current Research Funds 2024, Ministry of Health, Italy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplementary material.