
Abstract
Background
Cancer is a major burden of disease worldwide which continues to rise. Prevalence of falls increases with age, whilst those with a diagnosis of cancer have also been found to be predisposed to a greater risk of falls, partially due to impaired balance. Exercise programs in older adults have been shown to improve balance and reduce fall risk.
Objective
The aim of this study was to explore the effectiveness of a 10-week circuit training program on balance and fear of falling (FoF) among adults diagnosed with cancer.
Methods
Participants (n = 12) completed a 14-item balance (Mini-Balance Evaluation Systems Test (BESTest)) and FoF (Falls Efficacy Scale - International (FES-I)) assessment prior to taking part in a 10-week circuit training program. Upon completion of the program, participants completed a post-assessment, consisting of the Mini-BESTest and FES-I.
Results
Balance significantly improved, as measured by the Mini-BESTest (p = 0.003; mean difference: 15.2%; BCa 95% CI: 10.1% to 20.8%), with significant improvements in three of the four subcomponents (Reactive Postural Control: p< 0.001; Dynamic Gait: p< 0.001; Anticipatory Postural Adjustments: p = 0.046) following the 10-week circuit training program. FoF significantly decreased following the program (p = 0.026; mean difference: −4.8; BCa 95% CI: −8.1 to −1.9).
Conclusion
A 10-week circuit training program significantly improved balance and reduced FoF among older adults diagnosed with cancer. Such exercise interventions could be considered as part of routine care following a diagnosis of cancer, as they may help reduce healthcare costs and improve quality of life among people with cancer.
Introduction
With an estimated 10 million deaths and 20 million new cases worldwide in 2022, cancer remains a major burden of disease which continues to rise. 1 In the United Kingdom alone, there were over 375,000 new cancer cases reported between 2016 and 2018. 2 Thirty-six percent of diagnosed cancers in the United Kingdom are among individuals aged 75 or older, with the greatest incidence among individuals aged 85–89 years old. 3
A fall is defined as ‘an event that results in a person coming to rest inadvertently on the ground or floor or other lower level’. 4 It is well established that the incidence of falls increases with age, 5 with around one third of adults aged 65 and older expected to experience at least one fall in any 12-month period, rising to half of those aged 80 and over. 6 Experiencing a fall can result in many detrimental physical (e.g. fractures and dislocations) and psychological (e.g. fear of future falls, loss of confidence and loss of independence) health outcomes. Risk factors for falls are multifactorial, particularly among older adults. Loss of coordination, muscle weakness, slower response times and reduced proprioceptive feedback are all associated with increased age, as well as influencing an individuals’ postural control; thus, increasing the likelihood of experiencing a fall.7–10
Research indicates that incidence of falls is greater among people with cancer in comparison to those without,11–14 potentially due to the symptoms of the cancer, as well as the side effects of surgery and treatments (e.g. impaired balance, cancer-related fatigue and muscle weakness). 15 One study reported that almost half (48.3%) of cancer survivors experienced a balance impairment, mainly due to vestibular dysfunction. 16 Research also indicates that an individual is at a greater risk of falling if they undergo surgery or adjuvant treatment for their cancer.17–19 Other research contradicts these findings, reporting no difference in incidence of falls between those with and without a diagnosis of cancer,20–22 potentially due to the great variation in cancer type, stage and associated symptoms, although an association cannot be ruled out.
Upon receiving a diagnosis of cancer, there is no clear guidance on the recommendation of exercise from oncologists or healthcare professionals in the United Kingdom. This is despite numerous studies showing the positive effect of exercise in older adults, on multiple health outcomes, including improved balance, thus helping to reduce the risk of falls.23,24 There is, however, limited research on exercise programs among individuals with cancer, despite exercise appearing feasible, safe and effective in improving physical function. 25 Circuit training is a quick, easy way to implement exercise into an individual’s weekly routine, whilst also easily adaptable to suit a range of abilities. Limited research explores the benefits of circuit training in people with cancer and the impact this has on their balance and fear of falling (FoF), with that currently available appearing effective at increasing muscle mass and physical function.26,27
The aim of this study, therefore, is to explore the effectiveness of a 10-week circuit training program on balance and FoF among individuals with cancer. It is hypothesised that the circuit-training program will improve measures of balance and reduce FoF in individuals who have received a diagnosis of cancer.
Methods
Ethical approval and study design
The study was approved by Bishop Grosseteste University’s research ethics committee (REC 29–23). A quasi-experimental study design was used with a 10-week follow-up period, where balance and FoF were assessed at baseline (before circuit training program) and following the circuit training program (minimum of 10 weeks).
Participants
Participants were recruited through self-referrals to an existing circuit training intervention designed for individuals who have had a cancer diagnosis. Within the online referral form, there was an option to opt into the current research study, whereby the researcher then contacted these individuals regarding their interest in the proposed study. Eligible participants were sent an information sheet via email detailing the study and were given the opportunity to ask questions prior to arranging a study visit to a university laboratory to complete the assessments. All participants provided written informed consent.
Inclusion criteria for the study included: (1) individuals who had a previous diagnosis of cancer; (2) aged 50 or over; (3) had the ability to read and understand English; (4) did not have any condition which affected their cognition, thus had the ability to understand the information sheet and what the study entailed.
Those who were under the age of 50 could not read or understand English or were deemed not to have the cognitive capacity to participate were excluded from the study. Any participants who were deemed a high fall risk during the balance assessments by the researcher were also excluded from the study.
Data collection
Anthropometric and demographic information was obtained, along with details of the participants’ cancer diagnosis. Participants were also asked whether they had experienced any falls in the past 12 month, and of their current exercise behaviour, with the options ‘never exercised’, ‘currently exercises’ and ‘exercised previously but not currently’.
Participants were then asked to complete the Falls Efficacy Scale – International (FES-I), in the presence of the researcher, to explore their FoF in differing daily scenarios. The FES-I has been used in other cancer populations previously 28 and is shown to be a reliable test of FoF. 29
Participants completed the Mini-Balance Evaluation Systems Test (BESTest) unshod in a quiet university laboratory. Participants were advised to rest as required throughout the assessment. The Mini-BESTest has been shown to be a valid measurement tool to assess balance in a cancer population. 30 It is easily administered and not too time-consuming, thus reducing burden on participants. This assessment consists of 14 tests which measure different areas of an individual’s balance, including anticipatory postural adjustments, reactive postural control, sensory orientation and dynamic gait.
Following this initial assessment, participants took part in a 10-week circuit training program, once per week, run by a local non-profit charity organisation. The individual delivering the circuit training sessions was a personal trainer qualified in exercise prescription, strength and conditioning and cancer rehabilitation. A variety of strengthening (e.g. wall press up and sit to stand), cardio (e.g. marching on the spot and step ups) and balancing (e.g. unipedal stance) exercises were included in the program, with a range of difficulties available for differing abilities in the group. The first week began with 10 exercises (stations), with participants completing 30 seconds per exercise and a 10 second rest whilst they switched stations. Upon completion of a circuit, participants were given a two to three-minute rest, before completing the circuit twice more. Each week, exercise duration increased by 5 seconds, whilst time between stations was increased by 5 seconds every 3 weeks. Exercises were changed on a weekly basis to ensure participants remained motivated and engaged, and a range of physical attributes were targeted.
Upon completion of the ten-week program, another study visit to the university laboratory was arranged. Participants completed another FES-I and underwent another Mini-BESTest assessment to determine whether there had been any changes in balance and FoF.
Data analysis
Data were analysed using Statistical Package for Social Sciences version 29 (SPSS Inc., Armonk, NY). Normality of data was assessed using the Shapiro-Wilk test. To evaluate differences between the measures of the Mini-BESTest and FES-I between pre- and post-circuit training, a paired samples t-test was used for normally distributed data. For non-normally distributed data, bootstrapping was performed with 1000 samples. 31 The mean difference is presented alongside its 95% confidence intervals (CIs). For non-normally distributed data, bias corrected accelerated (BCa) CIs were used.32,33
Results
Participant demographics (n = 12).
Data are mean (standard deviation) unless stated otherwise.
Participants had a mean (standard deviation (SD)) age of 64.6 (7.0) years and were evenly split regarding sex (50% male). Of the 12 participants who completed the study, six had a diagnosis of breast cancer (50%), four had a diagnosis of prostate cancer (33%), one with spinal cancer (8%) and one with pancreatic cancer (8%). Tumour stages were predominantly stage 4 upon diagnosis, as self-reported by participants (n = 5, 42%).
Following the circuit training program, the overall Mini-BESTest score improved significantly (p = 0.003) compared with the baseline results (Figure 1), rising from 65.2% (22.6%) to 80.4% (17.5%) (mean difference: 15.2%; BCa 95% CI: 10.1% to 20.8%). The total Mini-BESTest score rose by 4.25 points, from 18.25 to 22.5, exceeding the minimal clinically important difference (MCID) of 3.8 points as reported among patients with early subacute stroke.
34
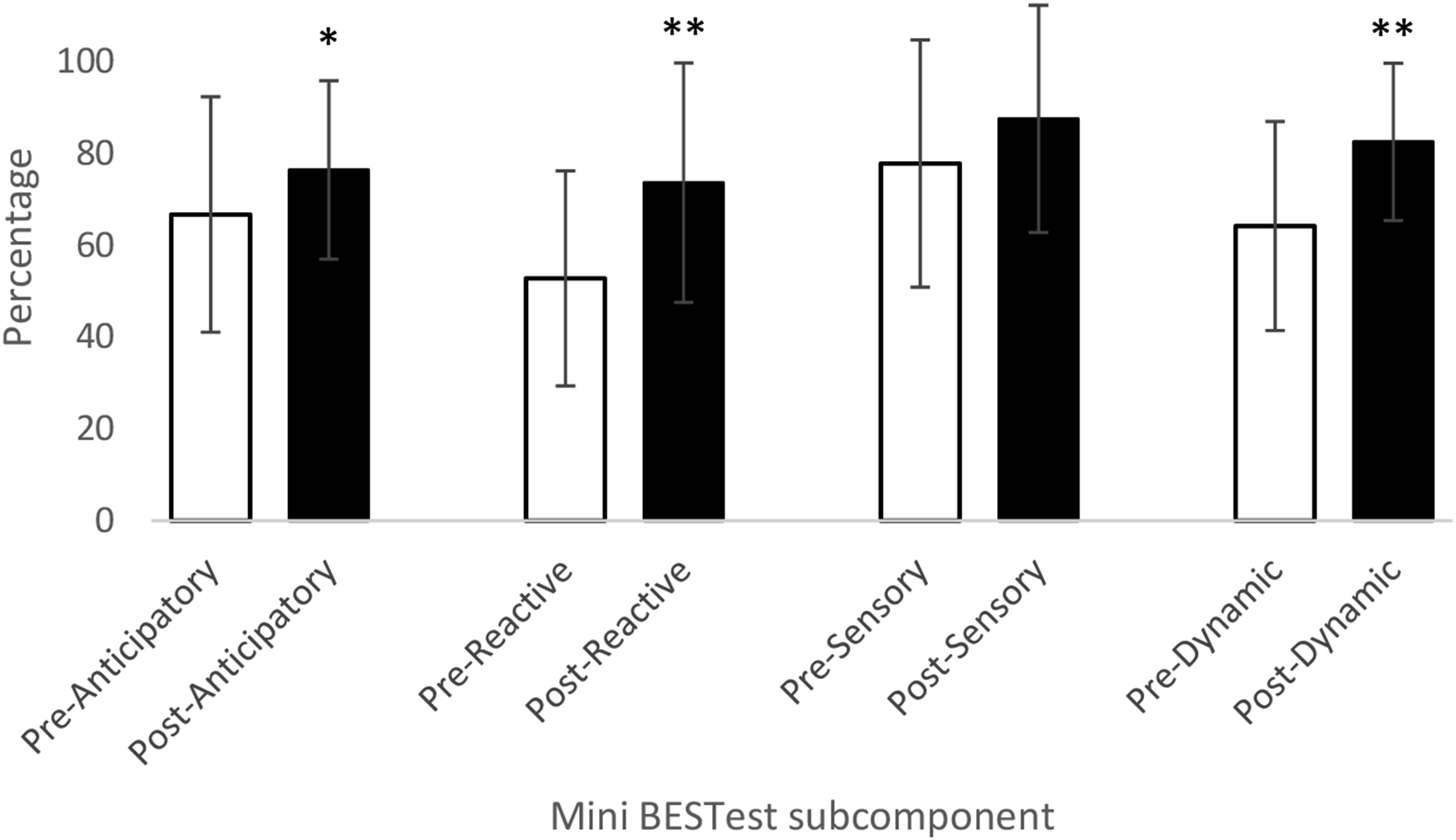
Regarding the Mini-BESTest subcomponents (Figure 2), the Reactive Postural Control subcomponent saw the greatest improvement (p< 0.001) between pre- and post-circuit training (mean difference: 20.8%; 95% CI: 10.6% to 31.1%). Dynamic Gait (mean difference: 18.3%; BCa 95% CI: 13.5% to 23.3%; p< 0.001) and Anticipatory Postural Adjustments (mean difference: 9.7%; 95% CI: 0.2% to 19.3%; p = 0.046) also significantly improved following the 10-week circuit training program. The Sensory Orientation subcomponent was the only non-significant improvement (p = 0.192), with a mean difference of 9.7% (BCa 95% CI: −2.8% to 25.0%). Total Mini-BESTest percentage between pre- and post-circuit training. Note: ** = p< 0.01. Subcomponent total percentages between pre- and post-circuit training. Note: * = p< 0.05; ** = p< 0.01.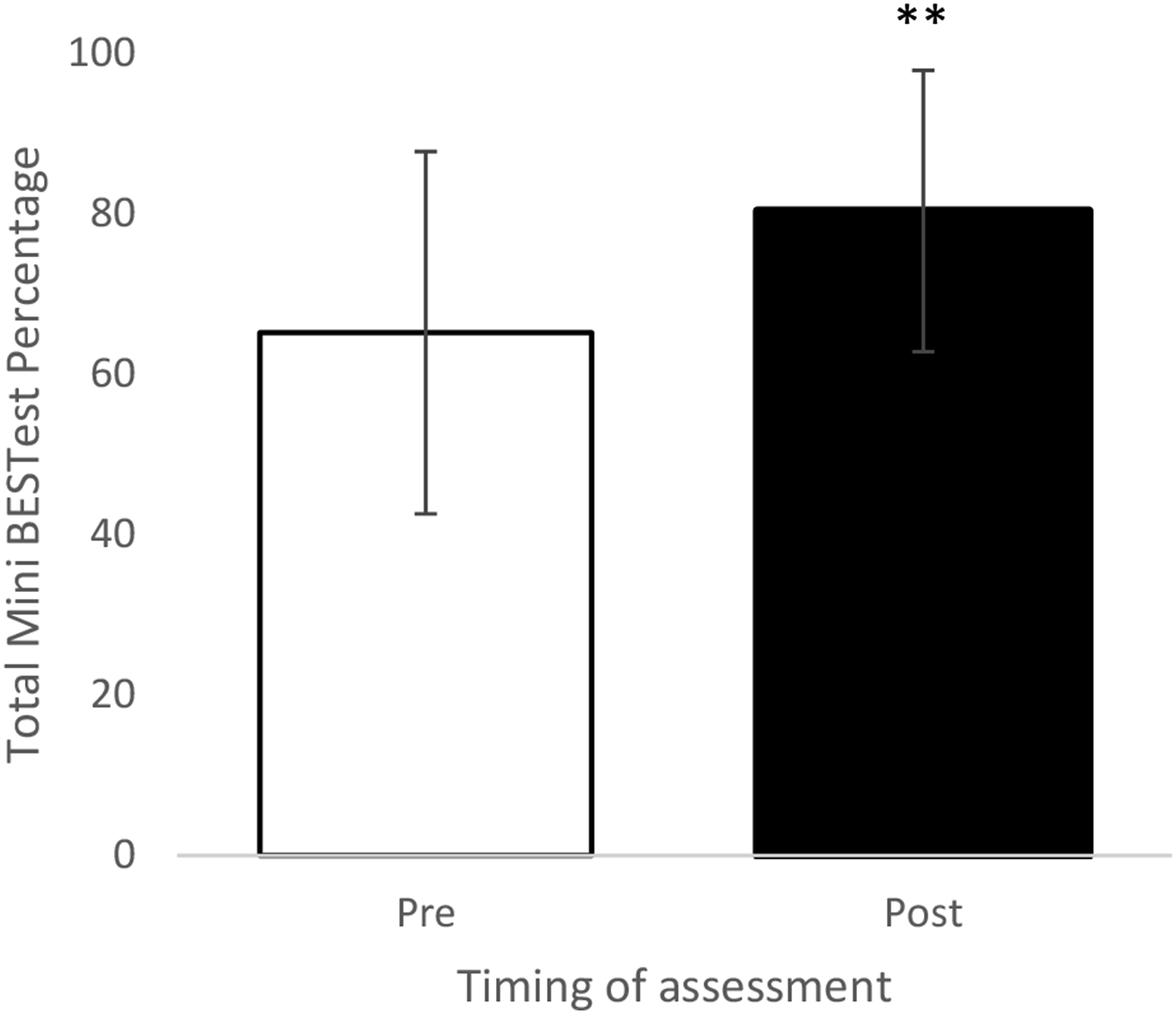
As assessed by the FES-I, FoF significantly decreased (p = 0.026) following the 10-week circuit training program, with a mean difference of −4.8 (BCa 95% CI: −8.1 to −1.9) (Figure 3). Despite the significant improvement, the changes did not meet the MCID as previously reported of between 5.5 and 10.
35
Total FES-I scores between pre- and post-circuit training. Note: * = p<0.05.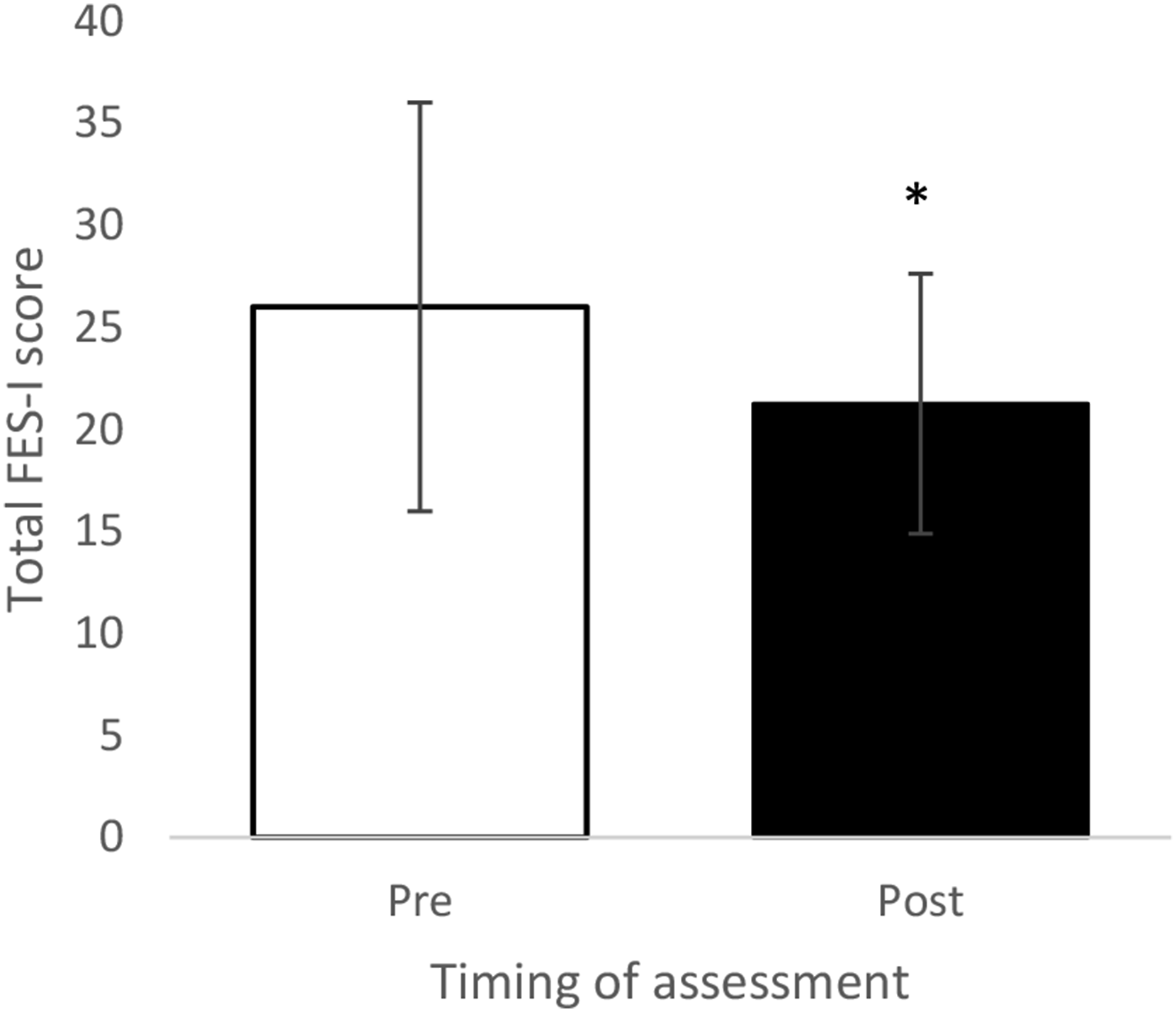
Discussion
The aim of the study was to investigate the effectiveness of a 10-week circuit training program on balance and FoF among individuals with cancer. The hypothesis, that both balance and FoF would be improved following partaking in the circuit-training program, was supported. Significant improvements were found in overall balance (p = 0.003) and three of the four subcomponents of the Mini-BESTest. FoF, assessed using the FES-I, also significantly decreased (p = 0.026).
Research shows that individuals with cancer, whether they have undergone surgery or adjuvant therapies, are more at risk of having impaired balance, thus being predisposed to a greater risk of falling.16–19 Individuals who have received chemotherapy to treat their cancer may also experience chemotherapy induced peripheral neuropathy (CIPN) which further exacerbates FoF and incidence of falls. 36
Exercise, meanwhile, has been shown to be beneficial in an older adult population in eliciting a multitude of health benefits, including improving an individuals’ balance, thus reducing likelihood of falls.23,24 Although research into circuit training in people with cancer is limited, that which is available shows it is effective in improving physical function and muscle mass.26,27 The findings of the current study support previous research, with a significantly improved balance after the 10-week circuit training program. Further to this, all subcomponents of the Mini-BESTest improved, three of which significantly (Anticipatory Postural Adjustments, Reactive Postural Control and Dynamic Gait). Gusi et al. 37 found that when an individual has a greater balance and postural stability, they have a lower FoF. Participants in the current study reported a significantly lower FoF following the circuit training program compared to baseline measures.
This increased confidence, along with improved postural control, will help to reduce incidence and prevalence of falls in people with cancer. Currently, however, exercise interventions or programs are not routinely offered upon receiving a diagnosis of cancer within the United Kingdom. This is something that should be considered as part of routine care for people with cancer, to ensure that they can reduce their risk of falling, improve or maintain physical functioning, and continue with their usual daily activities. In doing so, time and cost to healthcare organisations can be reduced, whilst quality of life can be improved for those diagnosed with cancer.
Limitations and future research
Despite the positive findings of the study, several limitations existed. The small sample size may make it hard to generalise the findings to the wider population of people with cancer; however, the confidence intervals suggest it is likely that these results would be seen regardless. Those within this study were also recruited through a self-referral scheme, indicating that they were already keen on partaking in exercise, which may have impacted the findings. This study also included participants with a variety of cancer types at differing stages, as well as those who had and had not undergone surgery and further treatments. Future research should aim to investigate whether an exercise program of this nature would be suitable and effective for all individuals with cancer. It would also be relevant to explore whether a circuit training program could be implemented over a longer period, as well as how to ensure adherence to the program, particularly during further treatments.
Conclusion
A 10-week circuit training program was effective in improving balance and reducing FoF among adults with cancer. While the results suggest the potential benefits, further research is needed to confirm the generalisability of the findings. Healthcare providers should consider implementing or referring patients to exercise programs upon a diagnosis of cancer as part of their routine care, as this could improve physical functioning, reduce FoF and potentially lower fall risk. Future research should also explore the most effective method of exercise to maximise benefits and assess applicability to all cancer types and individual circumstances.
Footnotes
Acknowledgements
The author would like to express their appreciation to Alice Carter of Lincoln City Foundation who helped to contextualise the study and led the recruitment of participants from the Fighting Fit program. A special thank you is also given to the instructors of the Fighting Fit program, as well as the participants for their time and commitment to the study.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.