
Abstract
Objectives:
This study was aimed to assess the knowledge and practices of pregnant women about iodized salt and its availability in their households in Hawassa city, Ethiopia
Methods:
A community-based cross-sectional study design was conducted among pregnant women with a total sample size (N) = 553 in Hawassa city. A multi-stage sampling technique was employed. First, four sub-cities of Hawassa city (out of eight sub-cities) were selected using the lottery method. Households of pregnant women in each selected sub-city were identified and screened. Finally, representative samples were drawn using systematic random sampling technique.
Results:
A total of 537 pregnant women was included, a response rate of 97.1%. This was due to incomplete data for nine and participation refusal for seven participants. The mean age of the participants was 26.98 ± 4.75 years. About 52.51% and 52.33% of the respondents had good knowledge and good salt handling practices, respectively. Regarding availability of iodized salt, 65.55% of pregnant women (31.66% salt with iodine level ⩾15 parts per million (ppm) and 33.89% salt with iodine level <15 ppm) had iodized salt and the remaining 34.45% non-iodized salt (0 ppm) respectively.
Conclusion:
Availability of iodized salt in households of pregnant women was 65.55% (>0 ppm). More than one-third of pregnant women in Hawassa city are utilized non-iodized salt (0 ppm). Nearly half of the pregnant women in Hawassa city had poor knowledge and poor practice about iodized salt. Hawassa city Health Department along with concerned stakeholders should invest more effort to increase awareness about iodized salt and how to handle it safely in households.
Introduction
Iodine is a trace micronutrient that is essential for the metabolic pathway of the human body, development of brain tissue, and maturation of the central nervous system. It is an essential component of the thyroid for the synthesis of thyroid hormones (thyroxine and triiodothyronine).1,2 Due to marked physiological changes and increased production of thyroid hormones, iodine requirement during pregnancy increases more than 50% compared with non-pregnant women of reproductive age. 3 Pregnant women who are unable to get sufficient amount of iodine (150–249 μg/L) required during pregnancy develop a disorder called iodine deficiency disorder (IDD). 4
Severe iodine deficiency problems manifested by goiter (maternal hypothyroidism) and neurological problems including mental disability (mental retardation) and neurological cretinism (deaf Mutism, mental deficiency, spasticity, and squint) that permanently harm the fetus cause the fetus to develop with lower learning ability (lower intellectual quotient), reduced capacity, and less investment in education and creativity. 3 Congenital deformity, stillbirth, and irreversible fetal brain damage are also poor obstetric outcomes caused by insufficient intake of iodine during pregnancy.4,5
Globally, more than two billion people are affected by IDD. Pregnant and lactating women and children of school age are part of the population categorized highly vulnerable groups by IDD. Among school-aged children who are iodine insufficient, more than half reside in two regions (78 million in Southeast Asia and 58 million in Africa). Europe is also one of the continents where IDD is highly prevalent which accounting for 30.5 million school age children being iodine insufficient. 2
An additional need for iodine is required by the fetus, maternal iodine requirement to maintain maternal euthyroidism, and increased renal excretion of iodine during pregnancy causes pregnant women to fall under a highly vulnerable group for iodine deficiency. 2 The global urinary iodine concentration data in pregnant women compiled from 65 countries indicates that iodine intake in pregnant women is insufficient in 37 countries. 6
Despite its irreversible effect on the developing fetus, IDD is an easily preventable public health problem. According to the World Health Organization, International Council for Control of Iodine Deficiency Disorders and United Nations International Children’s Fund recommendations, Universal Salt Iodization (USI) is a safe, cost-effective, and sustainable strategy to deliver sufficient iodine to all individuals living in the iodine deficit country. It is iodization of all human and livestock salt, including salt used in the food industry by considering the required amount of iodine to be delivered to individuals living in iodine-deficient countries. 7 IDDs can be prevented, if 90% or more households from iodine deficient country are available with iodized salt. 7
Ethiopia is one of the Sub-Saharan countries that has implemented USI strategy for more than a decade to prevent iodine deficiency. Currently, the availability of iodized salt to households at national level is 88.8%; however, the country’s goiter rate ranges between 14% and 59%, which leads Ethiopian pregnant women to have 50,000 stillbirths annually and at least one out of 1000 births to be a cretin (permanent mental disability). Poor knowledge about iodized salt and low dietary intake of foods fortified with iodine are the major contributing factors for insufficient iodine within households.8–10 Currently, the iodized salt coverage for households at the national level is 88.8%, but only 26% of households use adequately iodized salt. 11 There is a scarcity of evidence regarding the knowledge and practices of pregnant women regarding iodized salt and its availability in their households, both at the national level in general and in Hawassa city in particular (Hawassa city health department report in 2019). Therefore, this study aimed to assess the knowledge and practices of pregnant women about iodized salt and its availability in their households in Hawassa city administration.
Objective
General objective
To assess the knowledge and practice of pregnant women about iodized salt and its availability in their households in Hawassa city administration.
Specific objective
To assess the knowledge of pregnant women about iodized salt in Hawassa city administration.
To assess the practice of pregnant women about iodized salt utilization and its availability in their households in Hawassa city administration.
Methodology
Study area
This study was conducted in Hawassa city administration, the city of the Sidama Regional State located at 70°03′ latitude and 89°28′ east longitude. It is 270 km south of Addis Ababa, the capital city of Ethiopia and 1708 m above sea level. The city has 8 sub-cities and 32 kebeles (the lowest administrative structure in Ethiopia) inhabited by a total population of 376,539, of which 187,517 were men and 189,022 women. The city has 7 hospitals (3 public and 4 private hospitals), 12 public health centers (11 governmental and 1 non-governmental), 13 private special clinics, 19 health posts, 7 diagnostic laboratories, 111 drug stores, and 14 pharmaceutical suppliers. According to a health department report of the city administration, it was estimated that about 13,028 pregnant women were living in the city in the 2020 Ethiopian fiscal year.
Study design and period
A community-based cross-sectional study was conducted among pregnant women between October and November 2020.
Inclusion and exclusion criteria
Inclusion criteria
All pregnant women who permanently reside in eight sub-cities of Hawassa city and who are not medically restricted to take iodized salt by physician (health professionals) were candidates for this study.
Exclusion criteria
Pregnant women who are restricted to take iodized salt for medical reason and those who did not give consent to participate in the study were excluded from this study.
Source and study population
Source population
The source population for this study was all pregnant women residing in Hawassa city administration
Study population
The study population consisted of pregnant women living in households in selected sub-cities of Hawassa city.
Sample size determination
The sample size was calculated using Open Epi version 3.03 Stat Cal c. software by considering 95% confidence level, proportion of availability of iodized salt, p = 37.7%, 12 margin of error, d = 5%, design effect = 0.5, and non-response rate = 5% which gives the total sample size, n = 553.
Sampling procedure
A multistage sampling technique was employed to determine the samples used in this study. First, the number of sub-cities in Hawassa city administration (a total of 8 sub-cities) was determined and four sub-cities (Bahel adarash, Mehal ketema, Addis ketema, and Tabor) were selected using lottery method. Households of pregnant women in each selected sub-city were identified and screened. Representative samples were drawn from each selected sub-city through proportionally allocating samples to the size of the study population. Lottery method was used to determine the first household with a pregnant woman and systematic random sampling technique is employed to determine the next participating pregnant women. Only one pregnant woman was interviewed if more than two pregnant women resided in a single household (see Figure 1).

Schematic representation of sampling procedure to assess the knowledge and practices of pregnant women about iodized salt and its availability in their households in Hawassa city, 2020 (N = 553).
Operational definition
Availability of iodized salt: Salt used by pregnant women for cooking within the preceding 24 h and observed to have a color change of salt or presence of iodine by the test kit.
Adequately iodized salt: Salt with an iodine level ⩾15 parts per million (ppm; deep blue color of salt) after the salt was tested using the kit.
Inadequately iodized salt: Salt with an iodine level <15 ppm (light blue color of salt) after the salt was tested using the kit.
Non-iodized salt: Salt with an iodine level of = 0 ppm (no color change of salt) after the salt was tested using the kit.
Good knowledge: Pregnant women who answered half and more than half (⩾50%) of knowledge questions correctly.
Poor knowledge: Pregnant women who answered less than half (<50%) of knowledge questions correctly.
Good practice: Pregnant women who answered practice questions more than or equal to the mean correctly.
Poor practice: Pregnant women who answered less than the mean of the practice questions correctly.
Data collection tools and procedures
Data were collected through an interviewer-administered semi-structured questionnaire adapted from previous similar literatures.13,14 The questionnaire was developed in English and translated into Amharic and Sidaamu Afoos (common languages commonly spoken by Hawassa city residents) and finally retranslated into English by language translators to check consistency. The questionnaire was structured to obtain information on sociodemographic characteristics (monthly income, educational status, family size, and occupational status), knowledge about iodized salt, and practices of iodized salt utilization (exposure of salt to sunlight), place and duration of salt storage and testing salt for iodine using a Rapid Iodine Test Kit (BMI Kits International, Chennai, Tamil Nadu, India). The reliability test result indicated that Cronbach’s alpha is 82.3%.
To assess the iodine content in the salt, interviewers asked pregnant women to obtain a teaspoon of salt used for cooking within the preceding 24 h. The salt was tested for iodine by interviewers using a Rapid Iodine Test Kit (MBI Kits International). This is an iodized salt test kit for assessing salt in home to home visit for salt fortified with either potassium iodide or potassium iodate with 89.8% and 65.8% sensitivity and specificity, respectively. 15
The kit includes two white ampules each containing 10 mL solutions called test solutions; one red ampule containing 10 mL solution called recheck solution; one white plastic cup; one color chart with circular color spots showing 0 ppm, below 15 ppm, and above or equal to 15 ppm; and one instruction sheet all fitting into a handy pocket size kit 15 (see Figure 2).

Components of a Rapid Iodine Test kit (BMI kits international) used to assess the availability of iodized salt in households of pregnant women living in Hawassa city, 2020 (N = 553).
Data were collected by six female Bachelor of Science in clinical laboratory health professionals who were fluent speakers of both Amharic and Sidaamu Afoos. Two health professionals, who were specialized in Master of Science in a clinical chemistry and who had experience in supervising previous similar study, were recruited as supervisors for this study. If participants were not present in households selected for data collection, a revisit was made otherwise a pregnant woman in the next household was considered.
Data quality assurance
A week before actual data collection, data collectors and supervisors were trained for 1 day about the procedures to be followed during testing salt for iodine. The pretest was conducted on 5% (28 participants) of the sample in Yirgalem town (115 km away from Hawassa city in the southern direction) to check the validity and consistency of the data collection tool. Ongoing supervision was made to check whether all the questionnaires were appropriately completed and the recorded information made sense or not. A Rapid Iodine Test Kit was used (before the kit expiry date) to test the salt.
Statistical analysis
Completeness of data was checked on daily basis by supervisors during data collection and if data were missed, an interviewer is returned back to pregnant women and completes the missed data. After the data collection process is completed, each data was entered to Epi Data version 3.0 software and then exported to Statistical Package for Social Sciences version 20. Frequency distribution, mean, and percentage were calculated to know the magnitude for each variable. Tables, pie charts, and bar charts were used to describe the final result.
Result
Sociodemographic characteristics
A total of 537 pregnant women participated in the study, a response rate of 97.1%. This was due to incomplete data for nine and participation refusal for seven participants, respectively. The mean age of participants was 26.98 ± 4.75 years. In all, 519 (96.6%) was married and 3.4% were others. The majority were Protestant religion followers (60.1%) followed by Orthodox (34.3%), Muslim (5%), and Catholic (0.6%), respectively. About 157 (29.2%) participants attended secondary school, 28.9% college and above, 28.3% primary, and the remaining (13.6%) had not attended formal education at all. Regarding the occupational status, the majority (35.0%) were housewives followed by government employee (24.0%), merchant (21.0%), student (9.3%), self-employed 39 (7.3%), and daily laborer (3.4%) (see Table 1).
Sociodemographic characteristics of pregnant women living in Hawassa city, 2020 (N = 537).

ETB: Ethiopian birr; US$: US dollar
Knowledge about iodized salt
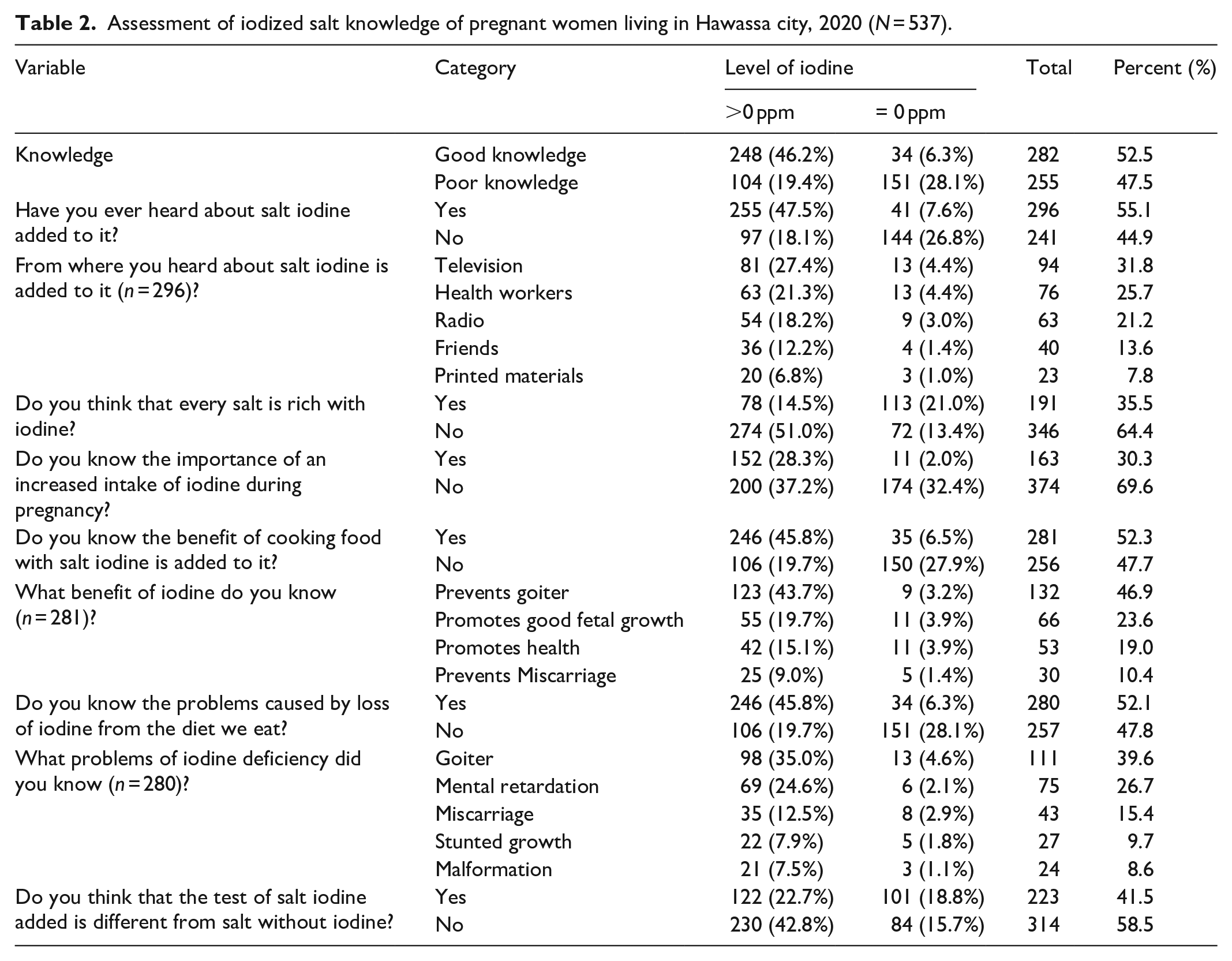
Among nine questions used to assess knowledge of pregnant women about iodized salt, 52.51% had good knowledge about iodized salt. In all, 296 (55.1%) had previously heard about iodized salt. Of those who heard about iodized salt, 17.5% heard from television, 14.2% from health workers, 11.7% from the radio, 7.4% from friends, and 4.3% from printed materials (leaflets about iodized salt) (see Figure 3 and Table 2).

Knowledge of pregnant women about iodized salt in Hawassa city, 2020 (N = 537).
Assessment of iodized salt knowledge of pregnant women living in Hawassa city, 2020 (N = 537).
Practices about iodized salt
About 52.33% pregnant women had good iodized salt handling practice in their households. The majority of the participants bought their salt from small shop (57.2%) followed by supermarkets (24.0%) and open market (18.8%), respectively. About 71.7% pregnant women bought their salt packed with original covering, 63% stored salt in containers having cover, and 43.2% stored salt in the dry and cool area (see Figure 4 and Table 3).

Salt handling practices of pregnant women living in Hawassa city, 2020 (N = 537).
Assessment of salt handling practices of pregnant women living in Hawassa city, 2020 (N = 537).

Availability of iodized salt in households of pregnant women
A teaspoon of salt was taken from households of pregnant women used for cooking within the preceding 24 h for determining the iodine level within the salt. Nearly one-third of the participants (31.66%) had been using salt with iodine level >15 ppm, 33.89% of women used salt <15 ppm, and 34.45% used non-iodized salt (0 ppm) (see Figure 5).
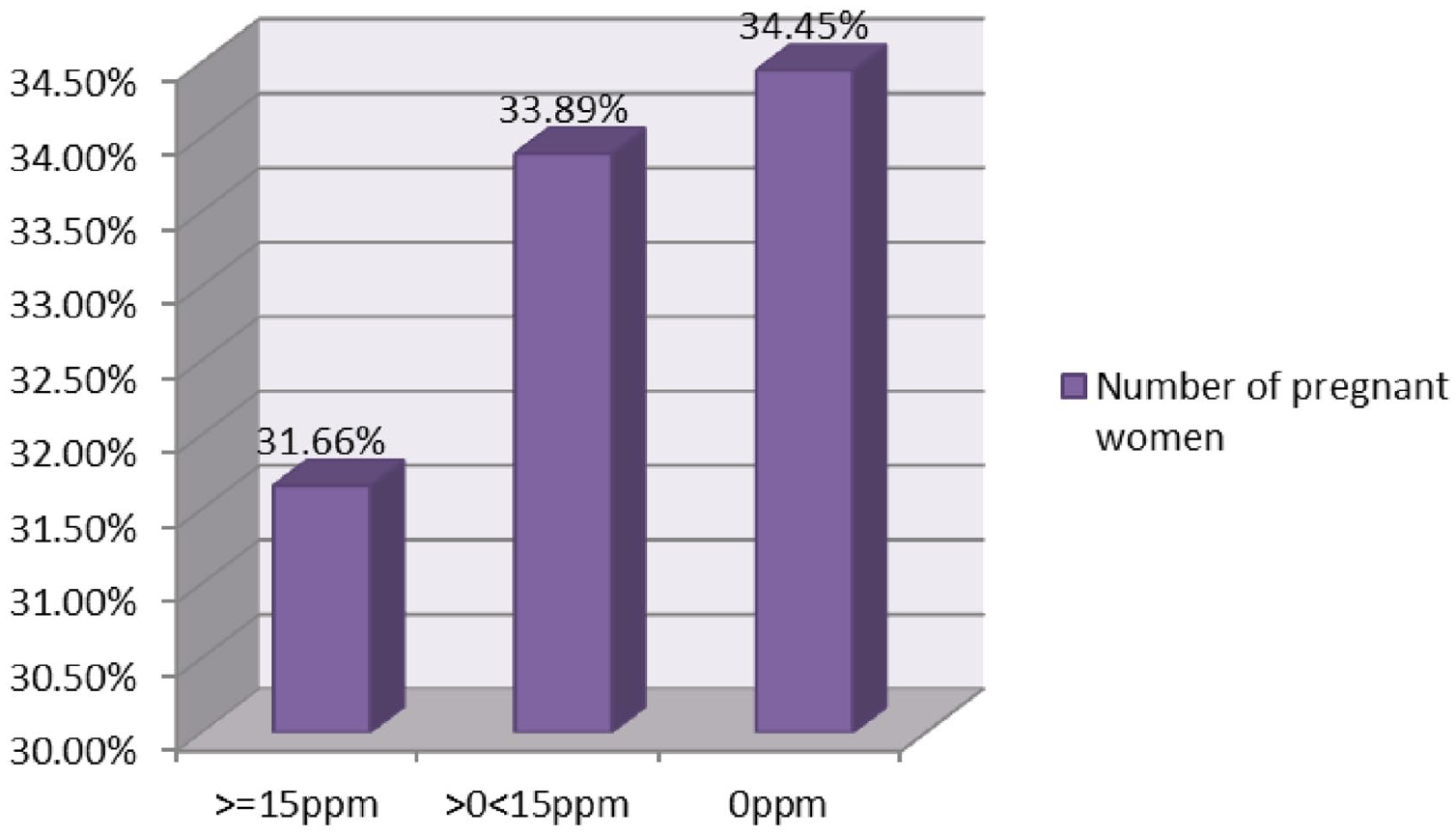
Availability of iodized salt in households of pregnant women living in Hawassa city, 2020 (N = 537).
Discussion
Among the 537 pregnant women involved in this study, 52.5% (95% confidence interval (CI): 48.2–56.8%) had good knowledge about iodized salt. Among those who were knowledgeable, 47.0% of women responded that salt rich with iodine prevents goiter followed by promotes fetal growth (23.7%) and improves maternal health (19.0%), respectively. A study which was conducted in Ghana found that 59.3% pregnant women were knowledgeable about salt rich with iodine. 16 This might be due to a special focus of Ghanaian government toward improving maternal and child health problems related to iodine deficiency. 17
The knowledge of pregnant women about iodized salt in this study was lower as compared with the study conducted in Ambo town health institutions. 18 This might be due to the difference both in the study area and in the study population. The previous study was conducted among pregnant women attending antenatal care service in Ambo town health institutions where education toward improving the nutritional status of pregnant women is given as one part of the service and may account for better knowledge for the previous study.
The knowledge of pregnant women living in Hawassa city was in consistent with the study conducted at Arbaminch town, southern Ethiopia, where 52.8% pregnant women were knowledgeable about iodized salt. 19 This might be due to the similarity in the study setting; both studies were conducted among pregnant women living in urban residences and might have similar accessibility of information through media. However, the knowledge of pregnant women living in Hawassa city was more as compared with the study conducted at Srinagarind Hospital, north-eastern region of Thailand, where only 33.3% pregnant women knew about iodized salt. 14 This difference might be due to the difference both in study setting and in the study population. The previous study was institution based and the participants were only pregnant women coming for their first antenatal visit while the present study is conducted at the community level and involves all pregnant women (pregnant women with history of more than one antenatal visits and might have obtained information about iodized salt in their earlier antenatal visits).
About 52.3% (95% CI: 48–56.8%) pregnant women had good salt handling practice in Hawassa city. This is lower than salt handling practices of pregnant women in Ambo town, Oromia regional state, Ethiopia, where three-quarters of respondents have good salt handling practice. 20 This difference might be due to the difference in the study area. The previous study was conducted on pregnant women coming for antenatal care visits that might have more access to health education about iodized salt utilization and may account for good practices of handling iodized salt. However, it is greater as compared with the study conducted in Thailand, where only 23.7% pregnant women had good practice of iodine supplementation. 14
Among households of pregnant women tested for iodine using the kit, 31.66% households have salt with iodine level ⩾15 ppm (deep blue color of salt), 33.89% <15 ppm (light blue color of salt), and 34.45% with 0 ppm (no color of salt). This is in consistent with the study conducted in Goba town, Bale zone, Oromia regional state of Ethiopia 18 and might be due to the similarity of the study area. Both this and the previous study were conducted on urban residence dwellers and might have similar access to information regarding nutritional education including iodized salt. Availability of iodized salt with iodine level ⩾15 ppm in households of pregnant women in Hawassa city was too low (31.66%). It was nearly reduced by half compared with salt availability in households of pregnant women in Kimbibit District, Oromia Regional State, Ethiopia. 21 This difference might be due to Kimbibit district is located near the trading center of the nation (addis ababa) by which iodized salt can be easily accessed as per the demand of pregnant women in the district.
In Ethiopia, a ban has been made by Salt Iodization Council of Ministers Regulation No. 204/2011 for processing, importing, and transporting non-iodized salt for edible consumption. According to the regulation, any inspector may inspect any processing, storage, transporting, or sales premises to ascertain that salt intended for human consumption is iodized. 22 However, salts supplied from small shops and open market have either lower or absence of iodine in the salt.18,23 This might be account for the lower availability of iodized salt in Hawassa city as the majority purchased salt from small shops and open market.
Limitation of the study
Rapid Iodine Test kit (BMI international kits) which was used for this study is not a very accurate assay for iodine content in the salt. It is based on the principle that the kit estimates the level of iodine based on the color change observed after testing salt for iodine using the kit. However, the kit is an easy, effective, and rapid method of assessing the iodine content of salt at the field or home to home visit. 15
Conclusion
Availability of iodized salt in households of pregnant women living in Hawassa city was low. More than one-third of pregnant women in Hawassa city are utilized non-iodized salt (0 ppm). Nearly half of pregnant women in Hawassa city had poor knowledge and poor practice about iodized salt, yet knowledge and practice play a major contribution in increasing access and availability of iodized salt in households. Hawassa city Health Department along with concerned stakeholders should invest more effort to increase awareness about iodized salt and how to handle it safely in households.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221115490 – Supplemental material for Knowledge and practices of pregnant women about iodized salt and its availability in their households in Hawassa city. Community-based cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221115490 for Knowledge and practices of pregnant women about iodized salt and its availability in their households in Hawassa city. Community-based cross-sectional study by Ketemaw Negese, Semahegn Tilahun, Aychew Kassie and Bamlaku Birie in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Hawassa city administration health extension workers for their unreserved contribution in screening and identifying pregnant women households in Hawassa city. Hawassa city Health Department deserves thanks for the provision of Rapid Iodine Test kit.
Author contributions
KN conceived and designed the study, performed statistical analysis and drafted the paper. ST, AK and BB participated in study design, closely supervised the overall undertaking of the study and participated in writing the paper. All authors contributed to the data analysis and interpretation and read and approved the final version of the paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Research Ethics Committee of Mizan-Tepi University, College of Medicine and Health Sciences with a reference number, MTU/CHS/00741/2020.
Informed consent
Written informed consent was obtained from all the study participants or/and legally authorized representatives of the study participants before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.