
Abstract
Laminoplasty is a common surgical procedure in our daily practice as a way for posterior decompression by expanding the spinal canal, for example in patients with cervical myelopathy. There are primarily two mainstays of laminoplasty, that is, single-door (open-door) and double-door (French-door) laminoplasty. Single-door laminoplasty was initially developed by Hirabayashi in which an asymmetrical canal opening was created on one side and hinged on the other. In contrast, the double-door technique was first described by Kurokawa, in which a symmetrical canal opening was created in the midline with hydroxyapatite block spacers in between the opened laminae hinging on two sides. Both techniques have been performed in our center and are options to provide adequate posterior decompression. We would like to evaluate any potential difference in outcomes between the patients receiving the two techniques of laminoplasty in our center, which may provide insight into future operative planning and practice. During 2018–2022, 40 patients who had received either single-door or double-door laminoplasty were recruited for analysis. This is a retrospective review of clinical and radiological outcomes of patients between the groups of patients receiving single-door and double-door laminoplasty in our local center. Our study showed that single-door and double-door laminoplasty were both effective in neural decompression to allow functional improvement by improving both post-operative Pavlov ratio and modified Japanese Orthopaedic Association scores. Single-door group had significantly shorter operative time, and less blood loss compared to double-door group. Given that single-door laminoplasty is an effective technique with shorter operative time and less blood loss, we concluded that it may be considered as a primary technique in laminoplasty in novice surgeons or in emergency setting.
Introduction
Laminoplasty is a common surgical procedure in our daily practice as a way for posterior decompression by expanding the spinal canal, for example in patients with cervical myelopathy. It was first developed in Japan in the early 1970s. There have been multiple modifications since. 1 There are primarily two mainstays of laminoplasty, that is, single-door (open-door) and double-door (French-door) laminoplasty. Single-door laminoplasty was initially developed by Hirabayashi in which an asymmetrical canal opening was created on one side and hinged on the other. In contrast, the double-door technique was first described by Kurokawa, in which a symmetrical canal opening was created in the midline with hydroxyapatite block spacers in between the opened laminae hinging on two sides.
Both techniques have been performed in our center and are options to provide adequate posterior decompression. We would like to evaluate any potential difference in outcomes between the patients receiving the two techniques of laminoplasty in our center, which may provide insight into future operative planning and practice.
Fourty patients who had received either one of the techniques during 2018 to 2022 were stratified into two different groups, that is, the single-door group and double-door group, for analysis. Their post-operative clinical and radiological outcomes were evaluated and compared.
This is a retrospective review of clinical and radiological outcomes between the patient groups receiving single-door and double-door laminoplasty in our local center.
Methodology
In this retrospective case–control study, 40 consecutive patients treated with single-door or double-door laminoplasty in our center from 2018 to 2022 were recruited. Patients’ demographics including the age and sex were collected. They were divided into two groups based on the different techniques of laminoplasty received. Exclusion criteria adopted included patient(s) who had received previous neck surgery, or previous spinal surgery and/or having a history of old cardiovascular accident.
In our center, the single-door laminoplasty is achieved by using a power burr to create single-door opening by a full-thickness gutter and another partial-thickness one over the laminae. The hinged lamina is fixed with an arch plate. Whereas in the double-door technique, after performing laminotomy over the upper and lower operating levels, the spinous process was split by a Tomita saw tunneled beneath. Subsequently, a power burr is used to create two partial thickness gutters over both laminae of the level, which are fixed with a hydroxyapatite block and suture afterwards. We allocated patients who received laminoplasty with either one of these techniques into two groups, that is, the single-door group and the double-door laminoplasty groups.
Different peri-operative clinical and radiological parameters were collected from the medical records in the Clinical Management System, which were compared between the two groups of patients in the subsequent evaluation. Clinical parameters included the modified JOA (Japanese Orthopaedic Association) score, any presence of neck pain (using visual analogue scale) and C5 palsy. Operative time, intra-operative blood loss and post-operative length of stay were also traced from the record. Radiological assessment included the change in cervical lordosis (by measuring the C2–C7 Cobb angle 2 ) and Pavlov ratio measured at the C4 level; both in pre-operative and post-operative lateral cervical spine radiograph, respectively (Figures 1 and 2).
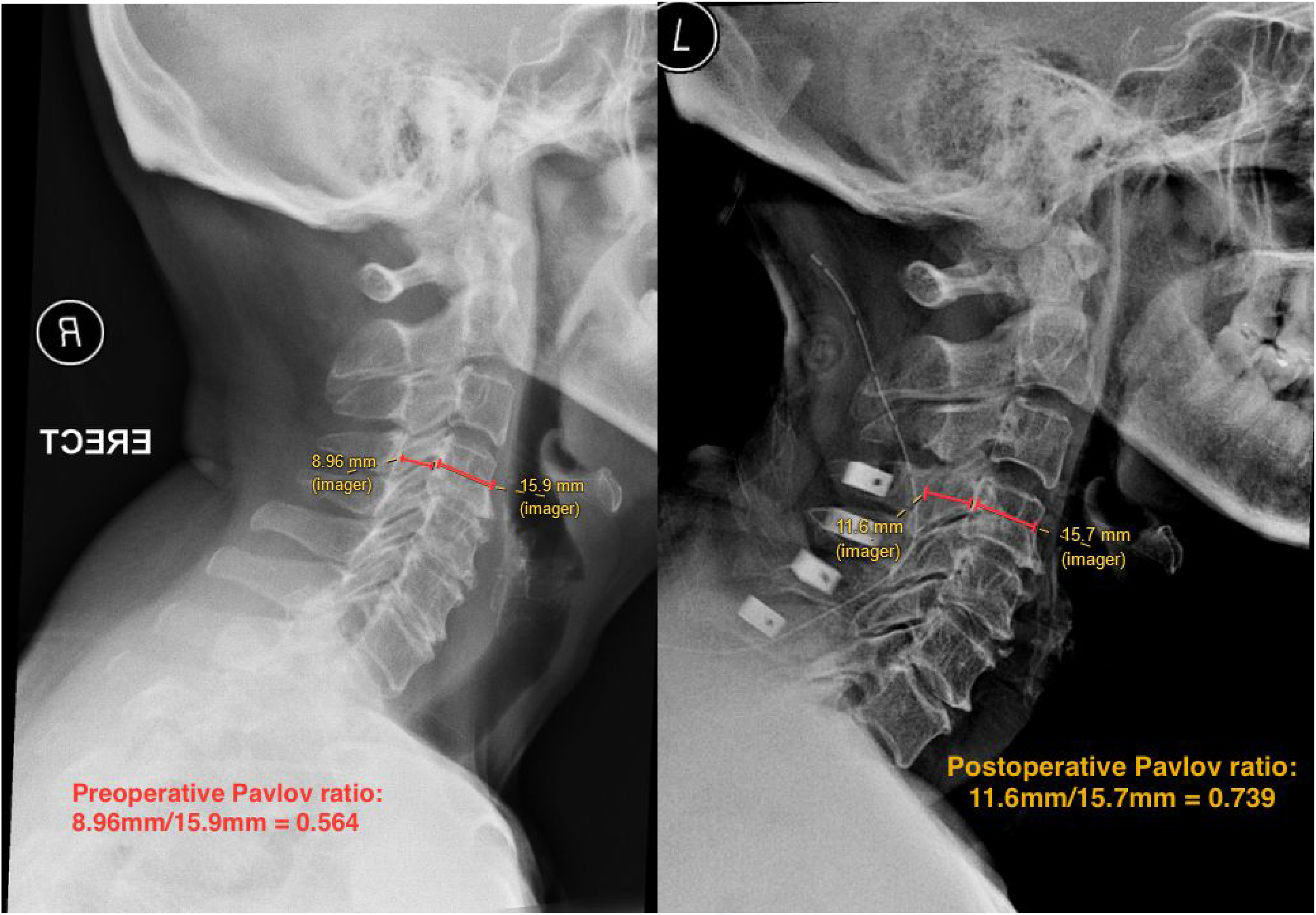
Example of Pavlov ratio measurement. The Pavlov ratio is calculated by dividing the sagittal diameter of spinal canal by the sagittal diameter of vertebral body at the level of C4 in the lateral cervical spine radiograph. In this patient, the pre-operative Pavlov ratio is 0.564 while the post-operative Pavlov ratio is 0.739.
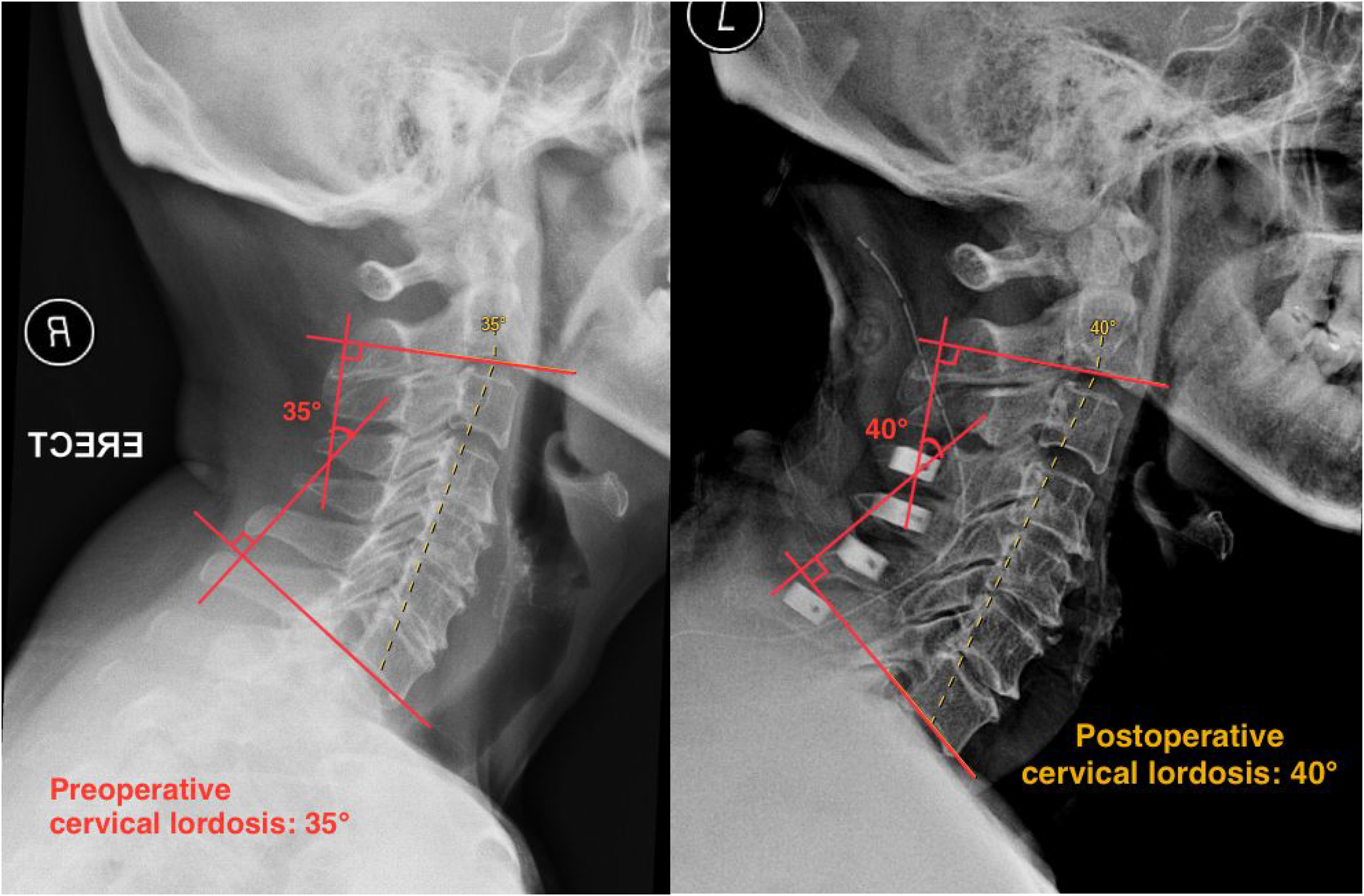
Measurement of cervical spine lordosis using Cobb's method. The cervical lordotic angles are measured by joining perpendiculars to lines drawn parallel to the lower end plates of C2 and C7 in lateral cervical spine radiograph. In this patient, the pre-operative Cobb angle is 35° and post-operative Cobb angle is 40°.
Initial patients’ data were collected as unidentifiable subset from which subsequent statistical calculations were performed using SPSS version 22. p Value of <0.05 was considered significant.
Results
Demographics
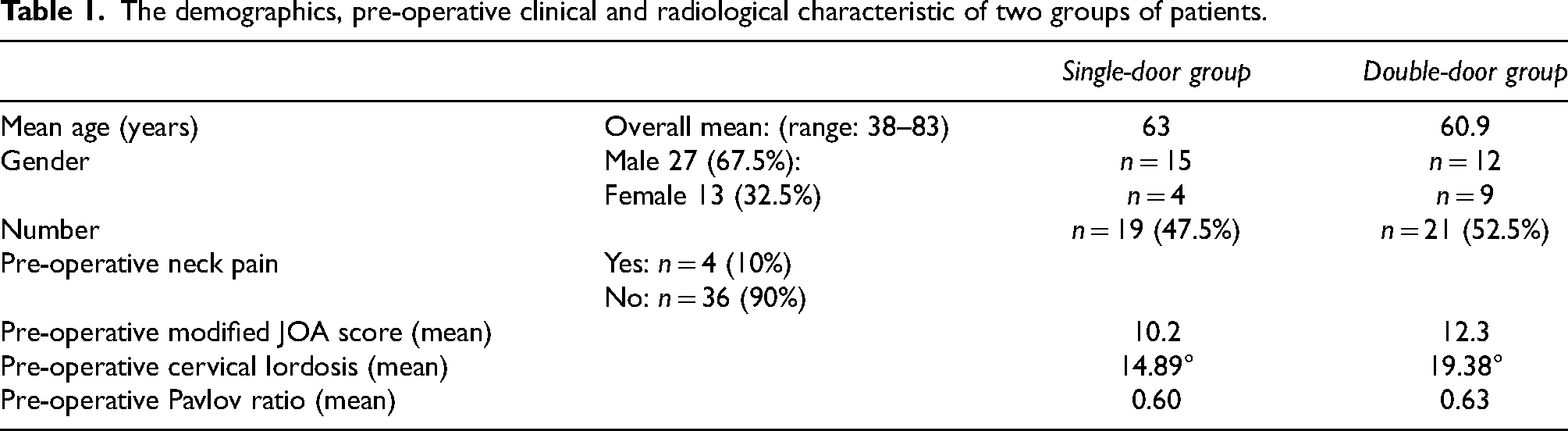
Total 40 patients’ data was collected in this study (Table 1). There were 13 female, 27 male patients recruited; 15 male (78.9%) and 4 female (21.1%) were in the single-door group, while there were 12 male (57.1%) and 9 female (42.9%) in the double-door group. The age ranged from 38 to 83, the mean age was 63 and 60.9 in single-door and double-door groups, respectively. Patient's baseline characteristics in the single-door laminoplasty group were compared with those of the double-door group. There was no statistically significant difference in patient's age (p = 0.515) and sex (p = 0.149).
The demographics, pre-operative clinical and radiological characteristic of two groups of patients.
Pre-operative parameters
The mean pre-operative cervical lordosis in the single-door group was 14.89°, which was lower when compared to the double-door group (19.38°) (p = 0.048) (Table 1). There was no statistical difference in mean pre-operative neck pain (single-door: 1.89 and double-door: 1.90) (p = 0.919). The mean pre-operative Pavlov ratio between both the single-door (0.60) and double-door groups (0.63) also showed no significant difference (p = 0.288). However, the mean pre-operative modified JOA score in the single-door was statistically lower (mJOA score: 10.2) than the double-door groups (mJOA score: 12.3) (p = 0.006).
Functional outcome
The change of modified JOA score at post-operative six months was evaluated (Table 2). The single-door group had mean mJOA increasing from 10.2 to 12.8 (p = 0.013), whereas that of double-door group increased from 12.3 to 14.5 (p = 0.27). Comparing between both groups, the absolute post-operative modified JOA score in the double-door group was significantly higher. Nonetheless, there was no statistically significant difference in terms of recovery rate. The recovery rate for the single-door and double-door groups was 33.3% and 38.6%, respectively (p = 0.28), which was calculated as (post-operative mJOA – pre-operative mJOA) (18 – pre-operative mJOA) × 100%) in both groups.
The functional outcomes in terms of pre and post-operative mJOA score and recovery rate for patients undergoing single-door and double-door laminoplasty.
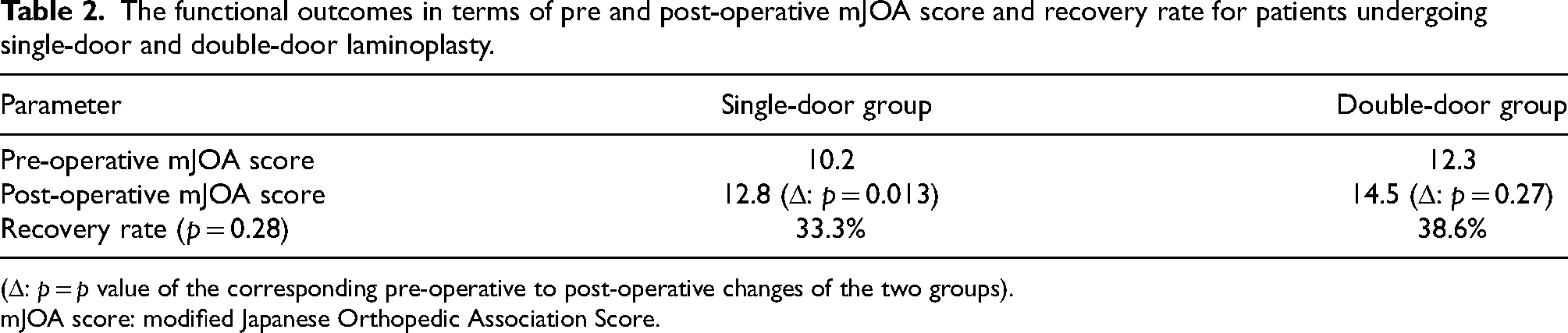
(Δ: p = p value of the corresponding pre-operative to post-operative changes of the two groups).
mJOA score: modified Japanese Orthopedic Association Score.
Radiological outcome
The six-month post-operative Pavlov ratio and cervical lordosis were measured (Table 3). The Pavlov ratio of single-door group had increased from 0.60 to 0.94 (p = 0.041) and that in double-door group had changed from 0.63 to 0.98 (p = 0.004). The percentage change in post-operative Pavlov ratio for the single-door group (56.7%) is higher than double-door group (55.6%) (p = 0.60). There was a slight reduction in post-operative cervical lordosis in both single-door (12.37° (Δ−2.52°)) (p = 0.129) and double-door groups (18.62° (Δ−0.76°)) (p = 0.658).
The changes in radiological outcomes for patients undergoing single-door and double-door laminoplasties.
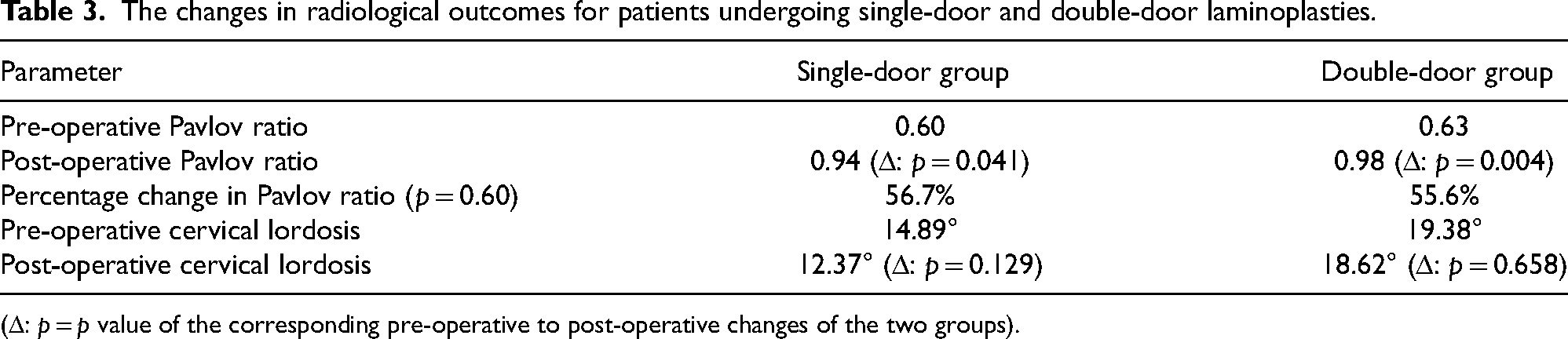
(Δ: p = p value of the corresponding pre-operative to post-operative changes of the two groups).
Operative time & blood loss, C5 palsy and post-operative length of stay
The single-door group has shorter mean operative time and less blood loss (Table 4). The mean operative time in the single-door group was 143 min, which was significantly shorter, compared to 221 min in double-door group (p = 0.00). Intra-operative blood loss in the single-door group (350 ml) is slightly less than double-door group (370 ml) (p = 0.84). There was no significant difference in the occurrence of C5 palsy (p = 0.78). There were four patients, respectively, reported to have C5 palsy in the single-door (21.1%) and double-door groups (19%). The post-operative length of stay in the double-door group was shorter (8.14 days) than single-door group (11.26 days) (p = 0.12).
The changes in operative time, blood loss, C5 palsy occurrence and post-operative length of stay for patients undergoing single-door and double-door laminoplasty.

Discussion
Our study showed that single-door and double-door laminoplasty were both effective in neural decompression to allow functional improvement by improving both post-operative Pavlov ratio and modified JOA scores.
Both groups had shown a significant increase in post-operative Pavlov ratio from about 0.6 to 0.94 and 0.98. The percentage change in the single-door group was higher though there was no significant difference. The single-door group had improved mJOA significantly by 2.6 points. The recovery rate was slightly higher in the double-door group (38.6%) than single-door group (33.3%) but there was no significant difference. Both groups showed reduced cervical lordosis post-operatively.
Both techniques can be considered viable options for treating cervical myelopathy, though they do not provide optimal deformity correction such as increasing cervical lordosis. Heller et al. commented there was no difference in improvement in JOA recovery rate between single- and double-door groups. 3 This was further supported by the similar findings demonstrated in the randomized study by Nakashima et al. 4 The neurological outcome was comparable between both single-door and double-door laminoplasty and both techniques were found to have reduced cervical lordosis and range of motion post-operatively.
Single-door group had significantly shorter operative time, and less blood loss compared to double-door group. There was no difference regarding occurrence of C5 palsy and post-operative length of stay. Longer operative time noted in double-door group may be related to extra steps such as laminotomy and sublaminal T-saw passage required. It is of note that passage of T saw in stenotic canal can be difficult and requires multiple attempts. Single-door laminoplasty is generally more technically feasible as fewer gutters are required.
Some researchers reported that double-door laminoplasty has shorter operative time and less blood loss. The meta-analysis by Ma et al. 5 has concluded that there was no statistical difference found in both the operative time and length of hospital stay between single- and double-door groups. Blood loss was not analysed in that study. These parameters could be confounded by the experience of operating surgeon and complexity of patient's presenting pathology.
Limitations of this study include its retrospective nature, relatively small sample size and possible selection bias. Observational error is possible despite measurements were done by single investigator. Pre-existing comorbidities may affect clinical outcomes.
Given that single-door laminoplasty is an effective technique with shorter operative time and less blood loss, we concluded that it may be considered as a primary technique in laminoplasty in novice surgeons or in emergency settings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.