
Abstract

Introduction
The problems facing the clinical laboratories at St Thomas' Hospital in London are no different from those facing any other public sector laboratory, how to manage the widening gap between the supply of scarce resources and the demand to cope with the workload and the need to continually tailor the service to the end-user's specific needs. However, the laboratories are different from others in the UK because change was forced upon them due to the merger of Guy's Hospital (figure 1), and St Thomas' Hospital (figure 2), both recognised as major ‘centres of excellence’ with long established reputations in Pathology. This created the need to re-engineer virtually every process within the new organisation - Guy's and St Thomas' NHS Trust, - giving the opportunity to consider automating those functions where there were possible economies of scale and improved service delivery resulting from better queue management of samples and data.
Guy's Hospital

St Thomas' Hospital
In common with many hospitals in the UK, consideration was given to the integration of the routine chemistry and haematology laboratories to form a core automated laboratory. However, this proposal did not demonstrate any significant benefit because there was little in common between the laboratories other than the fact that they both used automated analysers. The samples, once received proceed to separate and independent work processing queues. This, along with several other factors prompted a study of the areas of similarity between laboratory disciplines and to consider these for rationalisation. The study was conducted recognising that each laboratory section was bound by the professional management of its own ‘sphere of excellence’. To change this too quickly could destroy the basis of Pathology which has evolved over the last 100 years in both hospitals.
The Business Case for Automation
An analysis of workload and workflow indicated that the daily number of serum/plasma samples for chemistry, virology or immunology analyses, was approximately 3,000 with approximately 2,000 samples for haematology. Of these, 93% are received between 9.00 am and 5:00 pm, creating significant peaks of activity often associated with delay due to the backlog of work in the specimen reception and preparation areas of the laboratories.
For historical reasons each laboratory handled its own pre- and post-analytical functions, giving rise to multiple service delivery points. For example, there were nine specimen reception points, all of which were involved with data logging and handling telephone enquiries. Five of these areas were also involved with serum separation and aliquoting of blood samples. None of these areas was operating efficiently or effectively because none had sufficient staff to cope with peak demand. However, it was estimated that there were at least 35 members of staff involved in these functions. This represented approximately 23% of the staff involved with all aspects of sample and data processing. However, because no single service point had a critical mass of staff to cope with peak workload there were inevitable sources of delay to workflow, causing impairment of the service to the end-user. This was a clear indication that there could be economies of scale and concomitant improved delivery of service if some of these functions could be automated.
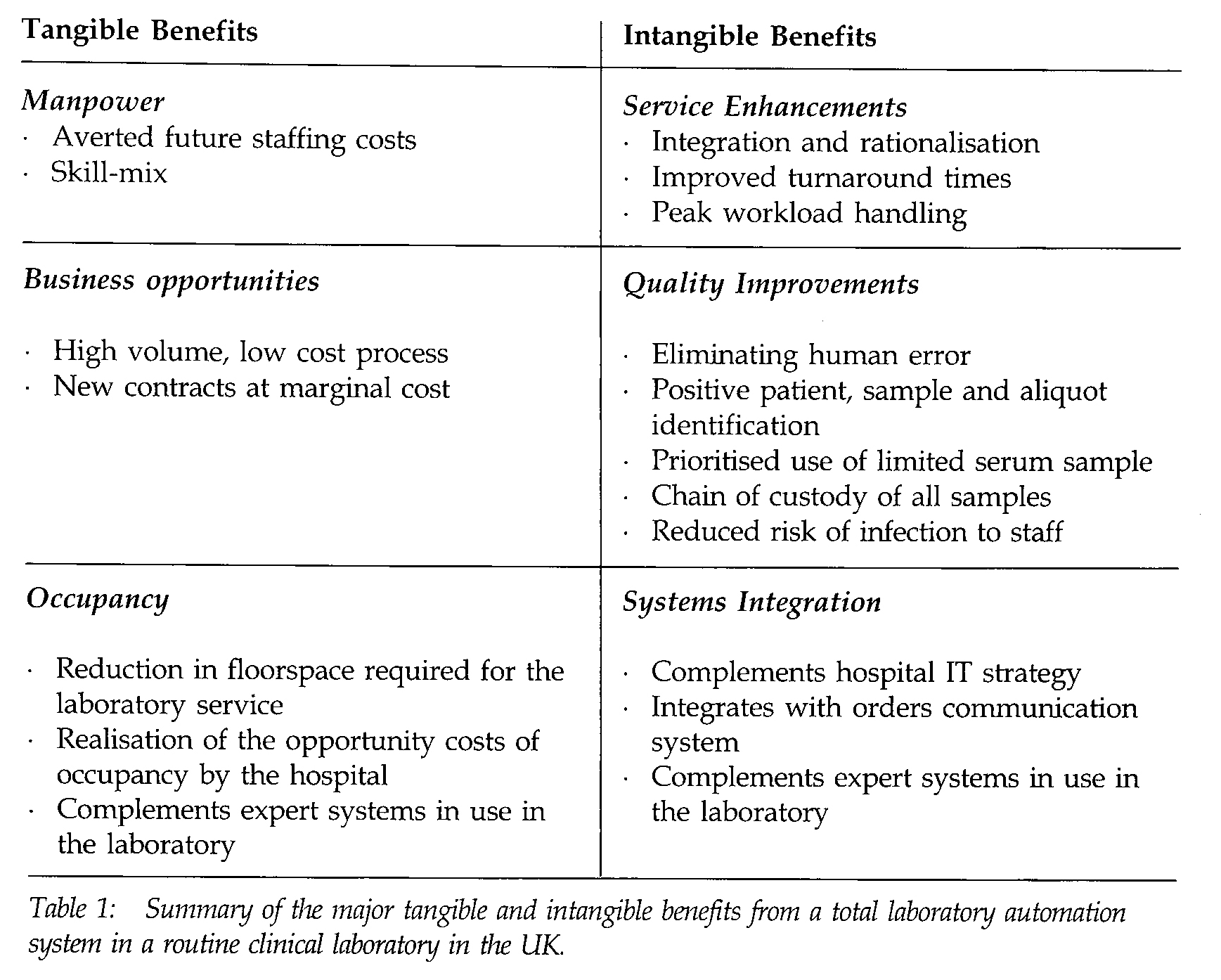
Automation should never be considered as an end-product in itself; it is merely a means of embodying skills and knowledge in an electromechanical system to reduce costs and improve quality of output and delivery of service. Although a decision to automate must be based on the risk of capital relative to the averted cost of future expenditure, the tangible benefits, attention must also be given to other benefits, some of which are non-pecuniary and are intangible. These are summarised in table 1.
Summary of the major tangible and intangible benefits from a total laboratory automation system in a routine clinical laboratory in the UK.
Major targets for automation, and common to most of the points of service, were centrifugation of samples, preparation of serum aliquots and loading and unloading of analysers because of the highly repetitive nature of the tasks. Although they do not require great technical skill or knowledge, they are highly dependent upon manpower and are seen as potential sources of error and delay. The decision was therefore taken to embark upon a project which would reduce the delay and errors associated with sample handling by installing an automated blood sample processor and transport system. However, since there was no empirical evidence from Western laboratories to indicate the magnitude of the revenue savings possible, a financial risk assessment was undertaken to establish the business case to support the capital expenditure. To assess the risk to the organisation, the capital cost of the total system and its components were compared with the predicted staff savings for each element of functionality covered by the automated equipment. This demonstrated that investment in an automated centrifugation and serum separation system was a low financial risk with a relatively short payback period, but that there was a much higher degree of financial risk to progress through the various stages to total automation. The principle reason for this was that the capital cost of the sample tracking systems and robotic interfaces to link the automated blood sample processor (ABSP) to the current generation of analysers used in clinical chemistry, serology, endocrinology and haematology at Guy's and St Thomas' Hospital would be significantly greater than the predicted reduction in staff cost over the life of the equipment.
It is, however, anticipated that as instrument manufacturers become more aware of the potential move to such systems, the next generation of analysers will be able to be mechanically interfaced at less cost. This should enable the totally automated laboratory to be developed over a number of years. For this reason the decision to proceed in three distinct phases was adopted.
The first stage of the project was to implement ABSP where samples for serum/plasma analyses could be placed on a conveyor or sample transport lane at the point of service (i.e. order entry workstation) for further processing. A schematic of the ABSP commissioned for Guy's and St Thomas' Hospital is given in figure 3. This system will be supplied by Coulter Corporation (Miami, US). The system will involve centrifugation of the samples and separation of the serum/plasma into labelled (eye and bar-code) aliquot tubes. The aliquot tubes will be sorted into racks according to the investigations required from each sample. These racks will be removed by laboratory staff at regular intervals and taken for analysis. Those samples requiring only one analysis achievable from the primary tube will be taken out of the processor immediately following centrifugation to avoid unnecessary delay in having to pass through the serum aliquot station.
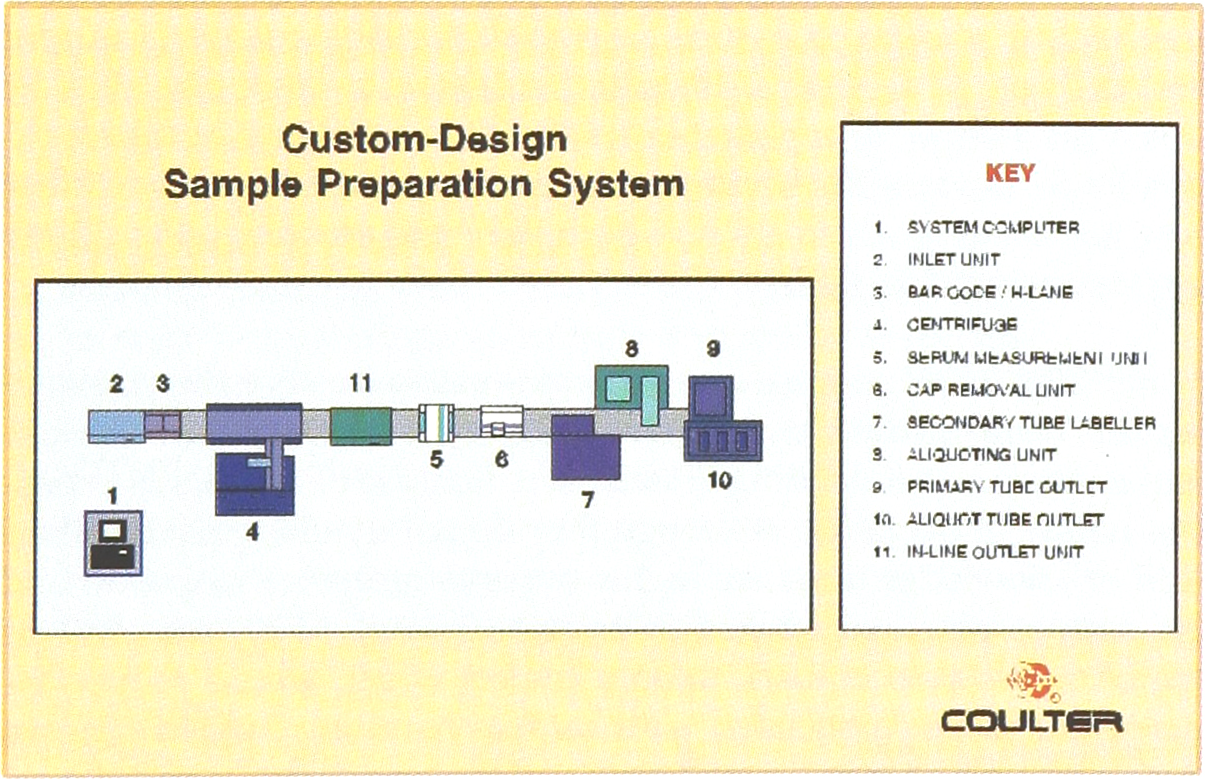
Schematic of the ABSP commissioned for Guy's and St Thomas' Hospital (Coulter Corporation, Miami, FL, US).
The second phase of the project will involve transporting serum/plasma samples (primary and/or secondary tubes) and loading and unloading these on to laboratory instruments. This would encompass the principal instruments used in the clinical chemistry, endocrinology and serology sections of the laboratory. The third phase of the project would expand the scope of the automated laboratory to include loading and unloading the EDTA samples for CBC analysis. However, the decision to proceed with phases 2 and 3 will be bound by the risk to capital, which in turn is linked to the cost of the robotic interfaces to the analysers.
Postscript: Progress Report
To date, Phase 1 of the project has been commissioned, part of the laboratory is being refurbished, the orders communication interface is being developed, the staff are being trained, the multi-disciplinary culture is beginning to change, and I, as the project manager, am keeping my fingers crossed. The predicted ‘go-live’ date for the ABPS is January 1998. This may be the start of the most significant change in the Pathology laboratories at Guy's and St Thomas' Hospital for the last 100 years.