
Abstract
Hitachi and Sysmex corporations combined their efforts to produce an integrated, high through-put laboratory by combining various sections of hematology and chemistry requiring a small fraction of the number of personnel employed.
Osaka City University hospital laboratory exemplifies one type of total laboratory automation that many large medical centers currently strive for. Here, Hitachi and Sysmex corporations combined their efforts to produce an integrated, high through-put laboratory by combining various sections of hematology and chemistry requiring a small fraction of the number of personnel we currently employ.
However, constraints of space and money, the ownership of a large number of fairly new instruments and different service requirements make the installation of such a laboratory as yet unattainable for most centers. For such centers a modular approach to laboratory automation with a future plan for total integration is a reasonable way to proceed. This is what we have attempted in our centralized hematology laboratory.
Historical Background
The Detroit Medical Center - Wayne State University Medical School complex is located in the heart of the city of Detroit. There are five campus hospitals and two off-site hospitals. It also includes a major oncology and transplant center for bone marrow and kidneys. In addition, there are numerous clinics and doctors' offices scattered over a three county area. In 1988 consolidation of the laboratories was achieved with a commercial managing partner, Damon Clinical Laboratories. 1 A core laboratory was established in one of the laboratories with the most space and a central location (Figure 1). The test consolidation initially included routine hematology, immunology, microbiology, virology, routine and special chemistry, serology and toxicology.
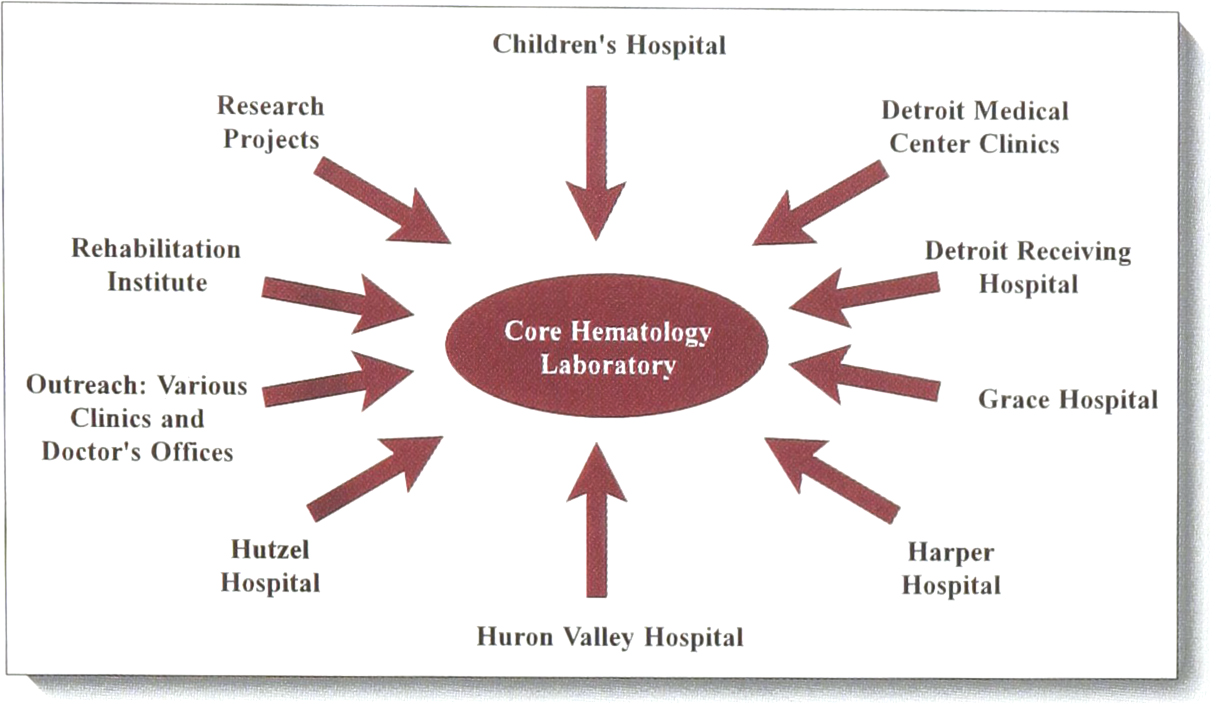
Core hematology and tributaries
Each campus hospital retained STAT laboratories for hematology and chemistry, blood bank and anatomic pathology. Later, specialized laboratories such as cytogenetics, HLA - immunogenetics, special coagulation and flow cytometry were transferred from the medical school. The five campus hospitals were connected by an underground pneumatic tube system with connections to the processing areas as well as direct connections to the core hematology and chemistry laboratories. Thus our Core Hematology Laboratory can receive from and send samples to the campus hospitals as well as our central processing area. The laboratory information system (LIS) consisted of Sunquest for the hospitals and Labnet and later Antrim for the commercial venture.
The first few years were very difficult. Until September 1993 we were using two Sysmex NE-8000 hematology analyzers, performing manual reticulocyte counts and sending all of our special coagulation studies to a reference laboratory in our School of Medicine. The laboratory was crowded, noisy, and labor intensive. Because of the large number of special coagulation tests sent to the medical school laboratory, it was also expensive.
Beginning of More Complete Automation
In September of 1993 we got relief. We purchased a Sysmex Hematology Workstation, HS-302, and put our existing NE-8000 analyzers on line. We kept the reticulocyte counter as a separate station because of the large number of pediatric samples.
We cleared out 1/3 of the laboratory to house this station. Within one week we were fully operational and were gratified by the sudden change in the tone of the laboratory from cramped, noisy and hectic to more spacious, quiet and relaxed (Figure 2).
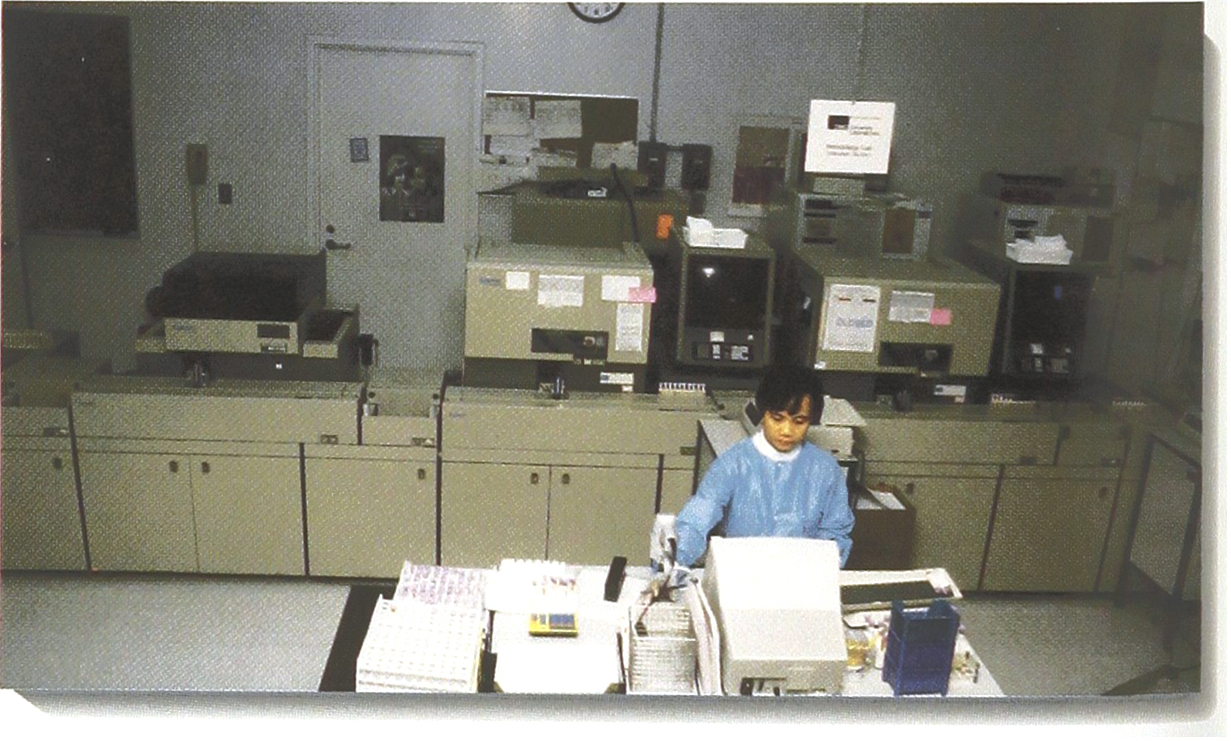
Our Sysmex workstation with a single technologist.
At this time we transferred the special coagulation reference laboratory from the medical school into our laboratory and transferred two medical technologists from the day shift into this newly created section. This produced considerable revenue both by not having to send samples out and also by performing all commercial reference work in house. The benefits of the workstation on the afternoon and night shift were the release of a technologist per shift from the analyzer to complete all the commercial and hospital work. Previously stacks of differentials and urines would be waiting for the morning shift as the commercial volume increased steadily (Figure 3). We further conserved 1.5 medical laboratory assistants FTE from the system by transferring all coagulation specimen processing into core hematology without adding personnel.
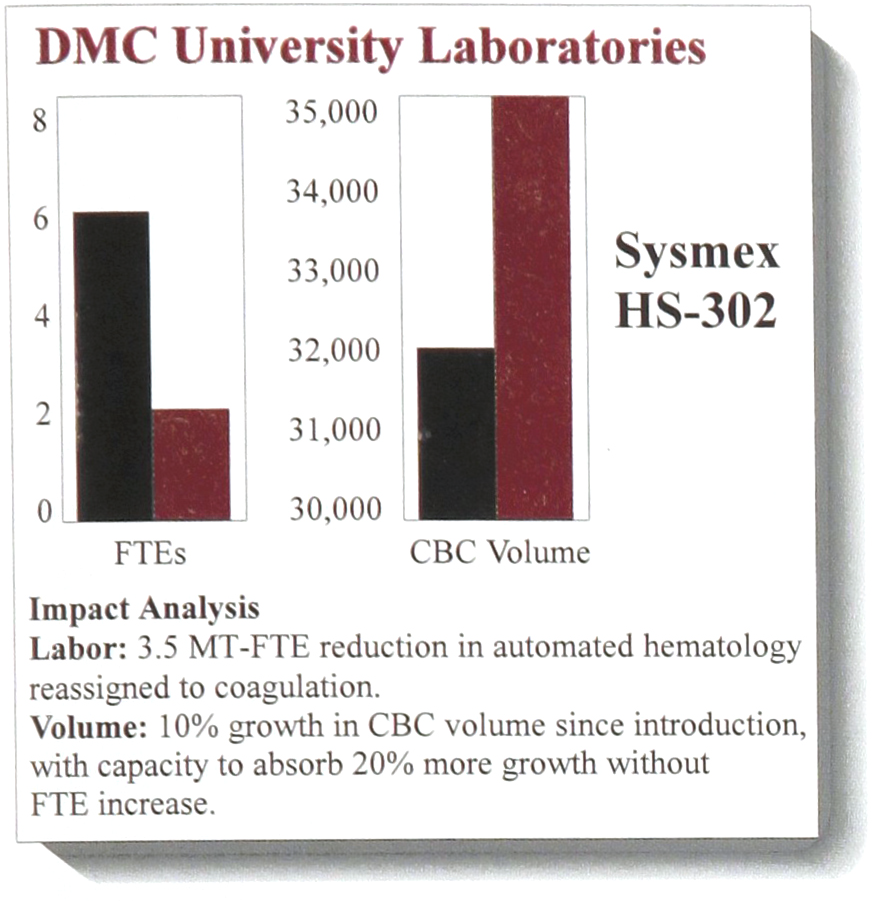
Partial labor savings in 1995. Number of CBC has since increased.
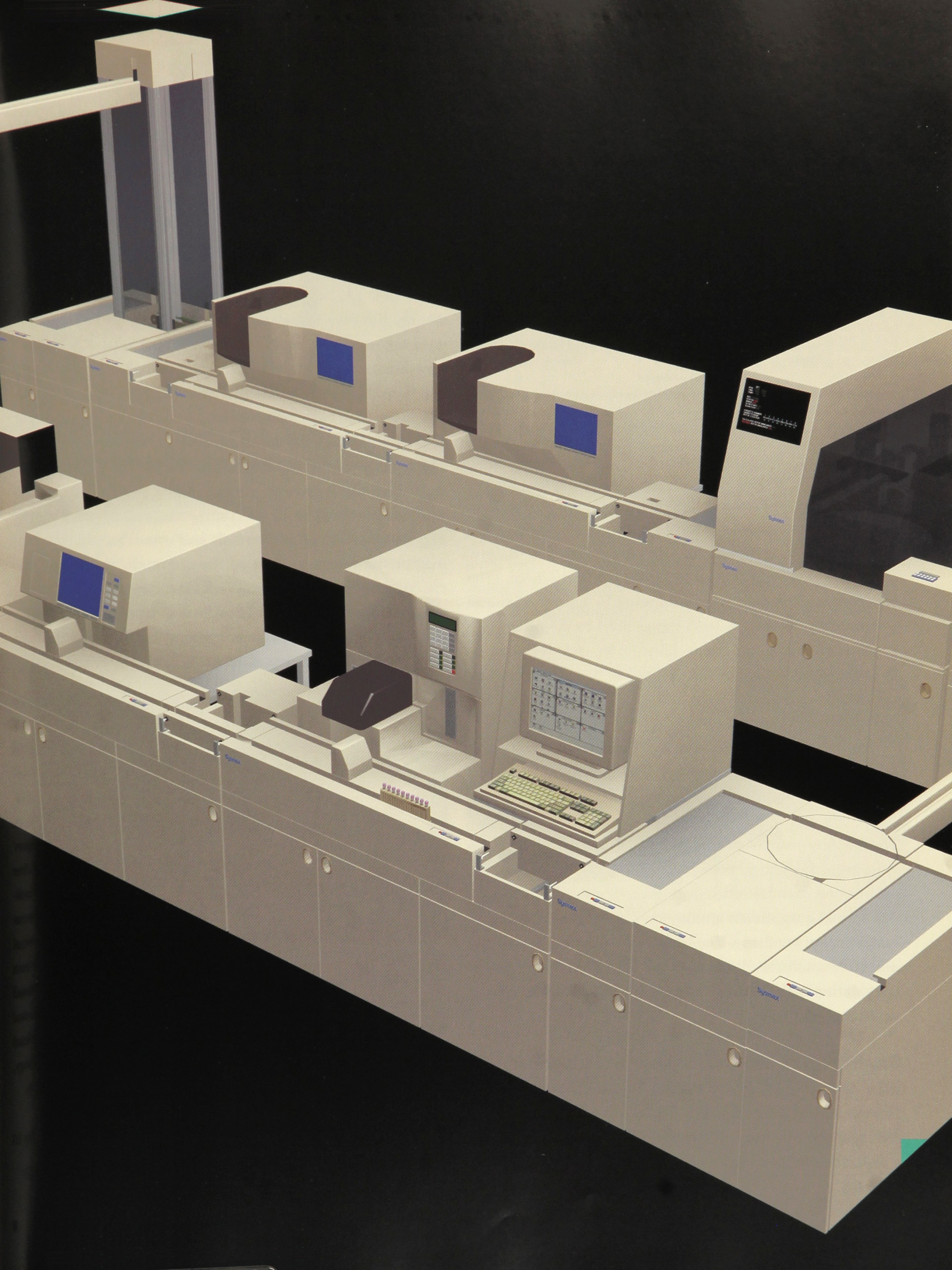
Previously, we needed 2.5 FTEs to constantly work at the two NE-8000 during peak hours. An additional person performed reticulocyte counts. It now only requires one technologist to put 1–20 racks holding 10 tubes into the loading area and to press the starter button and then either attend to other matters in the laboratory, add STAT samples or review the printouts as they come off the instrument (Figure 4). Our walkaway system consists of a system controller, a loading dock for 20 racks of tubes, two conveyor tracks, bar code verification station, robotic mixer, tube piercer and aspirator, two analyzers, slide preparer (SP-1) and tube storage area. The slides are prepared in an enclosed area after thorough mixing and bar code verification. The tube cap is pierced and a wedge type blood smear is prepared, an ID is applied and the slides are dried and stacked into staining baskets.
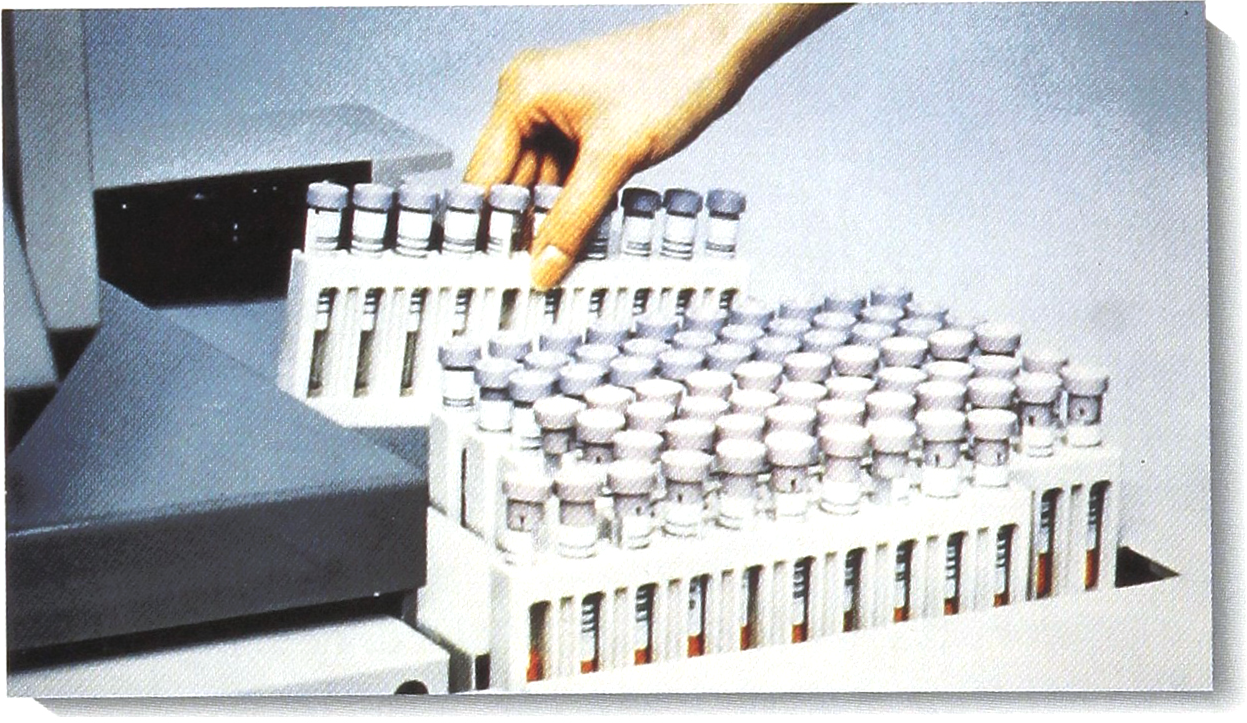
Beginning of automated process - filling up loading station and pressing a button. Courtesy of Sysmex Corporation.
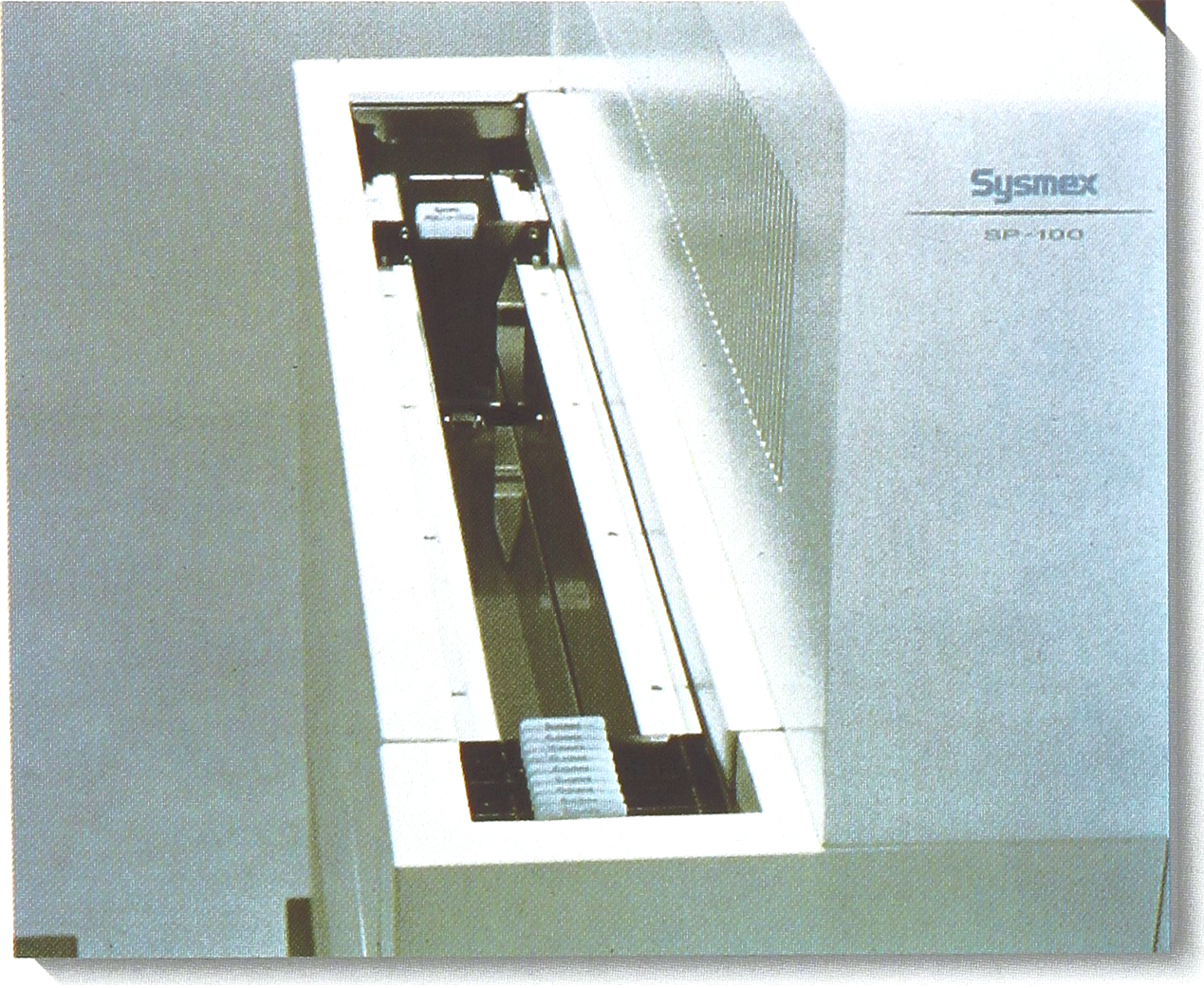
This automation came at a most critical time. At the end of 1992 the partnership with Damon Laboratories was dissolved and DMC University Laboratories was established. After a two year non-compete clause, the commercial outreach volume increased significantly. By 1995 the Outreach volume had increased from 580,604 tests in 1993 to 873,411 tests per year. Our volume on the night shift was now as high as on the day and afternoon shifts put together. However, we did not have to add any FTEs to the instrument section of the hematology laboratory and could absorb even more samples. One FTE was finally added to the night shift to absorb the greatly increased load of urine samples and differentials. Table 1 represents a recent representative monthly census
Monthly Census
We are currently operating this 7 day, 24 hour laboratory with 22.8 medical technologist FTE and 6 medical laboratory assistants FTE. Of these, up to 4 FTEs may be either on vacation, maternity leave, or prolonged and short sick leaves. In addition to the laboratory work we may also be teaching as many as 6 medical technology students, 2–3 pathology residents, medical students and locating samples and slides for internists and their entourage. We also serve as beta sites for new instrumentation.
Further Automation
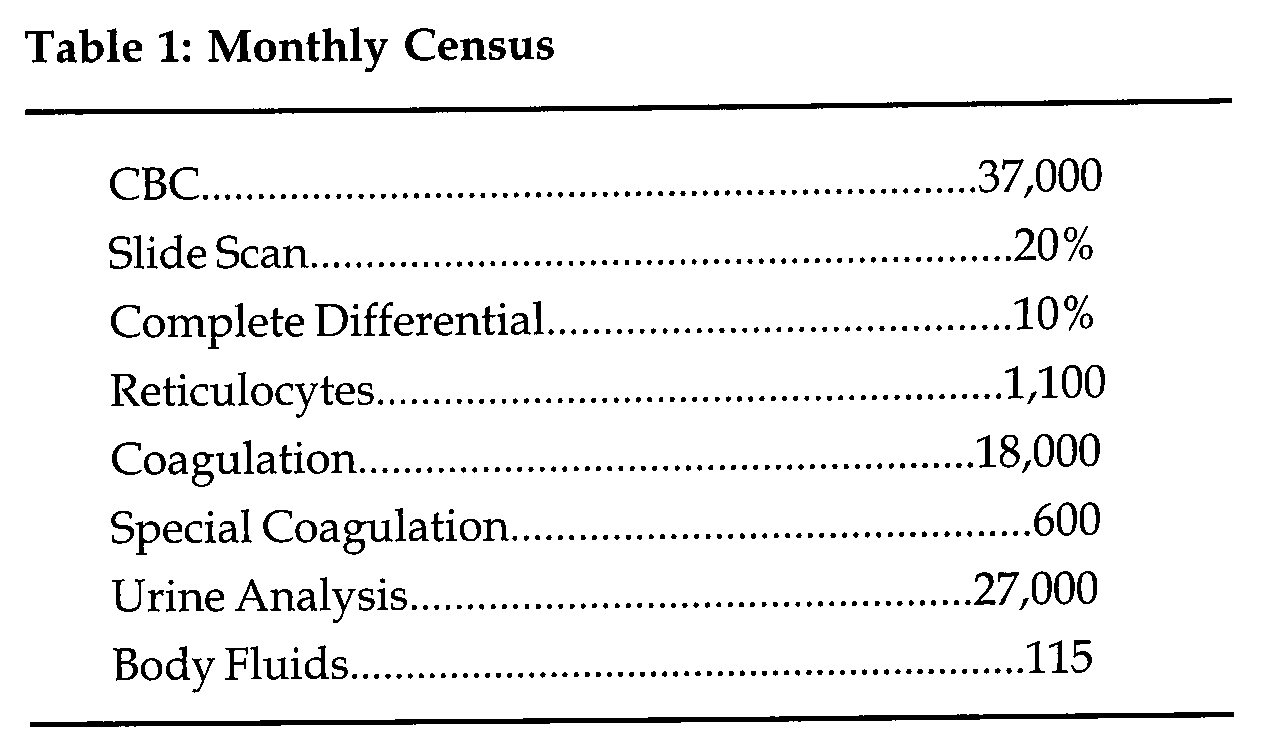
We now want to complete our hematology workstation by adding a new slide maker-slide stainer module, SP-100, (Figure 5) and replacing the NE-8000 with SE-9000. The latter analyzer provides a choice of different test menus. We would further like to expand this work station by having the stained slides of blood samples, which are flagged by the analyzer, go directly to an automated differential counter with viewing screen and/or to a flow cytometer which would define granulocyte precursors, atypical lymphocytes and phenotype leukemic cells.
End of automated process. Racks of stained and labeled blood smears ready for the microscope. Courtesy of Sysmex Corporation.
Total Hematology Automation and Specimen Delivery to the Laboratory
The next logical step, of course, is to create similar automated workstations for coagulation and urine analysis. Few complete urine analysis stations are available at this time. The yellow IRIS is introducing an almost walk-away system where dipstick reader trays are manually transferred to the microscopic reader. But the microscopic portion is still an interactive process for the technologist. We are presently a beta site for another urine analyzer by Sysmex which eliminates the interactive process and identifies the urinary sediment by other parameters. It resembles the hematology analyzer by using test tubes in the same loading racks (Figure 6). There are several complete coagulation systems. At this point we are interested in what type of tube carrier is used and how it would fit into a completely automated hematology laboratory.
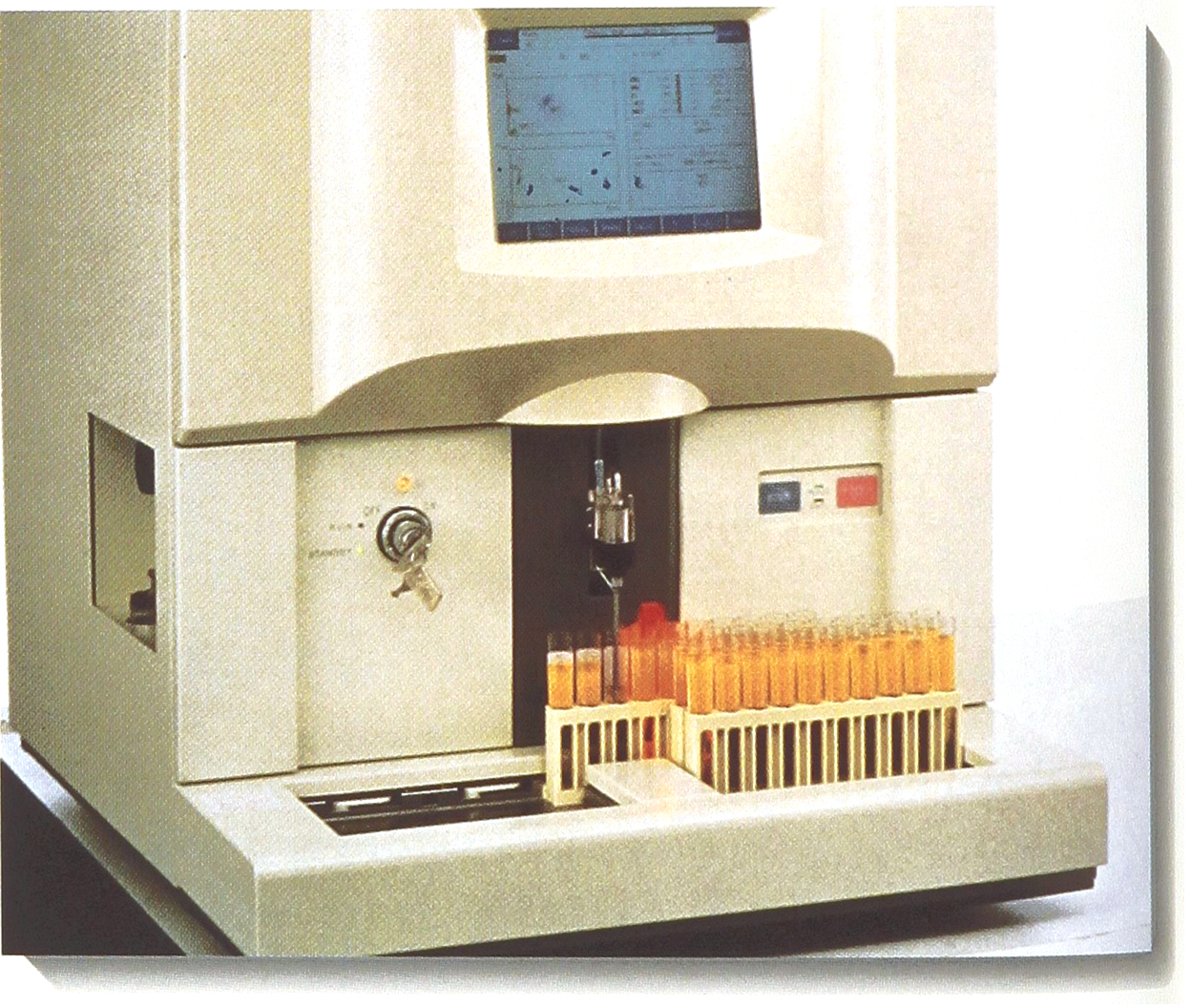
Sysmex urine analyzer. Note specimen holders. Courtesy of Sysmex Corporation
Specimen delivery at the present time is through the pneumatic tube with specimens enclosed in plastic bags. The tubes have to be loaded into the specimen racks by hand. We have explored the possibility of having up-front automated specimen processing in our central specimen processing area. Vendors supplying such up-front automation are Autolab (division of Automed), Coulter - IDS, Hitachi and Labotix. A special feature of Autolab, which shows promise, is the specimen transport containers (STC) which consists of snap-together plastic tube holders which can be single, in long racks of singles or in 5×5 packs.
These STCs fit the conveyor tracks of the Sysmex workstations thus raising the possibility of adapting a direct delivery system from the specimen processing station to hematology, urine and coagulation analyzers (Figure 7). The next step would then be obvious: connecting these three major work islands with conveyor tracks. This has been accomplished by Sysmex in collaboration with Labotix (Figure 8).
One type of specimen transport container. Autolab's STC might be adapted to Sysmex conveyor tracks.

Sysmex in collaboration with Labotix, has been able to onnect major work islands with conveyor tracks.
The labor savings in such a hematology laboratory will be substantial. During peak times one technologist would be at each of the three major work stations. Two would perform differential counts or one could work with a differential counter using artificial intelligence or a flow cytometer. As these differential counters become more proficient they could also perform bone marrow and other body fluid differentials.
High Through-put Laboratories
Larger space could be created in a laboratory such as ours to establish a high throughput laboratory by knocking down walls joining hematology, chemistry, and immunochemistry.
Factors to be considered are:
The cost of rebuilding the laboratory
The cost of interfacing a large number of different instruments
The number of specimens needing technologists attention
Emerging new technologies, such as nanotechnology
These factors should be weighed against the cost of creating:
Flexible modules of automation in specimen processing and various sections of the laboratory
Flexible delivery systems, whether pneumatic tubes or conveyor tracks
A flexible, responsive laboratory system in tune with the laboratory.
Footnotes
Acknowledgements
The authors gratefully acknowledge Mrs. Tracey Wolfe's secretarial and graphics assistance.