
Abstract
Background:
Antenatal exercise is crucial in promoting pregnant women’s health and well-being. However, no research in Libya examined the knowledge, attitudes, and practices of antenatal exercise among pregnant women.
Methods:
This cross-sectional study aimed to explore the knowledge, attitudes, and practices related to antenatal exercise among pregnant women in Libya. A convenience sample of pregnant women (n = 205) receiving prenatal care at Misrata Medical Center and having no contraindication for exercise participated in the study. A self-administered, previously elaborated questionnaire was used to assess participants’ awareness, knowledge, attitudes, and practice of antenatal exercise. Descriptive statistics and binary logistic regression analysis were employed using SPSS version 28.
Results:
The findings revealed that nearly half of the participants demonstrated good knowledge (56.1%) and a positive attitude (47.8%) regarding antenatal exercise. Less than one-third (30.2%) of participants engaged in some form of exercise during pregnancy. The logistic regression results showed that age, income, and practice of exercise before pregnancy significantly contributed to the knowledge score. The analysis indicated that the unemployment status (AOR = 2.42, 95% CI [0.78-6.38], P = .03) and practicing exercise before pregnancy (AOR = 1.97, 95% CI [0.92-4.24], P = .02) were significantly associated with a higher likelihood of engaging in antenatal exercise. The main subjective reasons for pregnant women not engaging in antenatal exercise were lack of time, poor knowledge, fatigue, and worries about harming the baby.
Conclusion:
This study sheds light on the current state of antenatal exercise among pregnant women in Libya and highlights the factors shaping these behaviors. The findings underscore the importance of promoting accurate knowledge, addressing misconceptions, and providing support and resources to overcome barriers and encourage safe and effective antenatal exercise practices in Libya. Future studies should consider employing qualitative or mixed methods research designs to examine antenatal exercise from different perspectives.
Introduction
Antenatal exercise, which refers to exercise that women perform during pregnancy, is an essential aspect of prenatal care that helps promote the health of both the mother and baby. 1 For the mother, regular exercise during pregnancy can help to reduce the risk of gestational diabetes, high blood pressure, and preeclampsia. 2 Antenatal exercise can also help to improve mood and reduce the risk of postpartum depression. 3 For the baby, antenatal exercise can help to improve fetal growth and development, reduce the risk of preterm birth, and improve overall health outcomes. 4 Moreover, regular pregnancy exercise can help improve the baby’s brain development and cognitive functions. 5
International organizations and healthcare authorities widely endorse antenatal exercise as a beneficial practice for healthy pregnant women. The World Health Organization (WHO) 6 recognizes that regular, moderate-intensity physical activity during pregnancy can reduce pregnancy-related complications and improve maternal psychological well-being. Similarly, the National Institute for Health and Care Excellence (NICE) 7 guidelines emphasize the benefits of antenatal exercise in promoting maternal physical fitness, reducing the risk of back pain, and aiding in the management of gestational hypertension. Additionally, the American College of Obstetricians and Gynecologists (ACOG) 8 highlights that appropriately prescribed antenatal exercise can enhance maternal cardiovascular fitness, musculoskeletal health, and overall quality of life during pregnancy. These authoritative endorsements underscore the positive impact of antenatal exercise on maternal health, reinforcing its importance as a safe and effective practice for pregnant women.
Decreased physical activity during pregnancy represents a significant public health concern, as it is recognized as the fourth leading risk factor contributing to maternal mortality worldwide. 9 A sedentary lifestyle during pregnancy can lead to a range of adverse health outcomes for pregnant women, including an increased risk of excessive weight gain, gestational diabetes, hypertensive disorders, and venous thromboembolism. 10 These complications not only compromise the health and well-being of pregnant women but can also have long-term consequences for maternal and fetal health. 11 Therefore, promoting and encouraging appropriate levels of physical activity during pregnancy is imperative to mitigate these risks, improve overall maternal health, and reduce the burden of maternal mortality.
Despite the numerous benefits of antenatal exercise, many expectant mothers are unaware of its importance. A study conducted among pregnant women in Saudi Arabia found that 58.4% had a low level of awareness about the benefits of antenatal exercise. 12 Moreover, the Saudi study reported that 84.2% of women were not practicing any exercise during pregnancy. Similarly, a study in Ethiopia reported nearly two-thirds (60.5%) of pregnant women had a low level of knowledge about antenatal exercise and only 30.9% of participants practiced exercise during pregnancy. 13 Lack of awareness and knowledge about the benefits and safety of antenatal exercise can lead to a lack of motivation and reluctance to engage in exercise during pregnancy. 14 Therefore, it is crucial to educate expectant mothers about the importance of antenatal exercise and how to carry it out safely.
Attitude toward antenatal exercise is another critical factor influencing women’s engagement in exercise during pregnancy. One study in Sweden compared physical activity patterns among women pre-pregnancy, during pregnancy, and 8 months postpartum found a significant decline in nearly all activities studied. 15 This study explained the decline in physical activity during pregnancy due to fatigue, lack of motivation, and other environmental factors such as access to exercise settings. 15 In developing countries, women may have negative attitudes toward exercise during pregnancy due to other factors such as cultural beliefs or fear of harming the baby.16,17 However, research has shown that exercise during pregnancy is generally safe and beneficial for both the mother and baby. 18 Therefore, it is essential to encourage a positive attitude toward antenatal exercise and debunk any myths or misconceptions that may deter expectant mothers from engaging in exercise.
Although antenatal exercise is highly recommended during pregnancy due to its several benefits, many expectant mothers do not exercise regularly. A study conducted among pregnant women in Brazil found that only 20% of women engaged in regular exercise during pregnancy. 19 Another study in Saudi Arabia reported that only 15.8% of the studied sample practiced antenatal exercise. 12 Reasons for this poor engagement in antenatal exercise vary. However, several studies consistently reported that lack of time, motivation, and support can be significant barriers to the practice of antenatal exercise.13,15,19
Understanding the level of awareness, attitudes, and practices surrounding antenatal exercise in Libya is essential for developing targeted interventions, educational programs, and healthcare guidelines. The context of Libya offers a unique and underexplored landscape for studying antenatal exercise among pregnant women, even in the face of extensive research in western countries. Libya’s distinct cultural, societal, and healthcare factors, such as cultural norms, healthcare infrastructure, and access to resources, create a context that can significantly influence pregnant women’s exercise behaviors and overall maternal health outcomes. 20 Moreover, the country’s geopolitical history and recent healthcare challenges introduce specific health disparities and barriers that may necessitate tailored interventions for pregnant women.21,22 Although maternal mortality rates have declined over the past few decades, 23 the progression of this decline is slow and requires more attention. 24 Today, Libya has a much higher maternal mortality rate compared to other Arab countries. 25 Several health complications, including potentially life-threatening to the mother and/or the baby, have been reported in previous studies in Libya, highlighting the need for a more active lifestyle and innovative care options for pregnant women. 26 Therefore, it is a national priority to provide culturally relevant insights that inform healthcare policies and practices tailored to the unique needs of this population.
Equally important, conducting studies in this area potentially identifies knowledge gaps, addresses misconceptions, promotes safe and effective exercise practices, and ultimately contributes to improved maternal health outcomes in this country. Additionally, such studies can provide valuable insights for healthcare providers to better support and guide pregnant women in incorporating appropriate exercise into their antenatal care. The initial and crucial step in promoting antenatal exercise involves comprehensively exploring women’s awareness, knowledge, and attitudes toward such interventions. Therefore, this study aims to examine awareness, knowledge, attitudes, and practice of antenatal exercise among a sample of pregnant women in Libya.
Methods
Study design and setting
A descriptive cross-sectional study was conducted in Misrata City, Libya, from January 15th to May 15th, 2022. Misrata city has a population of nearly 500 000 inhabitants and is located 200 km east of the Libyan capital, Tripoli. The data was collected in the Obstetrics and Gynecology outpatient clinic at Misrata Medical Center (MMC). The MMC is the central healthcare institution in the city that provides medical services to the public for no cost. The MMC serves about 1 million people who live in the Misrata area and neighboring towns and cities in the middle region of Libya.
Anonymous questionnaires were distributed to pregnant women attending antenatal clinics in MMC and those attending other healthcare units in the same facility. Included participants were those 18 years of age or older and in stable medical condition. Women with unstable medical conditions or emotional or psychological problems were instructed not to complete the study questionnaires to comply with institutional policy and ethical standards. The recruitment of participants and collection of completed questionnaires were performed with the help of the nursing staff at data collection sites who were not part of the research team. The study package, including the questionnaire, was made available for a period of 4 months, and participants were given the option to complete the questionnaire at their convenience.
Ethical considerations
The Institutional Review Board (IRB) approved the study at the researcher’s institution [Ref# Ext-611-2022]. Informed consent was obtained from all participants before they were allowed to access the survey. The participants were informed about the purpose of the study, and their confidentiality was ensured throughout the study. To the best of our knowledge, this study was conducted following the Declaration of Helsinki. 27
Sample size calculation
The sample size was calculated using EpiInfo™ software, version 7. Since there are no studies that have investigated this topic in Libya, we hypothesized the probability of the knowledge about antenatal exercise in Libya to be 50%; the statistical power is 90%, a precision of ±5%, a design effect of 1.0, and a non-response of 10%, the minimum required sample size was estimated to be 182 participants.
Data collection tools
This study adopted the questionnaire used by previous studies conducted in Ethiopia, 13 Nigeria, 28 and Brazil. 19 The original English questionnaire was translated into Arabic and modified to meet the purpose and context of this study. We used the forward-backward translation method suggested by Beaton et al 29 to translate and culturally validate the questionnaire into the Arabic context. After rounds of discussion with the research team, the translated questionnaire was approved and tested on 27 pregnant women to evaluate its reliability, the questions’ clarity, and the time required to complete the questionnaire. Data collected during this phase were not included in the data analysis. Based on the pilot testing, the questions were determined to be straightforward and easy to understand. The reliability of the questionnaire, as measured by Cronbach’s α, was excellent (α = .89).
The final version of the questionnaire consisted of 48 questions. The questionnaires were designed to gather information on the variables of interest, including antenatal exercise awareness, knowledge, attitudes, and practices among pregnant women in Libya. The questionnaire consisted of closed-ended questions and Likert scale items. It encompassed sections on socio-demographic characteristics, such as age, educational level, occupation, maternal information, and medical characteristics, to provide a comprehensive understanding of the study population.
The questionnaire also included a section dedicated to assessing awareness about antenatal exercise. In the context of this study, “awareness of antenatal exercise” refers to the level of knowledge pregnant women possess regarding the concept, benefits, and safety considerations associated with engaging in physical activity during pregnancy. This encompasses understanding the potential positive effects of exercise on maternal and fetal health, recognizing the recommended types and intensity of exercises, and being aware of possible contraindications or precautions. This section assessed women’s awareness by evaluating their familiarity with different types of exercises. Participants were presented with the question, “Are you familiar with these antenatal exercises?” followed by a list of various exercises commonly recommended during pregnancy. The list included examples such as walking, breathing, yoga, low-impact aerobics, pelvic floor exercises, and stretching exercises. Participants were instructed to indicate their level of awareness for each exercise by selecting one of the following options: “yes,” “no,” or “don’t know.” This question allowed researchers to gauge the participants’ awareness and familiarity with specific antenatal exercise options. The total awareness score is the sum of the 9 items, and those who achieved more than the mean score were considered to have a good awareness of antenatal exercise. The questionnaire aimed to provide insights into the level of awareness regarding different types of antenatal exercises among pregnant women, highlighting areas that may require further education or promotion.
The third section of the questionnaire aimed to assess the knowledge of pregnant women regarding antenatal exercise. In this study, “knowledge regarding antenatal exercise” refers to the factual understanding and comprehension of pregnant women about the various aspects of safe and beneficial physical activities during pregnancy. It encompasses familiarity with the principles, benefits, and possible risks associated with exercise during the antenatal period. This section consisted of 22 questions, each requiring a response chosen from 3 options: “yes,” “no,” or “don’t know.” The questions covered various aspects of antenatal exercise, including its benefits and potential risks. The “yes” answer was scored “1,” and the “No” or “I don’t know” responses were scored “0.” The total score is the sum of the 22 values ranging from 0 to 22. We considered that a participant had good knowledge if their score exceeded the mean value.
Additionally, the questionnaire assessed the attitudes of pregnant women toward antenatal exercise. In the context of this study, “attitude toward antenatal exercise” refers to the overall evaluation, emotional disposition, behavioral inclination, and perceived barriers that pregnant women hold toward engaging in physical activities during pregnancy. It encompasses their feelings, beliefs, opinions, and motivations related to participating in exercise during the antenatal period. This section consisted of 12 questions, with respondents selecting their answers from 3 options: “yes,” “no,” or “don’t know.” The questions explored various aspects of attitudes related to antenatal exercise, including motivation, perceived benefits, and perceived barriers. Participants were asked about their level of interest and willingness to engage in physical activity during pregnancy. The questionnaire also investigated their beliefs about the impact of exercise on their own health and the health of their baby.
Additionally, it examined potential barriers that may prevent pregnant women from participating in antenatal exercise, such as lack of time, concerns about safety, or discomfort during pregnancy. The answers were scored as “1” for “yes” and “0” for “no” or “don’t know”. The total score is the sum of the 12 items, and those who achieved more than the mean score were considered to have a positive attitude toward antenatal exercise.
To capture information about the actual practice of antenatal exercise, a section in the questionnaire was dedicated to collecting data on the types of exercises performed, frequency, and duration. Of women who reported practicing antenatal exercise at least 3 times a week for a minimum of 20 minutes per session, as recommended by the ACOG, 8 were considered to have adequate practice.
Data analysis
The collected data was analyzed using a combination of descriptive statistics and logistic regression analysis to address the research objectives of this study. Descriptive statistics were employed to summarize and describe the socio-demographic characteristics of the study population, including age, educational level, occupation, and other parental and medical variables. Frequencies and percentages were calculated for categorical variables, while mean and standard deviation were computed for continuous variables.
Furthermore, a binary logistic regression analysis was performed to investigate the predictors of antenatal exercise. This analysis allowed for examining the influence of various independent variables (eg, knowledge, attitudes, and socio-demographic factors) on the likelihood of engaging in antenatal exercise. Predictor variables found to be significantly associated with the outcome variable in the univariate analysis were included as independent variables in the logistic regression model. Adjusted odds ratios (AORs) and their corresponding 95% confidence intervals (CIs) were calculated to estimate the strength and direction of the associations while controlling for potential confounders. All statistical analyses were performed using a statistical software package, SPSS (version 28), and the significance level was set at P < .05. The goodness-of-fit of the logistic regression model was assessed using the Hosmer-Lemeshow test. This method is widely used to evaluate the goodness-of-fit of logistic regression models by comparing the observed and expected frequencies of outcomes across different predicted probability groups. 30 However, there is no universally accepted threshold for what constitutes “acceptable” model fit values using the Hosmer-Lemeshow test. Instead, interpretation is often context-dependent, and the results are evaluated by examining the chi-square statistic and its associated p-value. Generally, a large value of Chi-squared (with a small P < .05) indicates poor fit and small Chi-squared values (with a larger P-value closer to 1) indicate a good logistic regression model fit. 31 Model assumptions, including linearity, multicollinearity, and independence of observations, were carefully checked and addressed.
Results
Participant characteristics
A total of 300 pregnant women were invited to participate in the study; 205 returned the completed questionnaires (response rate = 68.3%). The mean age of the participants was 27.56 years (SD = 7.18), ranging from 18 to 50 years. Most women (69.3%) were young (ie, less than 30 years old). The educational background of the participants varied. It was observed that 75.6% had completed college or university education, 5.9% had a graduate degree, and 2.9% had no formal education. Regarding employment, the participants were classified into different categories. Nearly two-thirds of participants, 68.8%, were unemployed, while the rest were employed in private or public sectors.
In addition to socio-demographics, the study also collected information on the medical characteristics of the participants. The majority of participants were in their second trimester (46.3%), followed by the third trimester (34.6%) and the first trimester (19.0%). Furthermore, the participant’s Body Mass Index (BMI) was calculated using their self-reported height and pre-pregnancy weight. The BMI values were categorized based on the national and international guidelines into 4 categories: Underweight (BMI < 18.5 kg/m2), normal weight (BMI 18.5-24.99 kg/m2), overweight (BMI = 25-29.99 kg/m2), and obese (BMI ⩾ 30 kg/m2). The distribution of participants across these categories is presented in Table 1. However, the significant finding is that about two-thirds of the study participants were either overweight (45.9%) or obese (21.0%).
Socio-demographic and health characteristics of the study sample (n = 205).
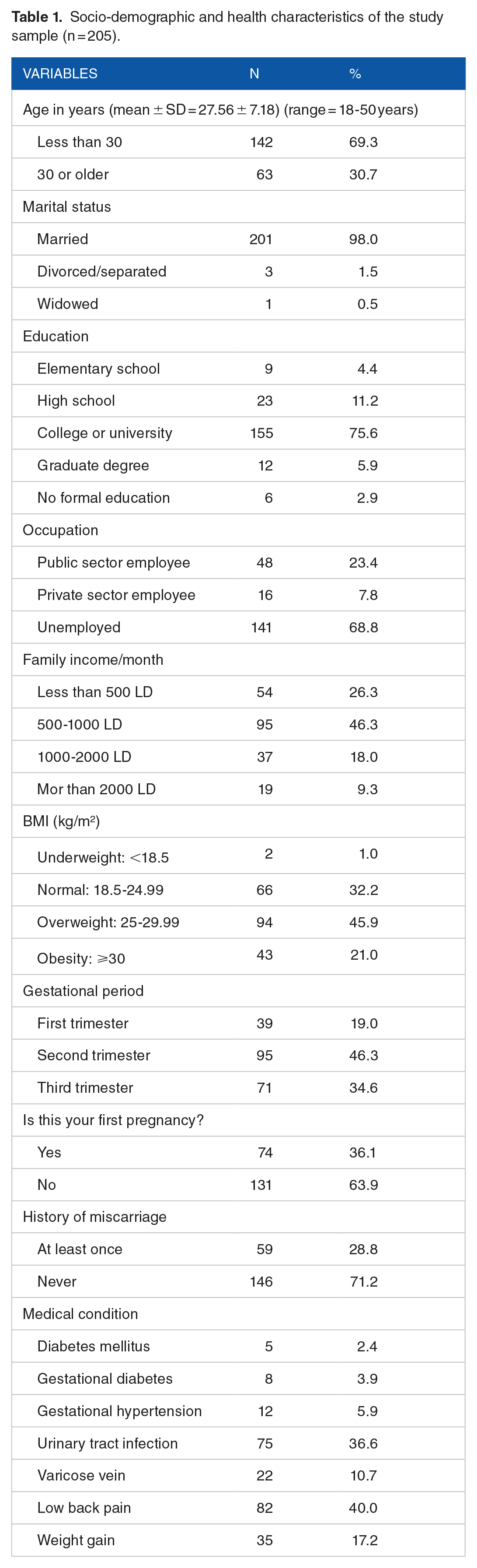
The study also assessed the presence of various medical conditions among the participants. The most common medical conditions reported by the participants included low back pain (40.0%) and urinary tract infection (36.6%). Other reported medical conditions included gestational diabetes, gestational hypertension, and varicose veins, among others. These medical characteristics provide insights into the health status and medical history of the study participants, which may have implications for their exercise practices during pregnancy. The socio-demographic and medical characteristics of the participants are summarized in Table 1.
Awareness of antenatal exercise
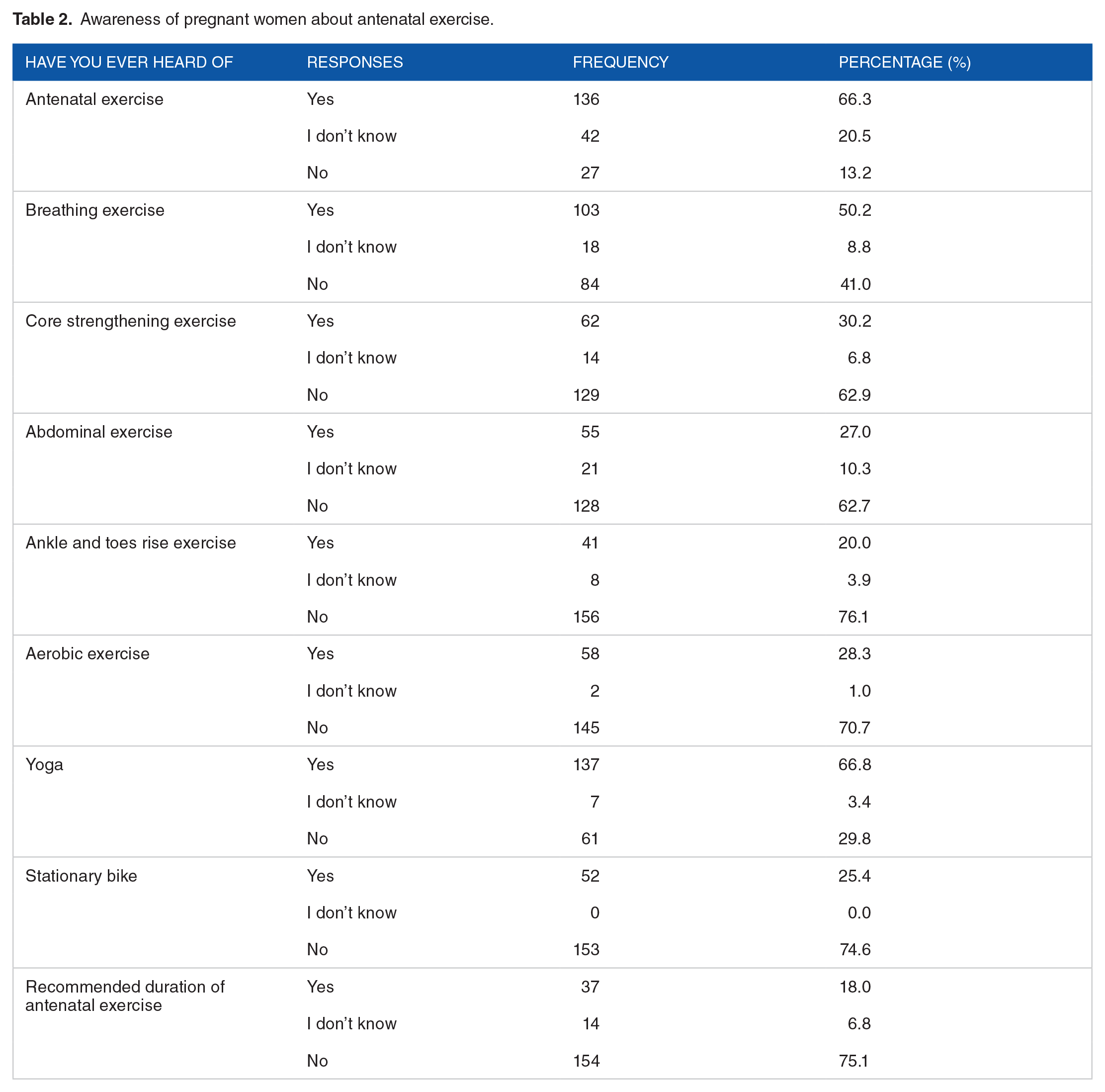
The questionnaire included several questions to evaluate women’s awareness of antenatal exercise during pregnancy. Overall, the results revealed that most participants demonstrated good awareness regarding antenatal exercise. A significant proportion of participants correctly identified the common types of antenatal exercise during pregnancy. However, the awareness about the abdominal strengthening exercise was relatively lower, with only 27.0% of participants being aware of this exercise. Interestingly, a large segment (66.8%) of the included women acknowledged their awareness of Yoga during pregnancy, although the practice of this type of exercise is uncommon in Libyan culture. Regarding the recommended amount of antenatal exercise during pregnancy, participants exhibited poor awareness, with only 18.0% of them accurately knowing the recommended weekly exercise duration. Table 2 presents the participants’ responses to the awareness section of the study questionnaire.
Awareness of pregnant women about antenatal exercise.
Knowledge of antenatal exercise
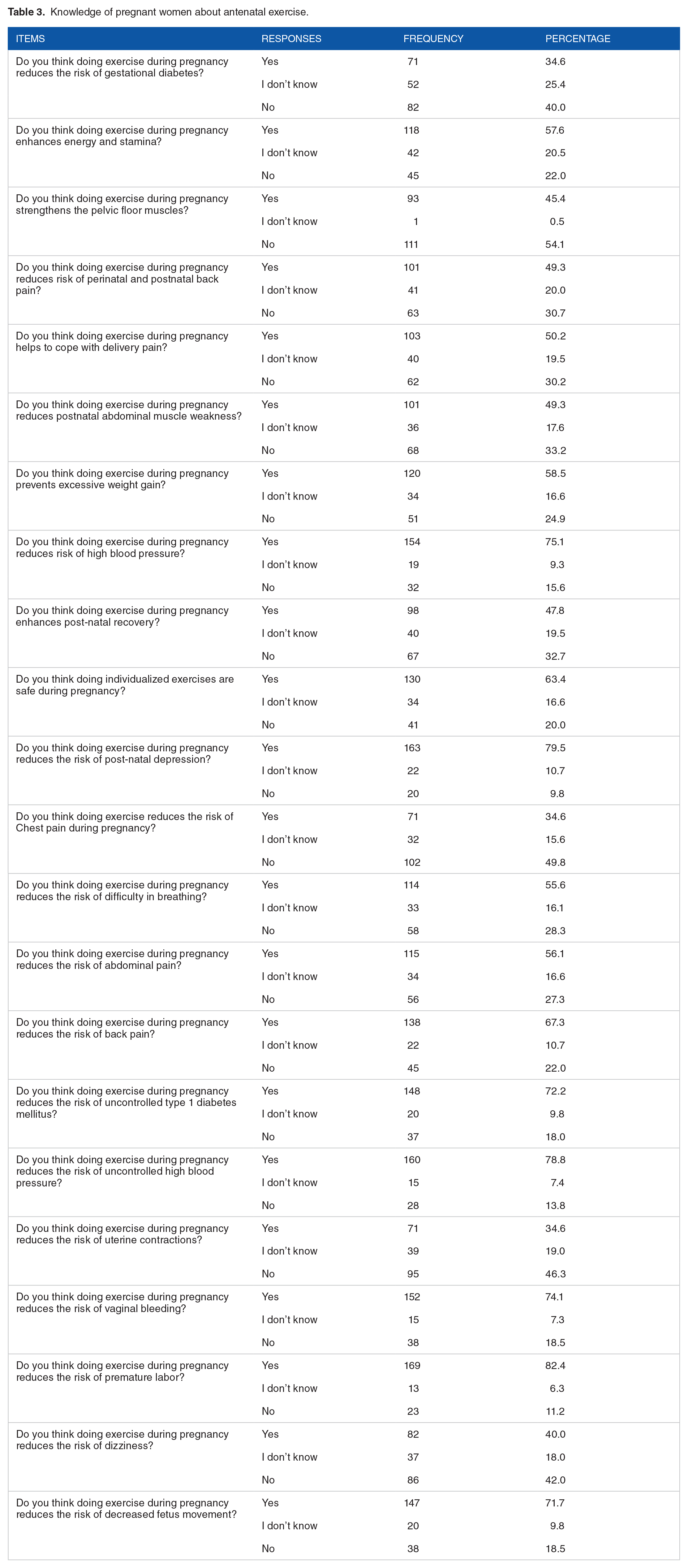
The study assessed the participants’ knowledge regarding antenatal exercise. Overall, 56.1% of participants demonstrated good knowledge, while 43.9% had poor knowledge. The mean knowledge score of all participants (n = 205) was 12.78 (SD = 5.29). Specifically, 57.6% of participants agreed that exercise enhances energy and stamina, and 47.8% recognized that regular exercise can improve pregnancy outcomes. When asked about exercise safety during pregnancy, 63.4% of participants correctly identified it as safe. Table 3 presents more details about this section.
Knowledge of pregnant women about antenatal exercise.
Attitude toward antenatal exercise
The study also examined the participants’ attitudes toward antenatal exercise. Participants were asked about their beliefs and feelings regarding the importance and feasibility of engaging in regular exercise during pregnancy. Results revealed that 47.8% of participants had a positive attitude toward antenatal exercise, expressing the belief that it is essential for their overall well-being. The mean Attitude score of all participants (n = 205) was 6.22 (SD = 3.20). However, only 15.1% of participants agreed that antenatal exercise suits the Libyan culture, the majority indicating a negative attitude toward antenatal exercise. Table 4 presents all responses to this section of the study.
Attitude of pregnant women toward antenatal exercise.

Practice of antenatal exercise
Results of this section showed that less than one-third (30.2%) of participants engaged in some form of exercise during pregnancy. The most common types of exercise reported were walking (66.8%), breathing exercises (34.1%), and relaxation exercise (41.4%). Among those who exercised, the majority of women did not reach the recommended exercise, which is not less than 3 times/week and for a minimum of 20 minutes per session.
The results also highlight the lack of doctors’ advice in referring to physiotherapy clinics or providing guidance and support regarding antenatal exercise. As high as 69.8% of participants reported that they did not receive directions to exercise, and only 3.9% had referrals to physiotherapy clinics. The main subjective reasons for not engaging in antenatal exercise by pregnant women were lack of time (35.1%), lack of knowledge (26.8%), fatigue (15.1%), and worries about harming the baby (10.7%; see Table 5).
Practice of antenatal exercise by pregnant women.
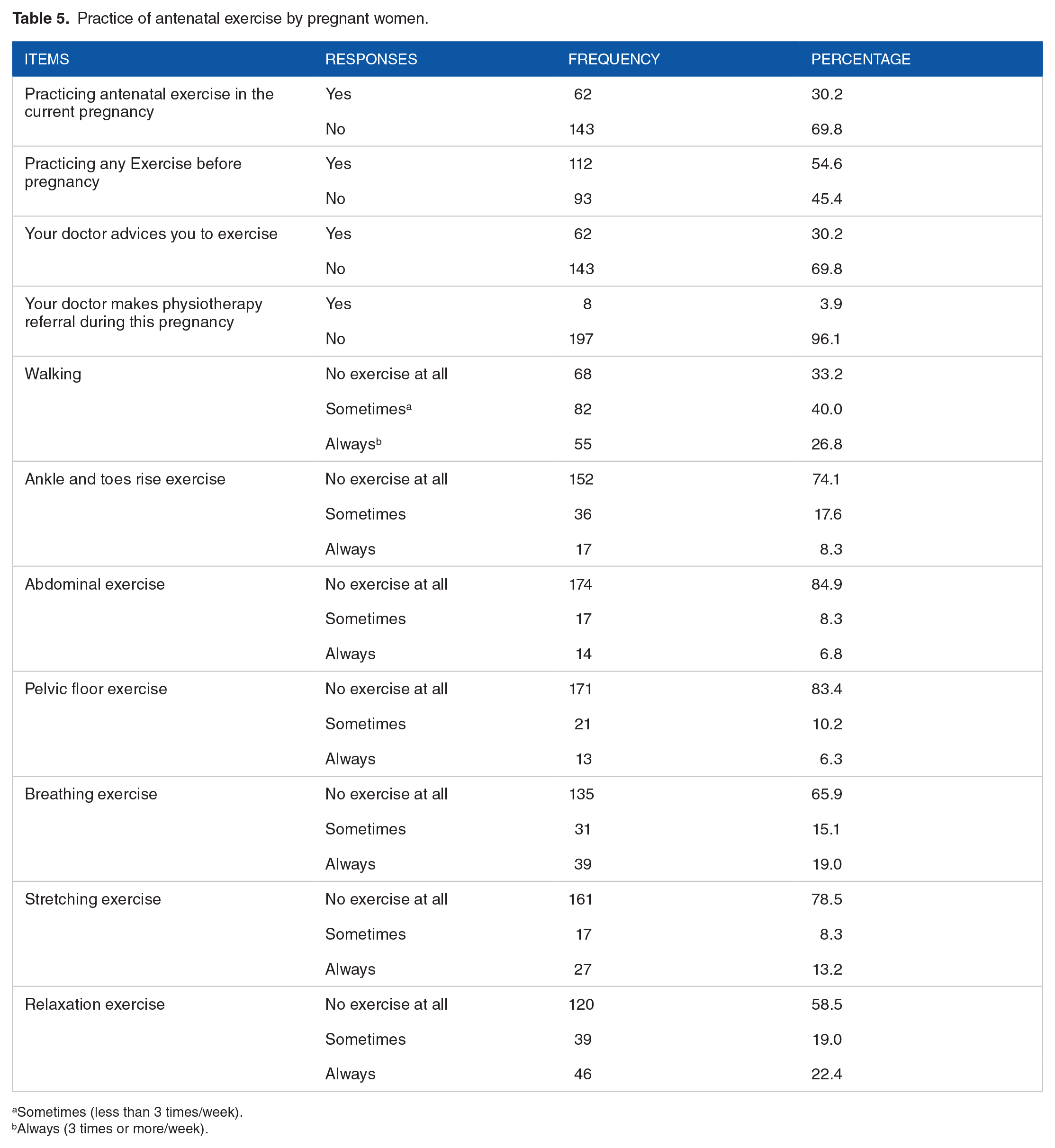
Sometimes (less than 3 times/week).
Always (3 times or more/week).
Factors associated with antenatal exercise
A binary logistic regression analysis was conducted to identify factors associated with the knowledge, attitude, and practice of antenatal exercise. The independent variables included the socio-demographic characteristics of study participants (see Supplemental File#1).
The model was statistically significant for knowledge, [χ2 (21, N = 205) = 185.46, P < .001], suggesting that it can distinguish between those with good and poor knowledge about antenatal exercise. The model explained between 59.6% (Cox & Snell R2) and 79.8% (Nagelkerke R2) of the variance in the dependent variable and correctly classified 89.3% of cases. Age, income, positive attitude, and practice of exercise before pregnancy significantly contributed to the model. The age adjusted odds ratio of (AOR = 1.22, 95% CI [0.98-1.52], P = .024) suggests that for every increase in age in years, participants were 1.22 times more likely to have good knowledge about antenatal exercise. For income, the adjusted odds ratio of (AOR = 5.89, 95% CI [0.85-4.96], P = .041) suggests that participants were 5.89 times more likely to have good knowledge about antenatal exercise for every increase in monthly income. The positive attitude adjusted odds ratio of (AOR = 3.47, 95% CI [2.29-5.27], P < .001) indicates that for every increase in positive attitude, participants were 3.47 times more likely to have good knowledge about antenatal exercise. Finally, the adjusted odds ratio of exercise practice before pregnancy (AOR = 0.26, 95% CI [0.07-0.88], P = .03) suggests that those who practiced exercise before pregnancy were 0.26 times more likely to have good knowledge about antenatal exercise. However, the practice of exercise before pregnancy does not seem to significantly contribute to the knowledge of antenatal exercise based on the AOR and the CI values.
For attitude, the model was statistically significant (χ2 (23, N = 205) = 283.79, P < .001), suggesting that it can distinguish between those with positive and negative attitudes about antenatal exercise. The model explained between 58.3% (Cox & Snell R2) and 77.8% (Nagelkerke R2) of the variance in the dependent variable and correctly classified 88.7% of cases. Only occupation, gestational trimester, and knowledge significantly contributed to the model. Employed women and those in their first trimester of pregnancy were less likely to have a positive attitude toward antenatal exercise by 4.4 times and 3.3 times, respectively. (AOR = 4.41, 95% CI [0.97-5.73], P = .026) and (AOR = 3.32, 95% CI [1.68-4.35], P = .035) respectively. However, pregnant women who have good knowledge were more likely to have a positive attitude by 2.4 times (AOR = 2.41, 95% CI [1.81-3.23], P < .001).
The results also indicated that unemployment status (AOR = 2.42, 95% CI [0.78-6.38], P = .030) and practicing exercise before pregnancy (AOR = 1.97, 95% CI [0.92-4.24], P = .02) were significantly associated with a higher likelihood of engaging in antenatal exercise. No significant associations were found between other socio-demographic characteristics and antenatal exercise practice. The model was statistically significant, [χ2 (22, N = 205) = 20.61, P < .001], suggesting that it can distinguish between those who practice antenatal exercise and those who do not. The model explained between 19.6% (Cox & Snell R2) and 24.1% (Nagelkerke R2) of the variance in the dependent variable and correctly classified 76.1% of cases.
Discussion
This cross-sectional study offers valuable insights into the awareness, knowledge, attitudes, and practice of antenatal exercise among 205 pregnant women receiving antenatal care at the Misrata Medical Center in Libya. This study found that less than half of a sample of expectant mothers in Libya had a good awareness, knowledge, or positive attitude to exercise, and even fewer engaged in exercise during pregnancy. The primary subjective reasons that deter pregnant women from participating in antenatal exercise were time constraints, limited awareness, fatigue, and concerns about potential harm to the baby. These findings provide a basis for understanding the current state of antenatal exercise in the region and shed light on potential areas for improvement in maternal healthcare.
The findings of this study align with previous research conducted in similar contexts. The results indicate that approximately half of the participants demonstrated good awareness, knowledge, and positive attitudes toward antenatal exercise. This is consistent with studies conducted in other countries, such as Saudi Arabia, 12 Ethiopia, 13 and Nigeria, 16 which reported similar levels of awareness and knowledge among pregnant women. However, the low practice rate observed in this study, where less than one-third of the sample reported engaging in antenatal exercise as recommended, is consistent with findings from various studies conducted globally. Studies conducted in different countries, including Saudi Arabia, 12 Brazil, 19 and Sri Lanka, 32 have reported low levels of antenatal exercise adherence, indicating a gap between intention and practice.
The discrepancy between knowledge/attitudes and practice observed in this study is a common challenge reported in the literature.12,19,33 Several studies have highlighted barriers to antenatal exercise, including time constraints, lack of motivation, fear of exertion or harm to the baby, and lack of guidance or information.13,15,19,34 These findings support the notion that knowledge and positive attitudes alone may not be sufficient to drive behavior change, and addressing barriers is crucial in promoting antenatal exercise practice.
To bridge this gap, interventions and educational programs have been proposed in previous research. 14 Studies have emphasized the role of healthcare providers in promoting antenatal exercise through counselling, education, and personalized recommendations. 35 Additionally, community-based interventions, such as prenatal exercise classes and social support networks, have been shown to be effective in promoting antenatal exercise. 36 By implementing a combination of these interventions and educational programs, healthcare organizations, communities, and governments can promote antenatal exercise, improve maternal health outcomes, and enhance the overall well-being of pregnant women and their infants.
Despite the above-proven interventions to promote antenatal exercise, women in developing countries often face numerous barriers that hinder their ability to exercise regularly.13,33 One major barrier is societal and cultural norms, which may discourage women from participating in physical activities due to traditional gender roles and expectations. 37 Cultural beliefs regarding appropriate behavior for women, limited autonomy, and restrictions on movement can further contribute to the lack of exercise opportunities.33,38 Economic constraints and limited access to resources, such as sports facilities, gymnasiums, or exercise equipment, are additional barriers that prevent women from engaging in regular exercise. 34 Lack of time due to household responsibilities, caring for children, and engagement in income-generating activities further limits the opportunity for women to prioritize physical activity. 35 Addressing these barriers requires comprehensive strategies that consider cultural context, economic empowerment, infrastructure development, and social support systems to create an enabling environment for women to engage in regular exercise and improve their overall health and well-being.
In Libya, pregnant women face a great deal of physical, mental, and emotional challenges during their pregnancy, 39 which can make it difficult to stay active and exercise regularly. In addition to the physical difficulties of exercise during pregnancy, cultural beliefs and misconceptions are significant factors that may explain why exercise is not a common practice among pregnant women in this country. One of the most prominent factors is the belief that pregnant women should not be exerting themselves. 40 This belief is particularly firm in traditional cultures, where pregnant women are often expected to rest and avoid any strenuous activities.35,38 This is based on the belief that pregnancy is a delicate condition and that any activity, no matter how mild, could put the mother and baby at risk. This can lead to pregnant women avoiding exercise, including walking, for fear of harming their babies. In certain cultures, there is also a stigma associated with pregnant women who exercise. 41 This stigma can be further reinforced by family members or community members who may not understand the physical and mental benefits of exercise during pregnancy and discourage it as a result.
Addressing these reasons for non-participation in antenatal exercise is crucial for healthcare professionals and policymakers to develop targeted interventions and support systems. By addressing these barriers and providing appropriate education, guidance, and resources, efforts can be made to promote the importance of antenatal exercise and empower pregnant women to make informed choices for their own health and the health of their babies.
Nevertheless, this study revealed poor awareness among healthcare providers (eg, obstetricians) about the importance of antenatal exercises, particularly those supervised by physiotherapists. Most participants in this study (69.8%) did not receive recommendations from their physicians, and only 3.9% had a referral to physiotherapy clinics. This alarming concern highlights the need for better education and training for healthcare providers on the benefits of antenatal exercises, especially those supervised by qualified physiotherapists, and how to promote them to pregnant women. The role of healthcare providers in promoting antenatal exercise seems a valid concern in African countries. Asante et al 33 conducted a study in Ghana and concluded that all healthcare providers should be responsible for providing education and support to ensure sustainable exercise practices during pregnancy. Improved awareness and collaboration among healthcare providers can help to improve maternal health outcomes and reduce the risk of complications during pregnancy and childbirth.
Aside from exercise practices, one of the most concerning findings of this study was the high prevalence of obesity among the studied sample of pregnant women. This is a major public health concern as obesity during pregnancy increases the risk of complications such as gestational diabetes, hypertension, pre-eclampsia, and preterm birth. 42 Pregnant women may gain excessive weight due to a variety of factors. An improper diet is the most obvious factor that can lead to an overweight pregnant woman. 43 Libya, as well as many other developing countries, are still in the process of transitioning to modern diets, which are often high in fat, sugar, and processed foods. These diets can lead to excessive weight gain if they are not balanced with adequate amounts of nutritious foods. Furthermore, many pregnant women in these countries may not have access to the resources or education needed to make healthy dietary choices. 13 The findings suggest an urgent need for targeted interventions to address obesity among pregnant women in Libya, including promoting healthy eating habits and regular physical activity.
Limitations
This study had some limitations that should be considered. Firstly, the study’s findings may be limited due to sampling bias, as the sample may not represent the broader population and generalizability to other geographical locations may be compromised. Another limitation of this study pertains to the unique cultural context of Libya, which may differ significantly from Western countries. While this current study focused on antenatal exercise practices in Libya, the findings may not be directly transferable to countries with distinct cultural norms and expectations about pregnancy and exercise. Therefore, caution should be exercised when extrapolating these results to populations outside of Libya, as cultural factors play a substantial role in shaping individuals’ attitudes and behaviors related to antenatal exercise. 44
Furthermore, while logistic regression analysis is a valuable statistical tool, it is not without limitations. Overfitting can occur if the model becomes overly complex or includes too many variables, affecting its generalization to new data. 45 Therefore, we included a sufficient sample size to ensure stable estimates. Causality cannot be inferred solely from logistic regression, regardless of the size, direction, or significance of the ORs, necessitating caution in interpreting associations as causal relationships. 46 As with any statistical approach, the limitations of logistic regression underscore the importance of understanding its constraints and employing complementary methods to mitigate potential biases and inaccuracies in research findings. 47
Lastly, this study relied on quantitative research methods exclusively. We employed quantitative data analysis techniques to address our research question, which provided valuable insights into the knowledge, attitudes, and practice of antenatal exercise and associated factors. However, the absence of qualitative or mixed methods design limited our ability to capture the nuanced perspectives, experiences, and motivations of pregnant women in Libya regarding antenatal exercise. Qualitative or mixed methods research would have offered a more holistic understanding of the cultural and sociocultural factors influencing exercise behaviors during pregnancy, allowing for a richer exploration of participants’ experiences.
Despite these limitations, our study contributes valuable insights into the context of antenatal exercise in Libya, offering a foundation for future research avenues that may incorporate qualitative or mixed methods approaches to further explore the cultural intricacies surrounding pregnancy and exercise in this unique context.
Conclusion
Antenatal exercise is an essential aspect of prenatal care that can help to promote the health of both the mother and baby. Awareness, knowledge, attitude, and practice are the key factors that can help expectant mothers unlock the benefits of antenatal exercise. Overall, the results of this study revealed that nearly half of the participants demonstrated good awareness, knowledge, and positive attitudes regarding antenatal exercise. However, less than one-third of participants engaged in some form of exercise during pregnancy. These findings demonstrate the existence of a gap between awareness/knowledge/attitudes and actual practice of antenatal exercise. The main subjective reasons for pregnant women not engaging in antenatal exercise were lack of time, poor knowledge, fatigue, and worries about harming the baby. These identified barriers to practice are consistent with the literature, highlighting the need for targeted interventions and support systems. Healthcare providers can play a crucial role in promoting antenatal exercise by addressing barriers, providing guidance, and integrating exercise counselling into routine prenatal care. Community-based interventions and educational programs should be developed to empower pregnant women with the knowledge, skills, and support necessary to engage in safe and effective antenatal exercise. By addressing these challenges, it is possible to improve adherence to recommended antenatal exercise guidelines and enhance maternal and fetal health outcomes in Libya and other similar contexts.
Supplemental Material
sj-docx-1-rpo-10.1177_27536351231212132 – Supplemental material for Exploring Antenatal Exercise: Knowledge, Attitudes, Practices, and Influencing Factors among Pregnant Women in Libya
Supplemental material, sj-docx-1-rpo-10.1177_27536351231212132 for Exploring Antenatal Exercise: Knowledge, Attitudes, Practices, and Influencing Factors among Pregnant Women in Libya by Alhadi M Jahan and Salima M Anaiba in Advances in Rehabilitation Science and Practice
Supplemental Material
sj-docx-2-rpo-10.1177_27536351231212132 – Supplemental material for Exploring Antenatal Exercise: Knowledge, Attitudes, Practices, and Influencing Factors among Pregnant Women in Libya
Supplemental material, sj-docx-2-rpo-10.1177_27536351231212132 for Exploring Antenatal Exercise: Knowledge, Attitudes, Practices, and Influencing Factors among Pregnant Women in Libya by Alhadi M Jahan and Salima M Anaiba in Advances in Rehabilitation Science and Practice
Footnotes
Acknowledgements
We would like to extend our heartfelt gratitude to all the participants who generously dedicated their time and efforts to take part in this research. Their willingness to share their experiences and provide valuable data was instrumental in the success of this study. Without their cooperation and participation, this research would not have been possible. Also, we are truly grateful for the contributions of all staff members and institutions involved in this research, and we recognize the significance of their collective efforts in bringing this study to fruition.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.