
Abstract
Background
Breastfeeding-related musculoskeletal disorders (BRMSDs) are prevalent among nursing mothers. Knowledge of suitable breastfeeding positions and their adverse health outcomes is necessary for the prevention of BRMSDs. However, research is lacking that has examined this in the southeast Nigerian population.
Objectives
To assess the knowledge of BRMSDs and suitable breastfeeding positions among pregnant women in the Enugu metropolis.
Methods
A descriptive cross-sectional survey was conducted on 100 pregnant women (mean age of 27.2 ± 5.0 years) who completed a researcher-structured questionnaire on the knowledge of BRMSDs and general characteristics of the participants. Data were analysed using descriptive and inferential statistics of Chi-square at p < 0.05.
Results
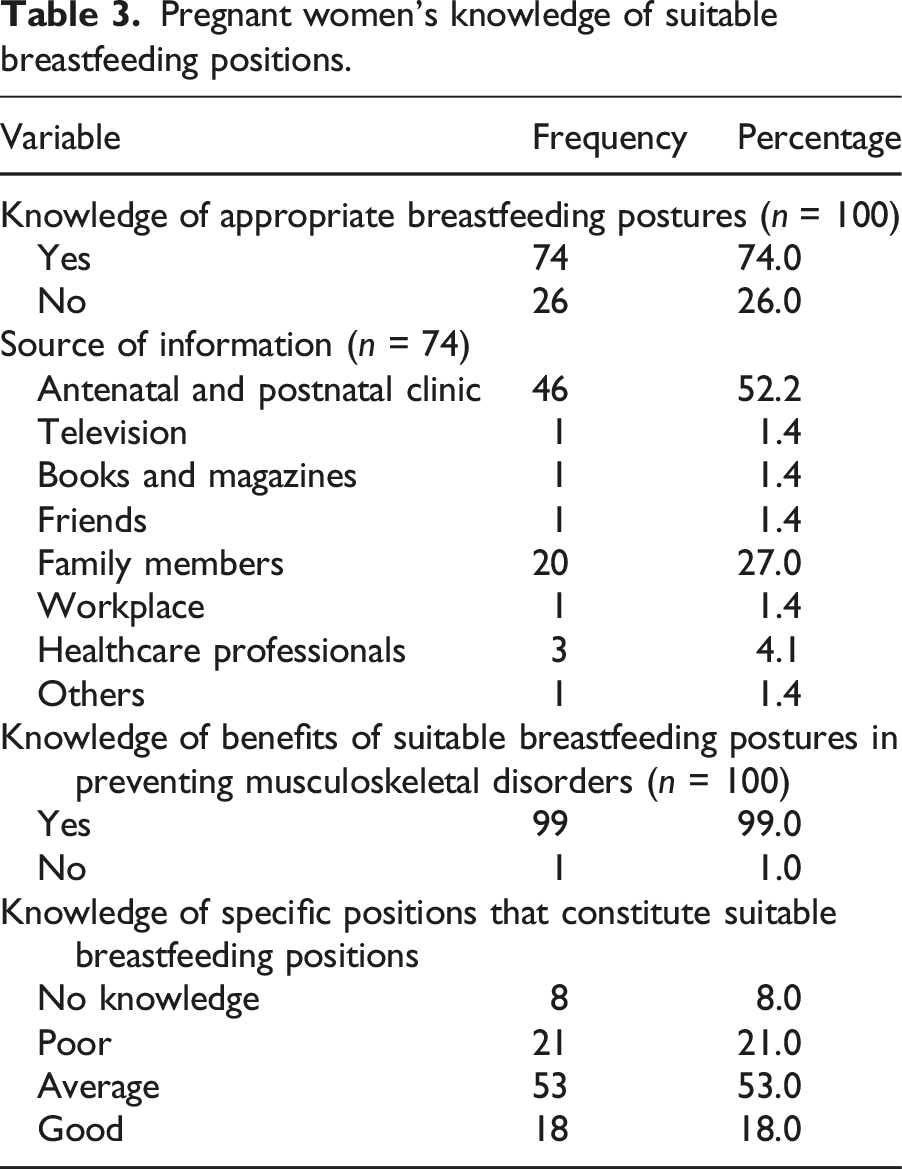
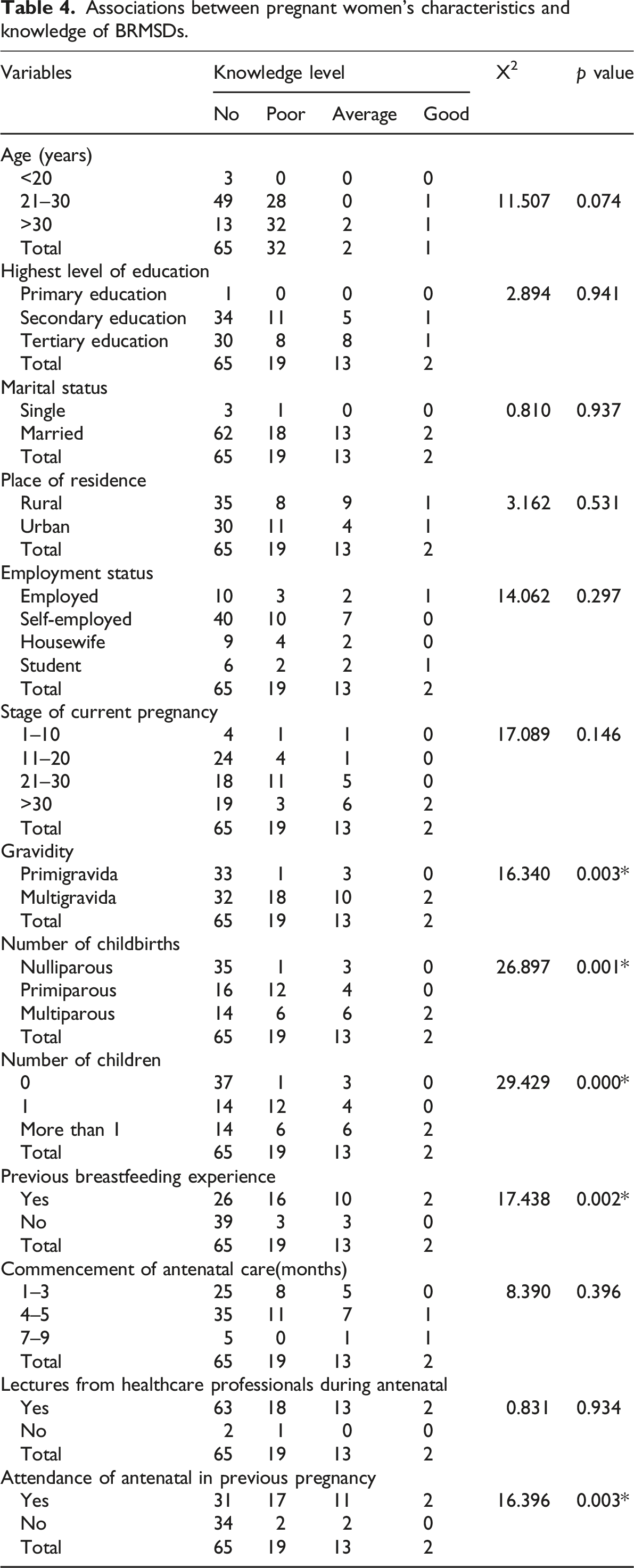
Slightly over half (55.0%) of the respondents lacked awareness of BRMSDs. Out of the 45% of them who were aware of BRMSDs, the majority gained the knowledge from antenatal and postnatal clinics (62.2%) and identified the upper/lower back (82.2%) and neck (62.2%) as the most affected body parts while breastfeeding for long hours per session was identified as the most common cause of BRMSDs (57.7%). The majority (53.0%) of the respondents have average knowledge of suitable breastfeeding positions. Furthermore, primigravida, a lesser number of previous childbirths, a lesser number of previous children, no previous breastfeeding experience, and non-attendance of antenatal classes in previous pregnancy(ies) were significantly (p < 0.05) associated with pregnant women’s knowledge of BRMSDs.
Conclusion
Knowledge of BRMSDs and suitable breastfeeding positions is fair among pregnant women. Maternal education to address these gaps is recommended.
Statement of significance
• Breastfeeding-related musculoskeletal disorders (BRMSDs) are prevalent among nursing mothers. • Knowledge of suitable breastfeeding positions and their adverse health outcomes is necessary for the prevention of BRMSDs. Still, the level of knowledge on this is not reported in research among women in developing countries. • We found a fair level of knowledge among pregnant women in Nigeria, necessitating more targeted maternal education on this subject during antenatal classes.
Introduction
Breastmilk has been regarded as the best form of nutrition for infants and also the gold standard for newborn nutrition. 1 The WHO and UNICEF 1 recommend that children initiate breastfeeding within the first hour of birth and be exclusively breastfed for the first 6 months of life, and up to 2 years of age or beyond in conjunction with other food. It is important not only for achieving the global goals of nutrition, health, and survival but also in terms of economic growth and environmental sustainability and should thus be considered a national and international health priority. 2 However, several factors, ranging from maternal, infant, environmental, socio-economic, and medical, among others, have been identified as barriers to exclusive breastfeeding in Nigeria.3–5 Relative to the mother, breastfeeding is physically demanding and poses remarkable energy costs, risk of faulty posture, and physical stress,6–8 leading to sudden severe stress9,10 and resultant Musculoskeletal Disorders (MSDs). 11 Specifically, breastfeeding has been commonly associated with the adoption of awkward body positions, shear postures, and poor latching techniques during feeding sessions.12–14
In Nigeria, nursing mothers have reported BRMSDs across various body segments (back, neck, and upper limb joints), with the neck and shoulder identified as the most affected body regions.12,15,16 Anecdotally, we have observed that these BRMSDs mitigate compliance with exclusive breastfeeding practices. Inappropriate techniques of breastfeeding and improper feeding due to these MSDs, among other problems such as nipple soreness, result in the failure of lactation. 14 For successful and effective breastfeeding, suitable breastfeeding mechanics, including latching and positioning, are considered important,17,18 as well as the use of breastfeeding pillows where necessary. 19 Maternal education for increasing awareness levels of BRMSDs, appropriate breastfeeding positions and postures becomes a vital tool for breastfeeding promotion, as poor knowledge levels among pregnant women have been identified as associated factors of BRMSDs.13,20 Tella et al. 21 reported that pregnant women in Karnataka, India, who had poor knowledge and attitudes of appropriate breastfeeding positions were more likely to experience poor breastfeeding practices, due to discomfort leading to unsuccessful lactation.
A few Nigerian studies have explored the knowledge of appropriate breastfeeding positions among pregnant and postpartum mothers. Mbada et al. 22 reported that nursing mothers in southwestern Nigeria demonstrated good knowledge and positive attitudes towards breastfeeding, with most practising advisable postures and effective techniques. Conversely, in another study, 13 nursing mothers in Enugu, southeast Nigeria showed poor practice and knowledge of appropriate breastfeeding positions, with a recommendation of maternal education to enhance positive practices. In response, healthcare personnel within the Enugu metropolis had previously shown some compliance with this recommendation. However, there have not been follow-up research activities to assess current knowledge levels of BRMSDs among mothers. Therefore, in this study, we investigated the knowledge of suitable breastfeeding positions and additionally, BRMSDs among pregnant women in Enugu, southeast Nigeria.
Methods
Study participants
A descriptive cross-sectional survey was conducted among 100 pregnant women who were conveniently recruited from the prenatal classes of two selected healthcare facilities in Enugu metropolis, southeastern Nigeria. A preliminary power analysis supported the sample of 100 participants for the Chi-square analysis at a degree of freedom (dfb) = 1, to achieve 99% (0.99) power with a small to moderate effect size of 0.40 at an alpha level of 0.05. 23 The data collection inclusion criteria were pregnant women who could read, write, and understand English to aid self-reporting and response to the data collection tool. Women who are medical personnel were excluded from this study because their professional or occupational dispositions may have exposed them to the requisite knowledge of BRMSDs. Ethical approval for the study was obtained from the health research ethics committee of the University of Nigeria Teaching Hospital, Ituku Ozalla Enugu state, Nigeria, and the research followed the ethical principles recommended by Helsinki.
Study instrument
A researcher-structured questionnaire on the knowledge of BRMSDs and general characteristics of pregnant women was developed in the English Language. The five-section tool had mostly closed-ended questions. In section (A), sociodemographic data were elicited, including age, educational level, marital status, employment, and living in a rural or urban location. Additionally, maternal characteristics were collected in this section, including gestation period, gravidity, number of previous childbirths, number of children, previous experience with breastfeeding baby(ies), months of commencement of antenatal care, and whether they received lectures from healthcare professionals during antenatal classes. Section (B) elicited data on knowledge of BRMSDs, which included awareness of BRMSDs, sources of knowledge of BRMSDs, possible body areas that could sustain BRMSDs, and causes of BRMSDs. The third section (C) elicited data on knowledge of suitable breastfeeding positions, which included appropriate breastfeeding postures and positions, as well as sources of information about breastfeeding postures.
The content and face validity of the questionnaire were reviewed by four experts (two clinical and two academic women’s health physiotherapists) who advised on how to increase its accessibility and confirmed the final draft. The questionnaire was also subjected to test-retest reliability by piloting it among 10 different samples of pregnant women. The intra-class correlation analysis for internal consistency, conducted at a 95% confidence interval, resulted in a correlation coefficient of r = 0.787 (p = 0.001), indicating a high level of reliability. 24
Data collection
The data collection took place between February and May 2023 in different contacts of groups of pregnant women during their antenatal classes. Participants were initially identified and addressed collectively during their antenatal classes in the outpatient maternity clinics of the selected hospitals. The nature, objectives, and relevance of the study were explained to them. Those who were willing to participate and who met the eligibility criteria were given the self-administered questionnaire after they had signed written informed consent. The questionnaires were duly filled out, and clarifications were given where necessary. Filled copies were collected immediately, which helped to ensure a 100% response rate.
Data analysis
Knowledge of BRMSDs was recorded as a “yes, maybe, or no” and scored 2, 1, or 0, respectively. The total score by individual participants was expressed as a percentage of the total possible level of knowledge score and coded as no knowledge (0%), poor knowledge (<60%), average knowledge (60%–79%), and good knowledge (80%–100%).
Data was summarised using descriptive statistics of frequency and percentages. Inferential statistics of Chi-square were used to assess the association between BRMSD knowledge levels and the demographic and maternal characteristics of pregnant women at p < 0.05. Data analysis was done with the aid of the Statistical Package for Social Sciences (SPSS, version 25, Chicago, USA).
Results
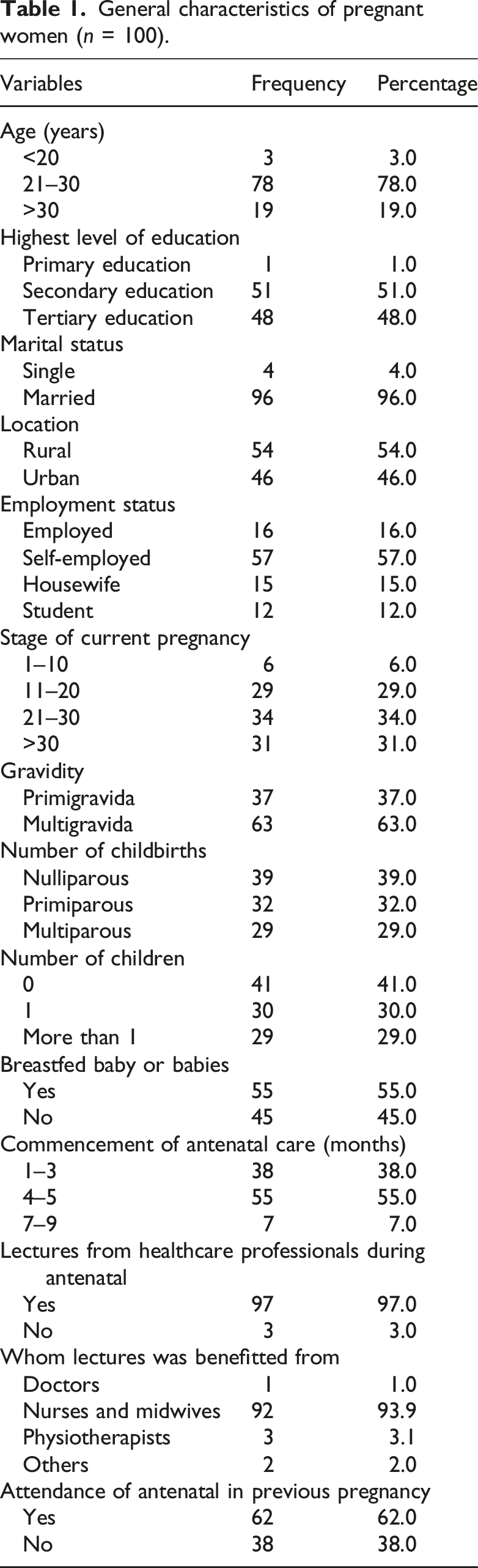
General characteristics of pregnant women (n = 100).
Knowledge of breastfeeding-related musculoskeletal disorders (BRMSDs).
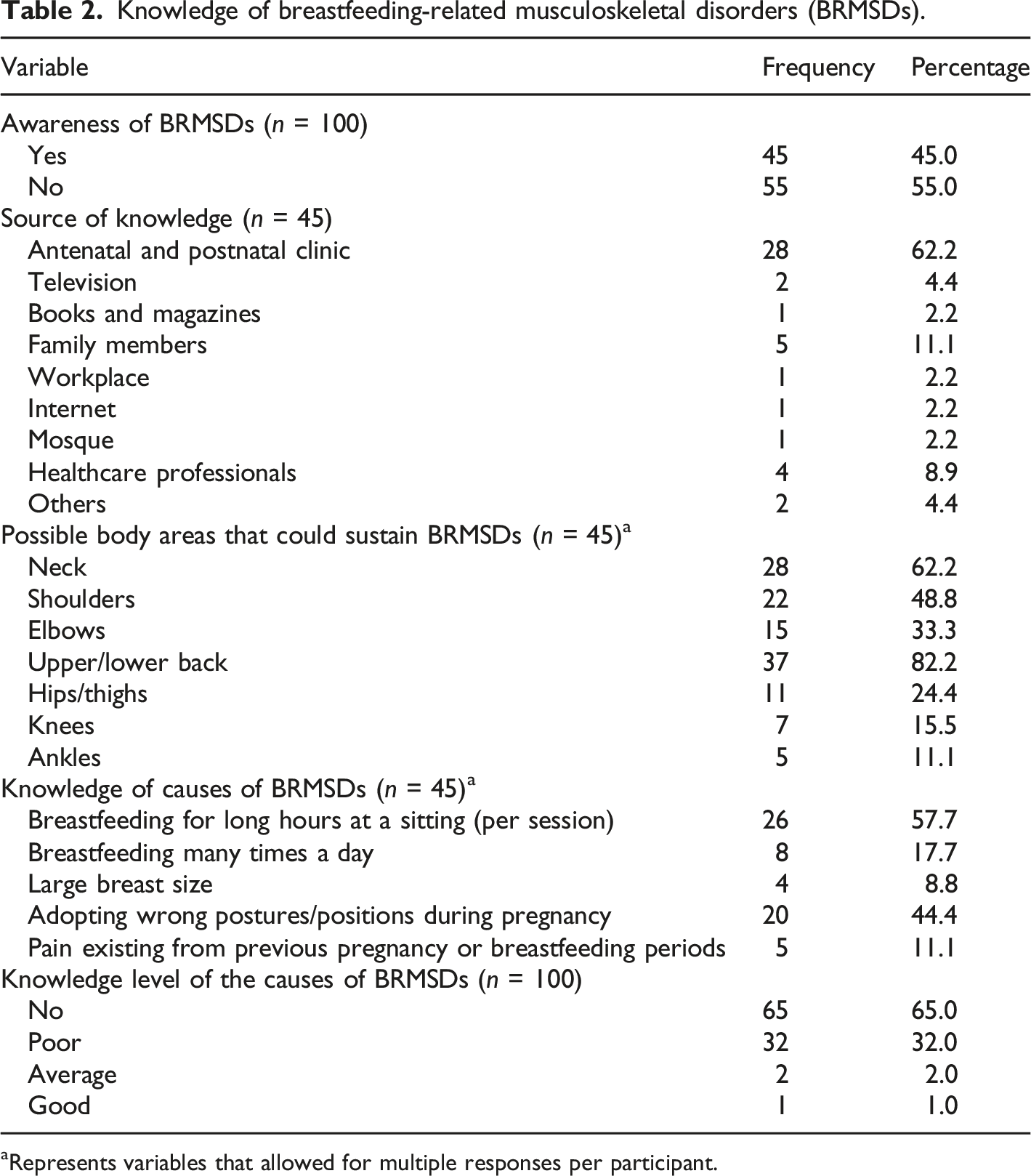
aRepresents variables that allowed for multiple responses per participant.
Pregnant women’s knowledge of suitable breastfeeding positions.
Associations between pregnant women’s characteristics and knowledge of BRMSDs.
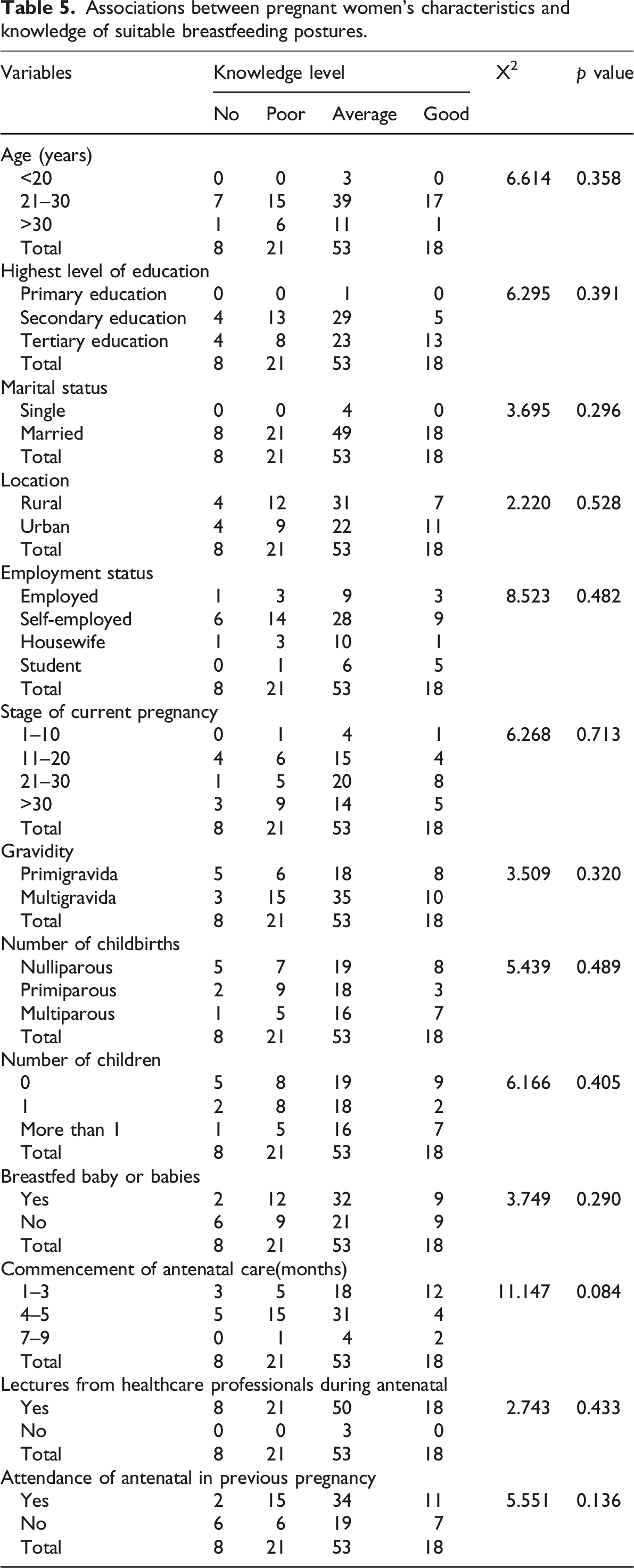
Associations between pregnant women’s characteristics and knowledge of suitable breastfeeding postures.
Discussion
This descriptive cross-sectional survey assessed the knowledge of breastfeeding-related musculoskeletal disorders (BRMSDs) and suitable breastfeeding positions among pregnant women in the Enugu metropolis. A below-average level of knowledge of BRMSDs was noted among pregnant women. The major factors leading to low knowledge were usually primigravida, a lesser number of previous childbirths, a lesser number of previous children, no previous breastfeeding experience, and non-attendance of antenatal classes in previous pregnancy(ies).
The low knowledge of BRMSDs and their causes that is noted in this study is consistent with those reported in related literature.12,13,15 Proper posture is a crucial practice that significantly reduces the risk of musculoskeletal disorders.25,26 According to the health belief model, poor knowledge of the crucial nature of proper positioning and appropriate practice of it, as well as its benefits, could mean that breastfeeding mothers will have little reason to adopt it as an important practice. This could explain why survey studies in this population have reported a high prevalence of BRMSDs,12,26 similar to the values recorded in this study.
While awareness about the benefits of breastfeeding has been increasing over the years with the information and education strategies brought about by various organisations and healthcare providers, the knowledge and awareness about BRMSDs and suitable breastfeeding positions remain limited. 20 Mothers often did not receive education about safe or optimal breastfeeding positioning from healthcare practitioners. 26 In the present study, only 28% gained knowledge from antenatal and postnatal clinics about BRMSDs and breastfeeding positioning. This is indicative of the need for an MDT approach to antenatal education to increase the diversity of knowledge shared at this important phase of the soon-to-be mothers. Other common sources of information about BRMSDs and breastfeeding positions included television, family members, and healthcare professionals. Unlike the report on the increasing usage of the Internet by many pregnant women for relevant information about pregnancy, birth, and childcare, 27 there was not much emphasis on the Internet in the present study. This could be due to the very low level of knowledge and campaigns about BRMSDs and breastfeeding positioning practices among healthcare practitioners.
The causes of BRMSDs are noted to be due to breastfeeding for long hours per session, which corresponds with previous works that have reported defective breastfeeding positions in which mothers stoop over their babies for long periods instead of bringing the baby closer to them.14,28 Ojukwu et al. 16 have also reported that unsupported head/neck posture with resultant sustained neck flexion in an attempt to monitor the infant during feeding is one of the most common awkward positions adopted by breastfeeding mothers and such a sustained awkward position with excessive repetition usually puts stress on the neck and back muscles. The pregnant women in this study showed poor knowledge of most of these causes, indicating the magnitude of their knowledge gap and possible lack of preventive practices. This also highlights the need for interventions targeted at promoting awareness, changing the attitude of mothers about the technique of breastfeeding, and enhancing maternal and neonatal health.
Given that promoting improved knowledge and self-efficacy is key to behavioural change and knowledge uptake,29,30 the uptake of healthy behaviour and behaviour change regarding breastfeeding positions and BRMSDs can be promoted with interventions targeted at the identified moderating factors in this study. In agreement with the work of Mbada et al., 22 many pregnant women agreed that adopting suitable breastfeeding positions is beneficial to the mother. However, despite these limitations, the present study’s finding reveals that knowledge of BRMSDs is significantly lower among certain subgroups, particularly primigravida women, those with fewer previous childbirths, those who have never breastfed, and those without antenatal attendance in their previous pregnancy. This suggests that firsthand experience, experience-based learning, and structured prenatal education play a crucial role in shaping awareness and understanding of BRMSDs.31,32 Antenatal programs should therefore incorporate specific modules on BRMSDs, emphasising preventive strategies and proper positioning techniques to reduce discomfort and long-term musculoskeletal complications postpartum. Also, primigravida women may require deliberate educational reinforcement to bridge this gap. Healthcare providers should consider employing interactive, multi-disciplinary, and demonstrative teaching methods, including visual aids and hands-on training, to enhance retention and practical application of breastfeeding ergonomics.
In addition to structured antenatal education, community-based interventions, peer support groups, and digital health resources can play a complementary role in disseminating information on BRMSDs and proper breastfeeding postures. Social media platforms, mobile applications, and telehealth services can serve as accessible tools for continuous engagement and reinforcement of best practices, particularly for women who may have limited access to in-person healthcare services. This study finding is therefore essential for reducing the burden of BRMSDs and promoting maternal and foetal health. Future research should explore the effectiveness of various educational strategies in improving knowledge uptake and behavioural changes among pregnant and breastfeeding women.
Study limitation
This study relied on self-reported data from pregnant women already attending antenatal care, which may limit the generalisability of the findings. Women who do not attend antenatal clinics or seek alternative healthcare services were not included, and their knowledge and experiences regarding BRMSDs and breastfeeding positions may differ. Future studies should consider broader recruitment strategies, including community-based surveys, to capture more diverse populations. Additionally, the cross-sectional design of this study limits the ability to establish causal relationships between knowledge levels and identified moderating factors. A longitudinal or interventional study design would provide more insight into how knowledge evolves over time and how targeted educational interventions may influence behavioural change. Another limitation is the reliance on self-reported data, which introduces the potential for response bias, particularly social desirability bias. Since data collection took place within a hospital setting, participants may have provided responses they believed were expected rather than their actual knowledge or practices. Future research should consider incorporating objective assessments, observational methods, or validated knowledge tests to enhance data reliability. Despite these limitations, the findings provide valuable insights into knowledge gaps and the need for targeted educational interventions to improve breastfeeding ergonomics and reduce the risk of BRMSDs among pregnant women.
Conclusion
Pregnant women’s knowledge of BRMSDs and suitable breastfeeding positions is below average. Maternal education to address these gaps is recommended to increase awareness and good knowledge of the importance of proper positioning and the actual and proper practices. As well as to change mothers’ attitudes towards breastfeeding techniques and encourage them to adopt the correct breastfeeding practices, which will enhance maternal and neonatal health, prevent complications, and improve their independence and quality of life.
Footnotes
Ethical considerations
Ethical approval for the study was obtained from the health research ethics committee of the University of Nigeria Teaching Hospital, Ituku Ozalla Enugu state, Nigeria (NHREC/05/01/2008B-FWA00002458-1RB00002323), and the research followed the ethical principles recommended by Helsinki.
Consent to participate
The procedure, ethical obligations, and the purpose of the research were clearly explained to participants who gave their written informed consent before the study commenced.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.