
Abstract
Background
Implant cut-out is the commonest post-fixation complication of intertrochanteric fractures. It increases socioeconomic and healthcare burdens as well as patient morbidity in its geriatric population. This study identifies cut-out risk factors to prevent its occurrence.
Materials and Methods
This is a retrospective analysis of 203 patients with intertrochanteric fractures treated with a short Proximal Femur Nail Antirotation (PFNA) nail from April 2021 to March 2022 at a major Hong Kong tertiary hospital. Variables studied included gender, age, pre-morbidities, fracture side, fracture type, reduction quality, Tip-Apex Distance (TAD), and Cleveland 9 zones.
Results
The cut-out rate was 2.72%. Significant risk factors included male gender (p = 0.036), chronic kidney disease (p = 0.039), and TAD≥25 mm (p < 0.001). Cut-out likelihood increased 263.53 times with a TAD>25 mm. Patients with good reduction quality had significantly lower cut-out rates (p = 0.018).
Conclusion
Both preoperative and operative variables affect cut-out rates. Optimizing TAD and reduction quality is crucial.
Introduction
Hip fractures, in particular intertrochanteric fractures, are one of the most common geriatric injuries troubling our society today and given current demographic trends, this problem will only become more prominent.1–3 In Hong Kong, fragility hip fractures are forecasted to increase from 6300 cases annually in 2020 to 14500 cases in 2040. 2 The gold standard of treatment remains surgical and the Proximal Femoral Nail Antirotation (PFNA) system is amongst the most accepted fixation method for intertrochanteric fractures; yet it is imperfect.1,3,4 Blade cut-out remains the most frequent reason for implant failure and is defined as the extrusion of the cephalic screw or blade after intramedullary nail fixation of intertrochanteric fractures. 3 Implant cut-out usually requires secondary surgery. However, not only does secondary surgery further increase socioeconomic and healthcare burdens, but a significant portion of this patient group may also be unable to endure such operations based on pre-existing comorbidities.1,3 Thus, the prevention of cut-out, and not its treatment, should be the primary goal.
To successfully prevent implant cut-out, one must identify its risk factors. Multiple studies have identified risk factors which include increased Tip-Apex Distance (TAD), blade position, varus neck shaft angle, fracture type, bone density and reduction quality.1,3–17 Yet, studies either fail to agree on the significance of these risk factors or fail to reach a uniform recommendation. Thus, this retrospective cohort study aims to confirm the risk factors for short PFNA cut-out and to compare local cut-out rates with literature results. To the best of the authors’ knowledge, this is the first study in Hong Kong to analyse local PFNA cut-out rates and related risk factors.
Method
Study design and patient selection
This is a single-centre retrospective cohort analysis of 203 cases with intertrochanteric fractures treated with a short PFNA nail from April of 2021 to March of 2022 at a major tertiary hospital in Hong Kong. Radiographs and hospital records were retrieved from the Hospital Authority CMS system.
Specifically, the inclusion criteria involved 1) adult patients over 18 years old, 2) patients with an intertrochanteric fracture, 3) fracture fixation using the DePuy Synthes short PFNA-II system with blade option (i.e., 170–240 mm PFNA nails), and 4) patients who were followed for a minimum of 3 months post-treatment with X-Ray evaluation of implant status at follow-up.
Meanwhile, the exclusion criteria omitted those with 1) atypical fractures (e.g., cancer-related, prophylactic nailing, other pathological fractures etc.), 2) non-pertrochanteric fractures, 3) same-admission mortality, 4) lost to follow-up, 5) non-short PFNA fracture fixation systems, 6) complications other than cut-out (e.g., infection, periprosthetic fracture, screw back-out etc.) and 7) severe femoral head deformity leading to inaccurate radiographical evaluation. A total of 56 patients were excluded from this study (Figure 1).
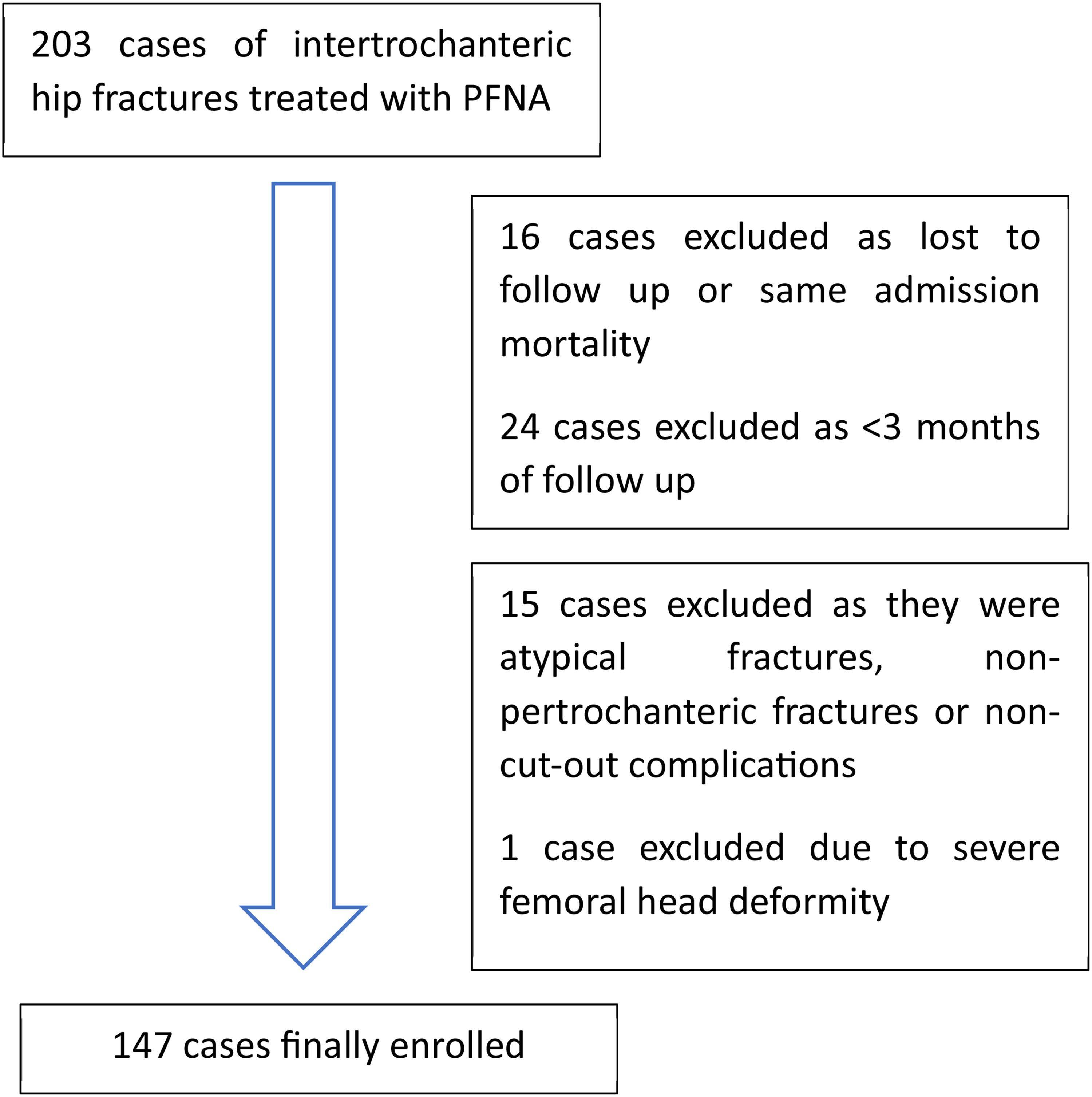
Patient flowchart.
Other patient data collected included patient age, gender, comorbidities (i.e., diabetes and chronic kidney disease), time to latest follow-up and fracture side.
Surgical technique and postoperative rehabilitation
Patients underwent closed reduction and were operated in the supine position on a traction table under fluoroscopic guidance. All cases utilised the standard lateral approach. When reduction was deemed unacceptable by the operating surgeon, adjunctive percutaneous or open reduction techniques were utilised to optimise reduction. The guide wire was inserted at the tip of greater trochanter, followed by reaming of the proximal fragment and insertion of the PFNA respectively. The blade length, intramedullary nail length and nail diameter were determined by the operating surgeon. All cases utilised the proximal femoral nail anti-rotation system (PFNA II) manufactured by Synthes®.
Standard plain radiographs (anteroposterior and lateral views) were obtained on the earliest post-operative day. Patients were allowed full weightbearing after satisfactory alignment was confirmed on the post-operative X-Rays. After discharge, the patients were seen at the out-patient clinic at periods determined by the case doctor based on individual assessment. Radiographs were included in each outpatient clinic visit.
Radiological assessment
Radiological evaluation was performed for both pre-operative and post-operative periods to evaluate for risk factors of implant cut-out. Fracture type was sorted according to the Orthopaedic Trauma Association (AO/OTA) intertrochanteric fracture classification. AO classifications group the fracture types based on stability and complexity with a lower number signifying a simpler fracture. Post-operative radiographs and operative records were evaluated for the presence of cut-out, Tip-Apex Distance (TAD), Cleveland zones and reduction quality. Radiographs were reviewed by a single surgeon.
PFNA blade positioning was assessed by analysing postoperative X-Rays. The TAD was defined as the sum of the distance (mm) measured from the tip of the blade to the femoral head apex measured on an anteroposterior (AP) and lateral radiograph after correction was made for magnification. Radiographic magnification was determined by dividing the known diameter of the lag screw with the measured diameter.1,4,5 Cases were divided into groups with a TAD≤25 mm and those with a TAD>25 mm. The blade position in the femoral head was recorded according to the Cleveland 9 zones (Figure 2–3). 6 Reduction quality was assessed according to the Baumgaertner's criteria which categorises reduction to be good, acceptable or poor. The displacement criteria were defined as a distance of <4 mm between fracture fragments on either the anteroposterior (AP) and lateral (Lat) radiographs. Correct angular reduction was achieved when the neck-shaft angle on the AP radiograph was normal or slightly valgus (125°—150°) and less than 20° of lateral angulation on the lateral radiograph. Reduction was good if both criteria were met, acceptable if only one criterion was met and poor if neither criterion was met.3,5,7
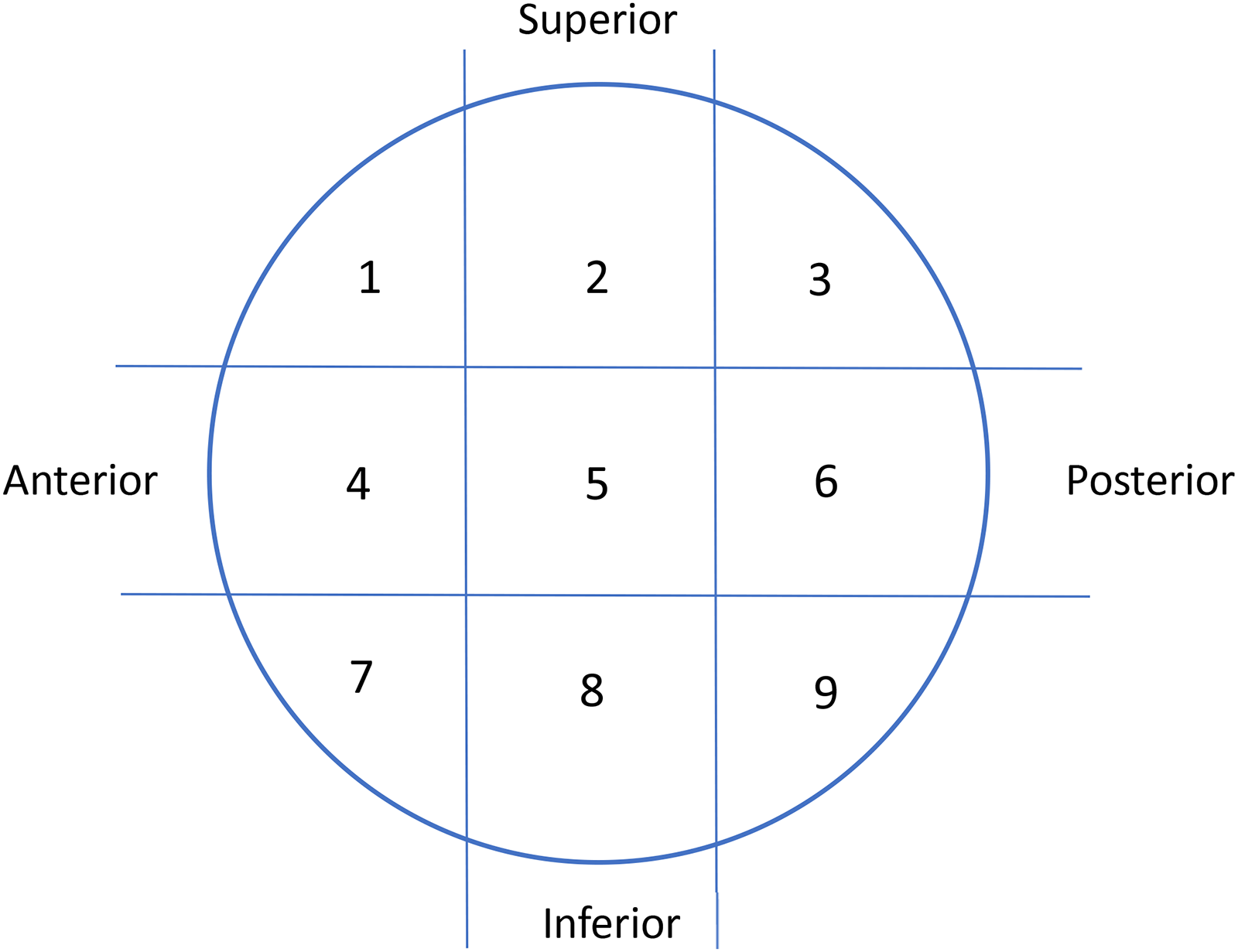
Cleaveland 9 zones of the femoral head.
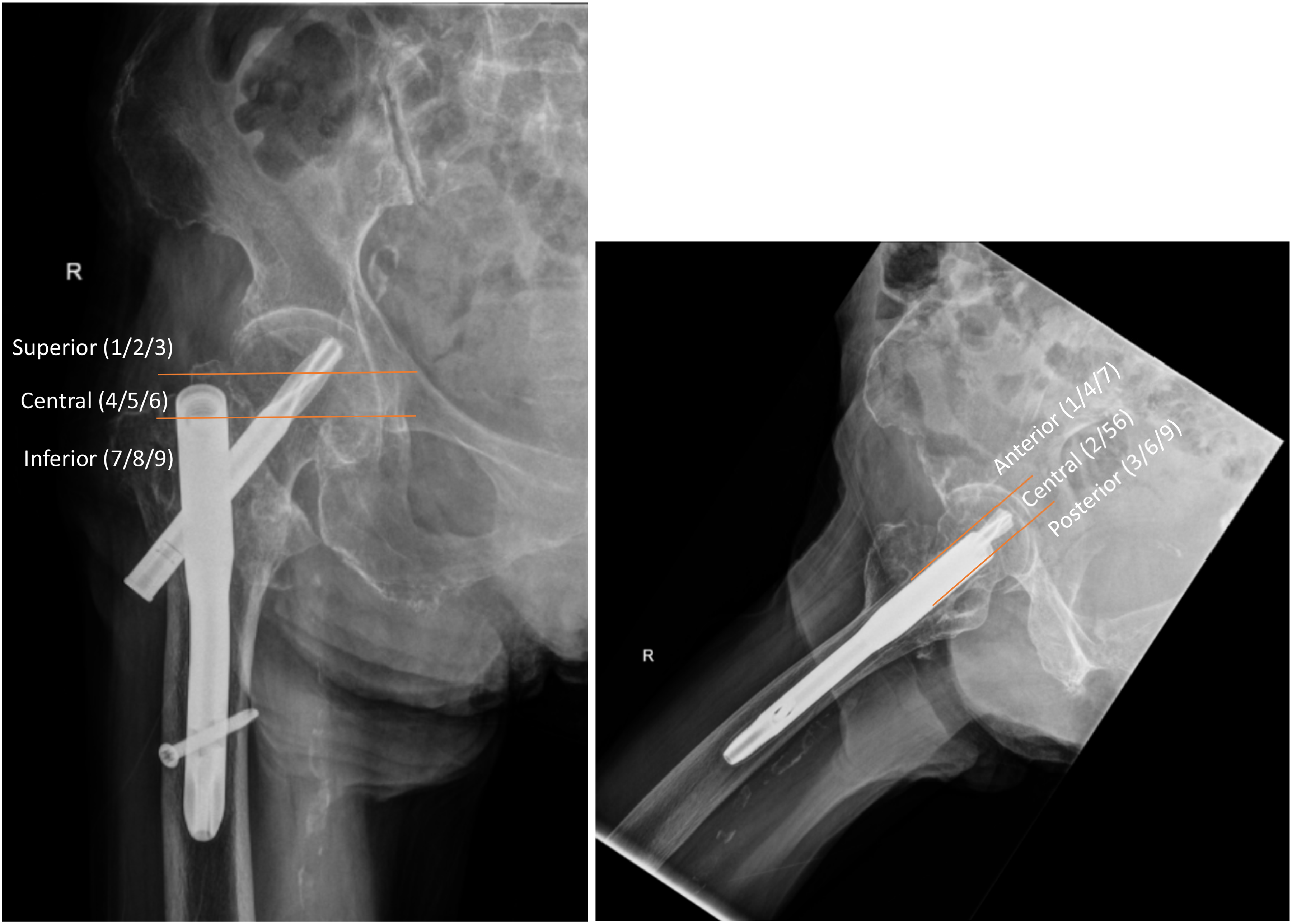
Determination of Cleveland 9 zones: an example. Cleveland zones divide the femoral head into superior, central and inferior thirds on the AP radiograph and into anterior, central and posterior thirds on the lateral film. In this example, the implant lies in quadrant 2 as it lies centrally and superiorly.
The type of locking mechanism could either be dynamic or static and their use was determined by the operating surgeon. Unfortunately, the type of locking screw was not always recorded in the operation record and was thus excluded from this study.
Data analysis
The data collected was analysed statistically using IBM SPSS version 29 (IBM Corp. Released 2022. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp). The baseline characteristics and radiological observations were compared between the cut-out group (cut-out = yes) and cut-out free group (cut-out = no) using Mann-Whitney U test for numeric variables and Chi-square test for categorical variables where appropriate. Data normality was tested using Shapiro-Wilk test, and the results showed data dispersion that deviated from a normal distribution. Resultantly, Mann-Whitney U test was used to compare numeric variables between the two groups. Stepwise multivariate logistic regression modelling was performed with cut-out being the dependent variable (reference = no). Crude logistic regression was conducted for each factor. Factors showing statistical significance were analysed again; this time controlling for the baseline characteristics that were statistically significant in the crude models. Multiple confounding factors were entered into advanced models to test their strength where appropriate. A p-value of <0.05 was considered statistically significant.
Results
A total of 147 patients were recruited to this study. Table 1 illustrates the basic demography of the patient group. The mean age of patients was 85.81 ± 8.10 years old (median age = 87.00years) and ranged between 52 and 101years (Table 1). A significant amount of cut-out cases was male (75.0%) and had chronic kidney disease (CKD) (50%). The percentage of cases with diabetes mellitus in both groups was similar. The cut-out rate was 2.72% (4 out of 147 patients).
Baseline characteristics.
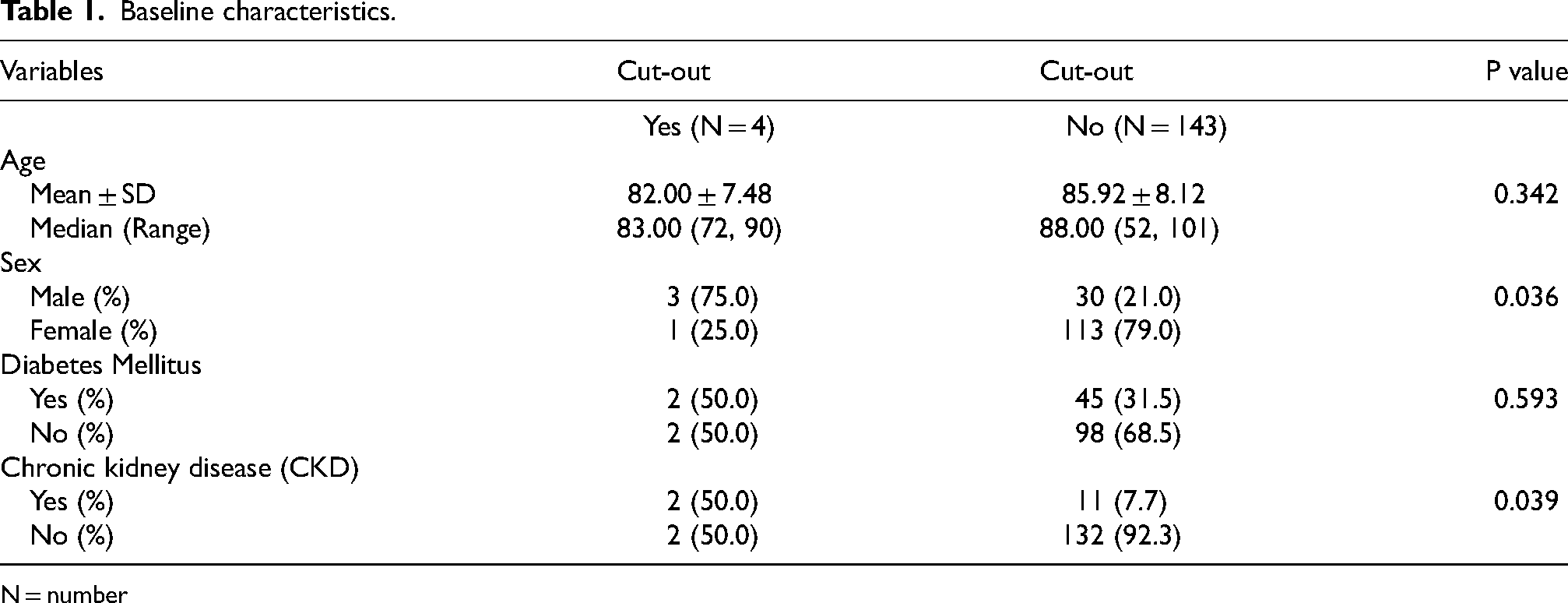
N = number
Pre-operative variables and radiological observations are highlighted in Tables 2 and 3. Surgical side did not differ significantly between the two groups. AO classification was also compared after categorising the cases into A1, A2 and A3 groups. Only subgroup analysis of the AO classification showed significant results. TAD>25 mm showed significantly higher percentage of cut-out (75.0% vs. 0.7%, p < 0.001). The distribution of PFNA blades according to Cleveland 9 zones is illustrated in Figure 4. Cleveland 9 zones did not show any significance (Table 3). Finally, cut-out free patients were significantly more likely to have good reduction quality (83.8% vs. 25.0%, p = 0.018).
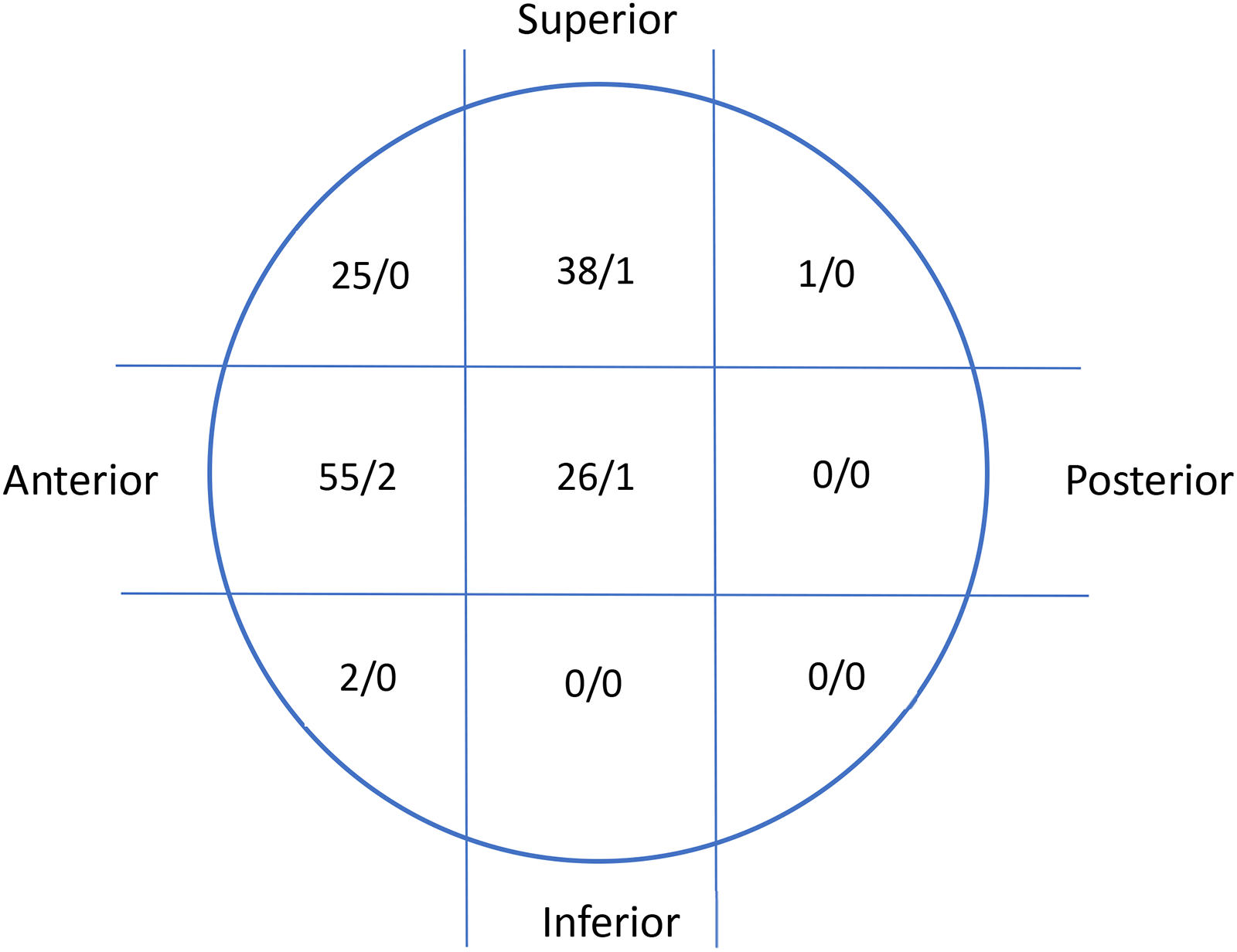
Diagrammatic distribution of femoral blade under Cleveland 9 zones.
Pre-op variables.
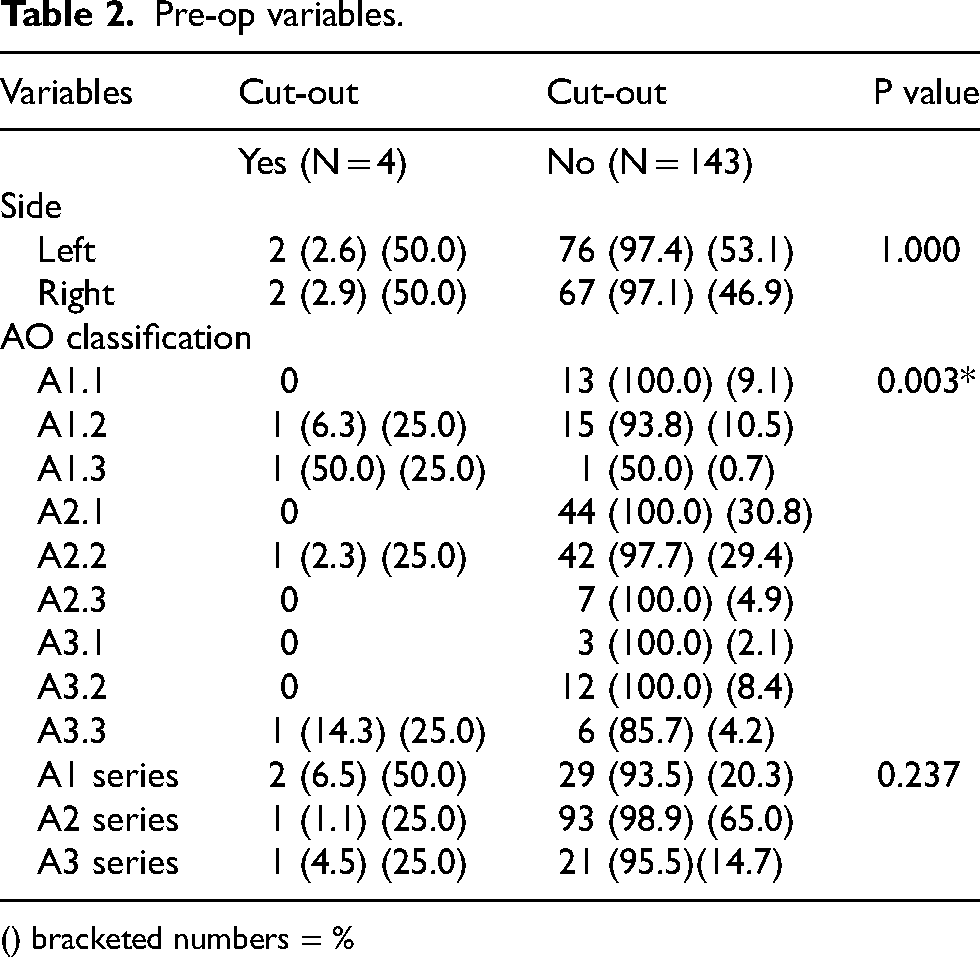
() bracketed numbers = %
Radiological observations.
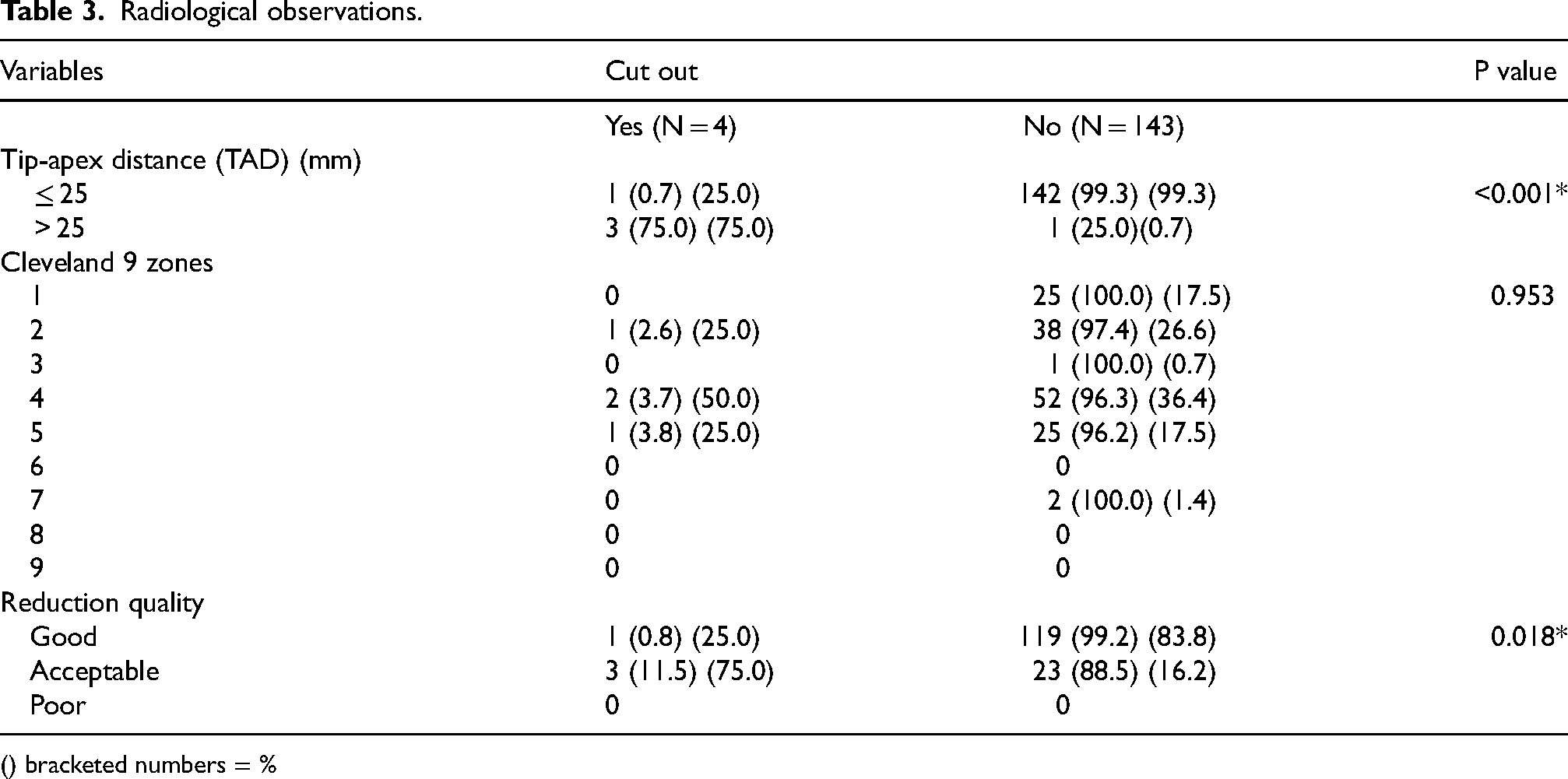
() bracketed numbers = %
The numerator (number on the left of the fraction) shows the total number of PFNA blades that landed in that zone. The denominator (number on the right of the fraction) shows the number of cases that resulted in cut-out in that zone. For example, in the most central square, the numerator shows that 26 blades landed in this zone (i.e., Cleveland zone 5) and the denominator shows that 1 of these cases resulted in cut-out.
The data underwent stepwise logistic regression analysis as detailed in Tables 4 and 5. Crude logistic regression was carried out in Model 1 (Table 4). In crude analysis, cut-out cases were statistically more likely in the male, CKD, TAD>25 mm and suboptimal reduction quality groups. Specifically, male patients were 11.30 times (95% confidence interval (of the fracture CI) = 1.13–112.56) more likely to have cut-out (p = 0.039). CKD cases were also more likely to have cut-out (Odds ratio: 12.00 (95% CI = 1.54–93.61), p = 0.018). Multivariate analyses in Model 2 and 3 then analysed possible risk factors again after controlling for either sex, CKD or both (Table 5). Cut-out cases were significantly more likely to have TAD>25 mm (odds ratio (OR) = 426.00 (21.24–8542.84)). After controlling for the baseline characteristics, cut-out cases were 263.53 times (11.84–5866.41) more likely in patients with a TAD>25 mm regardless of sex. Good reduction quality was less likely to occur in cut-out cases (OR = 0.02 (0.01–0.65)). This observation was constant even after controlling for sex (OR = 0.08), CKD (OR = 0.06) or both (OR = 0.043). In Model 3, no statistical significance was found after introducing both TAD and reduction quality into the regression model, after controlling for either sex, CKD or both.
Crude logistic regression.
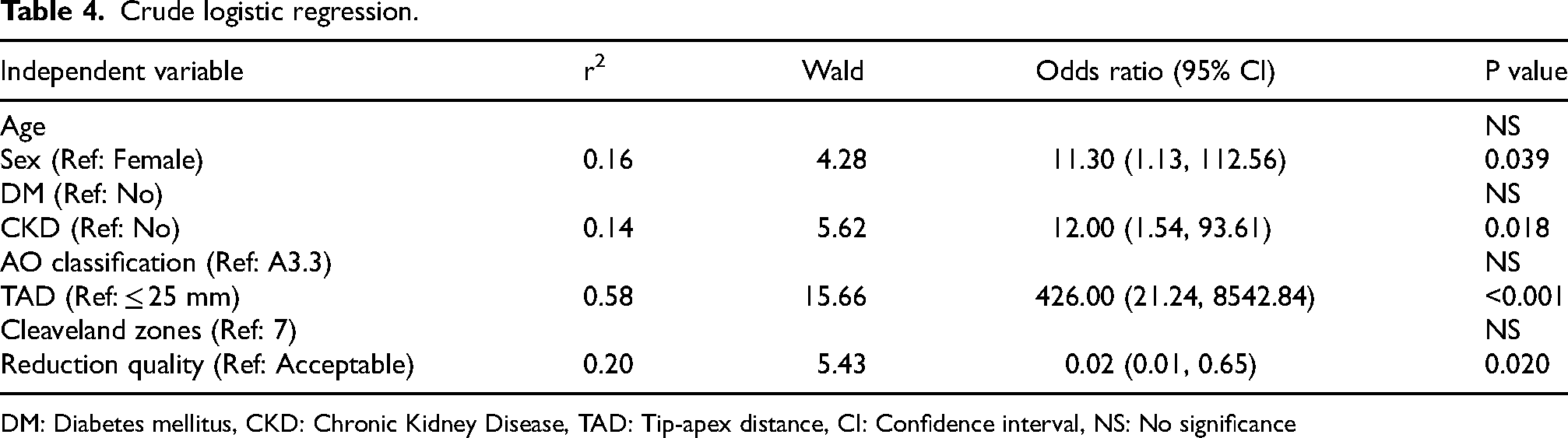
DM: Diabetes mellitus, CKD: Chronic Kidney Disease, TAD: Tip-apex distance, CI: Confidence interval, NS: No significance
Multivariable logistic regression controlling for either sex or CKD, or both sex and CKD.
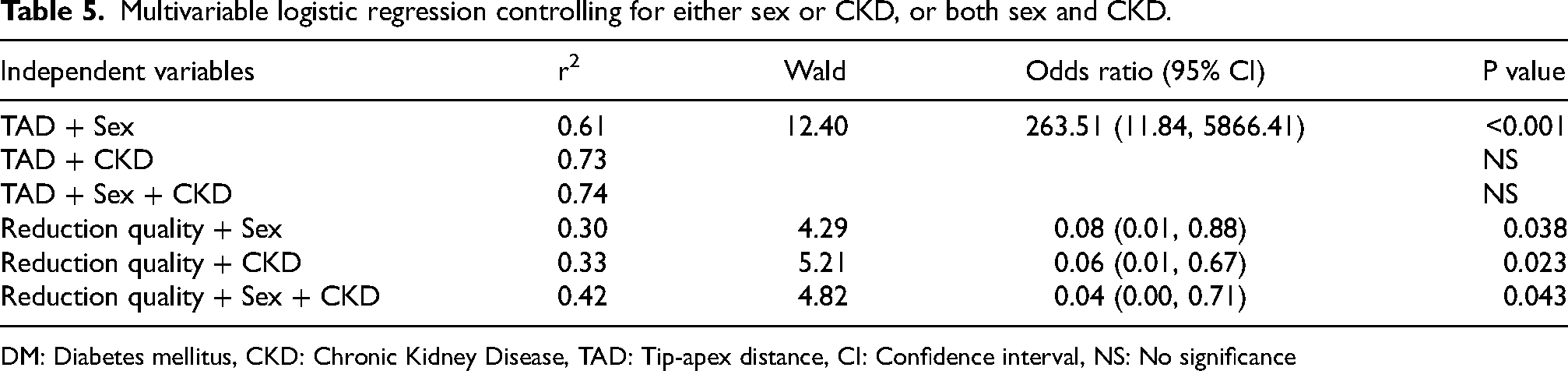
DM: Diabetes mellitus, CKD: Chronic Kidney Disease, TAD: Tip-apex distance, CI: Confidence interval, NS: No significance
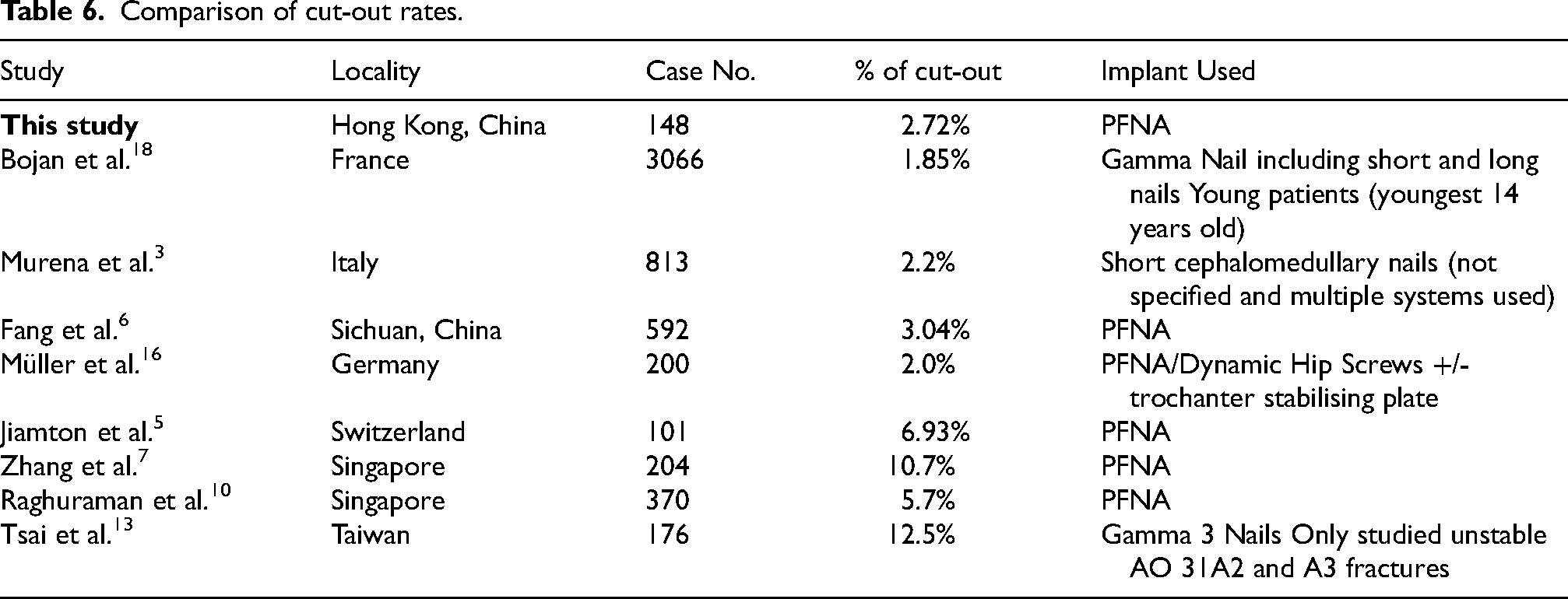
Comparison of cut-out rates.
Reference values:
TAD - Ref: ≤ 25mm
Reduction quality - Ref: Acceptable
Sex - Ref: Female
CKD - Ref: No
Discussion
Implant cut-out remains the most common complication of operative management of intertrochanteric fractures. Initially, this study collected data of all adults over 18 years old to avoid discriminating cut-out cases that occurred in younger patients with likely higher energy trauma and stronger bone density. However, likely due to this locality's aging population, our data set's youngest patient was aged 52. In fact, this was the only case of intertrochanteric fracture that was younger than 65, the cut-off for the geriatric population. The youngest cut-out case was aged 72. This is in line with other studies that mention that cut-out patients are often elderly and may be unable to endure secondary surgery due to pre-existing comorbidities.1,3 Thus, prevention precedes correction and precise identification of cut-out risk factors is key to the successful treatment of these patients. This study considered the effects of various patient demographics, TAD, reduction quality and Cleveland 9 zones.
Patient demographics including age, gender, presence of diabetes and chronic kidney disease (CKD) were analysed. Pre-operative factors including side of injury and fracture type were studied. Of these, only the male gender (p = 0.036) and the presence of CKD (p = 0.039) demonstrated significance.
Interestingly, many studies could not show gender as a significant risk factor for cut-out1,3,6–12. One study by Jiamton et al. showed the male gender as a significant risk factor for cut-out but did not provide an explanation for this occurrence. 5 Conversely, Tsai et al. showed that the female gender was a significant risk factor and reasoned that increased cut-out rates were due to gender differences in proximal femoral bone morphology and bone density. 13 In this study, 75% of the cut-out patients were male. All the male cut-out patients’ reduction quality, although not graded as good, were graded as acceptable. Some may query whether this study's male patients suffered more unstable fractures compared with the female group, which may explain the increased cut-out rates. However, their AO gradings did not reflect very comminuted patterns as the most severe pattern in the male cut-out cohort was only 31A2.2. Therefore, the authors of this study were wary in drawing too many conclusions on the significance of gender at this juncture; especially when other studies were also inconsistent. Nonetheless, this finding was an interesting and unexpected result to report even at this preliminary stage as it warrants further exploration in future studies.
CKD and fracture type were also analysed risk factors. A significant relationship between CKD and increased cut-out rates is likely due to the known relationship between renal dysfunction and poor bone quality. 14 In terms of fracture type, significantly higher percentages in the fracture subtypes A1.2, A1.3, and A3.3 had implant cut-out. However, the statistical significance disappeared when the fracture types were gathered into their broader A1, A2 and A3 groupings. Results from other studies were also mixed. A few studies report statistically significant cut-out rates in the complex fractures group.4,7 Yet in Kashigar et al.'s study, no statistical significance could be found for fracture pattern. 8 Conversely, Murena et al. showed that a more unstable fracture pattern was statistically significant at the univariate analysis but not in the multivariate analysis. 3 Similarly, although Fang et al. used the Evans-Jensen fracture classification system over the AO system, Fang et al. could only show a significant relationship between cut-out and fracture pattern in the univariate analysis but not in the multivariate analysis. 6 Both studies concluded that whilst an unstable fracture may be a contributing factor, it is not an independent factor for cut-out.3,6 This study could not confirm the relationship between fracture pattern and cut-out rates either.
For this study, the operative risk factors studied included TAD, Cleveland 9 zones and Baumgaertner's Reduction Quality. There was a significantly higher percentage of cut-out patients with a TAD>25 mm than cut out free patients (75.0% vs. 0.7%, p < 0.001). On the other hand, cut-out free patients showed significantly higher percentage of good reduction quality than cut-out patients (83.8% vs. 25.0%, p = 0.018). This study could not show a relationship between cut-out and Cleveland 9 zones. Thus, TAD and reduction quality were the most important operative factors for cut-out.
A TAD>25 mm is the most infamous risk factor for cut-out in literature. However, its significance does not come without debate. Originally, the 25 mm TAD limit was popularised by Baumgaertner et al. around 20 years ago. Baumgaertner et al. based the TAD on biomechanical studies that suggested the hip screw should be placed centrally and deep within the femoral head. 9 However, since then, studies such as Goffin et al. have argued that a TAD>25 mm could not be considered an accurate predictor of lag screw cut-out as it should be adjusted depending on the size of the femoral head.3,15 Meanwhile, some studies such as the one by Raghuraman et al., failed to even demonstrate a relationship between cut-out and an increased TAD. 10 These viewpoints contrast with this study which demonstrated a significant cut-out occurrence for patients with a TAD>25 mm. This significance remained even after controlling baseline factors. In Model 2, a TAD>25 mm translated to being 263.52 times more likely to have cut-out regardless of sex. This significant finding was discovered without adjusting for the femoral head size. Moreover, some studies argue that an alternative version of TAD, the CalTAD, should be used. The newer calcar tip-to-apex (CalTAD) is referenced to the femoral calcar and not the centre of the neck. However, this study decided against using CalTAD as a radiological measurement as no optimal for CalTAD has been identified. Moreover, currently, no study has been able to show CalTAD's superiority over TAD for predicting cut-out.6,12 Nonetheless, this study supports Baumgaertner's original definition of TAD>25 mm as an important risk factor for cut-out.
Another radiological observation that could be used to define implant position in the femoral head is by using Cleveland 9 zones. This study could not determine a relationship between the Cleveland 9 zones and cut-out which is unsurprising as the optimal implant placement within these zones is heavily debated. In general, a central position is agreed upon as this is the location of the strongest trabecular bone.1,5,8,16 An anterior positioning should also be avoided.1,5 However, whether the implant should be positioned in the inferior, superior or posterior position is controversial. For example, Müller et al. suggests a central-central (zone 5) position. 16 However, Andruszkow et al. advocates a posterior-inferior (zone 9) position as a posterior position could support the posteromedial cortex.1,3,12 Jiamton et al. suggest either zone 5 or 9 is optimal. 5 Yet Zhang et al. argue that a posterior position increases cut-out. However, Zhang et al. later acknowledges that there are opposing viewpoints in the protectiveness in the posterior positioning of the hip implant. 7 In a biomechanical study by Kuzyk et al., an inferior position provides higher resistance to axial and torsional stresses. 17 This study's results reflect that the depth of the nail as reflected by TAD may play a larger role in cut-out reduction than implant positioning by zones.
Reduction quality was assessed radiologically by Baumgartaener's criteria. In the included cases, all cases either had an acceptable or good reduction. As aforementioned, a good reduction was less likely to occur in the cut-out cases. A good reduction involves minimising fracture gapping and varus malalignment. Minimal fracture gapping is important for bone healing and fracture stabilisation. A slightly valgus reduction was reported to diminish deforming forces by reducing the distance between the plate or nail and the weight-bearing axis. 1 As the weightbearing portion of the proximal femur, the posteromedial calcar carries the highest stress. Once the medial femoral cortex is broken, varus deformity can easily occur and will promote implant failure. 6 Conversely, a valgus reduction reduces implant loads and induces interfragmentary compression.5,7 This study thus shows that whilst the TAD is important, careful attention should be given to good reduction principles.
Finally, the cut-out rate of this article is 2.72%. This cut-out rate is comparable to those quoted in the literature (Table 6). There is a large range of cut-out rates in the literature and can range anywhere from 1.85%—19.5%.3,6,10 It should be noted that the low 1.85% cut-out rate was from a large French study of 3066 cases that included cases as young as 14 years old. 18 This study's youngest patient was 52 years old. The French study considered gamma nailing and included long intramedullary nailing whereas this study only included short intramedullary PFNA nailing. These factors may slightly affect the comparability of this study. Nonetheless, this study's cut-out rate remains comparable to other quoted rates.
This study has multiple strengths. Firstly, all radiological assessments were done by a single observer. This limited this study's inter-observer error. This study also had a comparable minimal time of follow-up. The time of minimum follow-up of 3 months was chosen since Baumgaertner originally reported this as an adequate timeframe to identify cut-out. This was also a chosen timeframe of many other studies. 5 Furthermore, to the best of the authors’ knowledge, this is the first study to study local intertrochanteric fracture cut-out rates in Hong Kong. Despite the strengths this study does contain limitations. Firstly, it is a retrospective study. Secondly, although surgically advantageous for this centre, another limitation of this study is the relatively low cut-out rate. Yet, the limitations also expose future study possibilities.
Future studies include studying the risk factors not detailed in this study, such as osteoporosis and dementia. Despite osteoporosis being a known cause of poor bone density, this study decided against including osteoporosis as not every patient underwent a DEXA (Dual-energy X-ray absorptiometry) scan before intervention. Some studies attempted to circumvent this issue by using the Singh index. However, the Singh index is prone to operator bias and did not always correlate with the actual bone density. 4 Thus, given that there was a high risk of underdiagnosis and under-documentation of osteoporosis, this study did not evaluate it as a possible risk factor. Another potential risk factor that was not studied for similar reasons would be dementia. Of course, this analysis also warrants further prospective, larger and multicentre studies. Thus, the limitations of this study only unlock further possibilities.
Conclusion
Intertrochanteric hip fractures represent a very debilitating injury in the elderly population. The gold standard of treatment remains surgical and cephalomedullary nailing remains a popular option. Blade cut-out remains the most frequent reason for implant failure and often requires secondary surgery to rectify the issue. However, secondary surgery increases socioeconomic, healthcare burdens and morbidity to this frail patient group. Thus, the prevention of cut-out should be the primary goal. Baseline characteristics including a male sex and presences of CKD were risk factors of cut-out. Operative risk factors for cut-out include a TAD>25 mm and suboptimal reduction quality. Given cut-out remains the most common cause of implant failure, attention to these factors would assist in mitigating patient morbidity.
Footnotes
Data availability
The datasets generated during and/or analysed during the current study are not publicly available due to patient privacy but are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.