
Abstract
Introduction
Paediatric hip fracture is rare but the consequences can be devastating. Retrospective analysis was performed in a local trauma centre.
Methods
This study retrospectively reviewed 18 paediatrics patients with hip fracture from 2000 to 2021 in a territory hospital in Hong Kong. Serial hip images and clinical symptoms were reviewed.
Result
Significant (44.4%) amount of patients had injury during sports. An ambulatory status on presentation (16.7%) had to be highlighted. Despite a higher incidence of avascular necrosis (44%) reported, only two patients required salvage operation. The mean follow-up time was 77 months.
Conclusion
A shift in mechanism of injury and presentation from historical local data in 1986 to recent 20 years were identified. The mechanism of injury shifted from prior road traffic accident to sports injury. Preserved mobility after hip fracture was common, reminding medical practitioner to stay vigilant for early diagnosis. Higher avascular necrosis rate was reported but limited salvage operations were noted. Larger cohort with longer follow-up time would be needed for analysis of risk factors associated with avascular necrosis.
Keywords
Introduction
Paediatrics hip fracture was an uncommon injury, accounting for less than 1% of fractures in paediatrics’ population. The mechanism of injury was thought to be high energy trauma such as motor vehicle accident or fall from height in paediatrics population.1–4 The difference in vascular supply in skeletally immature hips compared with the skeletally matured predisposing them into a higher risk of vascular disturbance to the femoral head and proximal femoral physis 5 and subsequent devastating complications, namely avascular necrosis, premature physeal closure, and osteoarthritis. 6 Potential remedial surgeries and prolonged follow-up brought parental anxiety and great medical cost to the healthcare system.
Timely recognition and management were thought to be associated with better outcome. 7
Limited local data in Hong Kong was available. This could be dated back to 1986 by Leung and Lam 6 and 1999 by Cheng and Tang. 8
This study aimed to revisit the epidemiology, injury mechanism, and outcome of paediatrics hip fracture in a territory trauma centre, evaluating factors contributing to the healing and complications hip fracture, particularly, avascular necrosis, which would be valuable while counselling parents on the treatment outcome.
Method
This study retrospectively reviewed all patients aged ≤18 years old who sustained fracture hip between 3 January 2000 and 30 June 2021 in a territory hospital in Hong Kong.
Twenty patients were identified, and two were excluded due to follow-up interval < 12 months. This was because avascular necrosis would most likely be detectable within a year of injury.2,4,9 Patients’ clinical records and radiological results were assessed and recorded.
Fractures were classified by Delbet classification according to the initial injury film or as recorded by surgeon intra-operatively. They were also classified by Garden classification into displaced or non-displaced fracture.
The quality of reduction was determined by the degree of step-off and angulation based on immediate post-operative radiographs. We graded the quality of reduction by the following scale: excellent, less than 2-mm step-off and no angulation; good, less than 4-mm step-off and less than 5° angulation; fair, greater than 4-mm step-off and less than 10° angulation; and poor, greater than 5-mm step-off and greater than 10° angulation. 10
Serial radiographs and/or magnetic resonance imaging (MRI) of affected hip was evaluated for any evidence of avascular necrosis, coxa vara, or physeal arrest. Not all patients received MRI post-operatively. In these cases, plain radiographs of the hip would be evaluated instead.
Patient's subjective outcome of pain and effect on activity of daily living were assessed on their latest follow-up.
All patients were followed up for a minimum of 12 months. The mean length of follow-up was 77 months.
All patients were managed operatively within 24 h from admission from emergency department. None managed conservatively with bed rest or hip spica alone. Capsular decompression was performed in selected patients, depended on surgeons’ preference. This was partly due to some patients came with delayed presentation, and that the benefit of capsular decompression was still controversial in earlier days. While nowadays, there was more consensus on the need of capsular decompression due to the theoretical bases of reducing intra-capsular pressure. 5 In addition, it brought no significant morbidity. All patients were allowed non-weight bearing for 8 to 12 weeks until fracture union. They were allowed to have free hip mobilization post-operatively without the use of hip spica. Interval radiographs were arranged upon follow-up. MRI of the affected hip was arranged for selected patients post-operatively.
Result
There were 18 patients included in this study with 13 boys and 5 girls. Their age ranged from 6 to 18 years old with a mean of 12.9 years old.
Eleven of them injured their left hip (61.1%), and 7 (38.9%) injured their right hip. None suffered from bilateral hip fracture. Three cases (16.7%) sustained concomitant injury which were not life-threatening nor hinder them from subsequent management of hip fracture.
The major cause of injury was sports-related (Figure 1a), found in eight cases (44%). Within this, three of them injured during ball games (football, basketball, rugby), four during sports involving rapid acceleration and deceleration (including inline roller skating, skateboarding, wakeboard), and one was not specified during physical education lesson. Another major cause was falling from height, found in six cases (33.3%). However, the height that patient fell from varies, one patient reported falling from more than 6 m, another one from 2 m, while the rest fell from <1 m height. It was worth to mention that three patients (16.7%) sustained fracture with a level ground fall. One case had not specified the cause of injury.
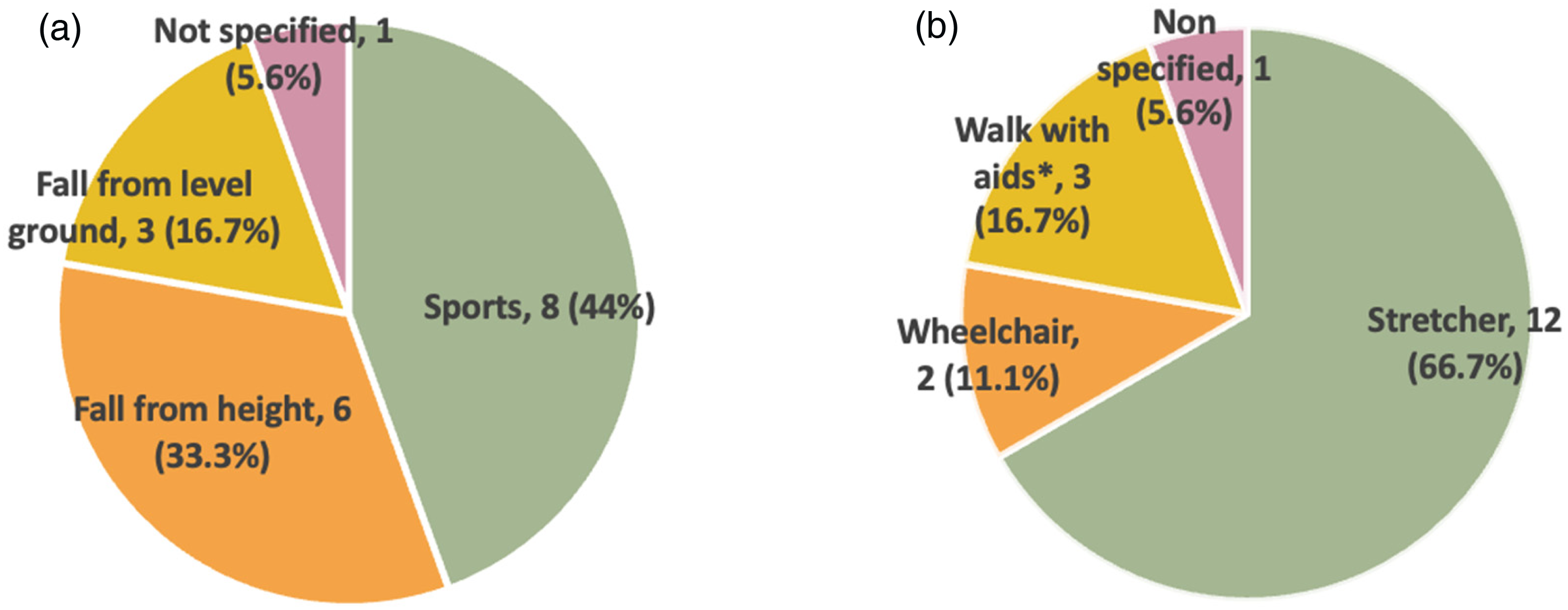
(a) Injury mechanism. (b) Ambulatory status on presentation. Remarks: *Two patients walk with limp, one patient walk with walking aids.
Among the three cases who sustained fracture in a level ground fall, the serum calcium and phosphate levels were normal.
None of the cases suffered from pathological cause nor non-accidental injury.
Fracture patterns were classified by Delbet classification. Majority of the cases belonged to type II transcervical fracture, found in 16 cases (88.9%); while the remaining two (11.1%) belonged to type III cervico-trochanteric fracture. None of the cases were trans-epiphyseal separation nor inter-trochanteric fracture.
The fracture pattern was classified into displaced or non-displaced fracture by Garden classification. Twelve patients (66.7%) suffered from displaced fracture, five (27.8%) suffered from non-displaced fracture, and one patient had no documented status nor initial film for comment.
Fourteen patients (77.85%) attended the emergency department for medical attention within 24 h from injury. Four patients (22.2%) had delayed presentation. Among the four cases with delayed presentation, two cases sought medical attention more than one week after the initial injury. They were both able to walk with limping gait when they first presented to the emergency department and diagnosed with an undisplaced hip fracture. The third case (Figure 2) attended the emergency department on the same day of injury with X-ray performed showing undisplaced neck of femur fracture. Yet, the diagnosis was missed and she was discharged home. She re-attended eight days later for persistent pain and was admitted for displaced neck of femur fracture. The fourth case was initially managed overseas and was transferred back two days after the injury for definitive management.
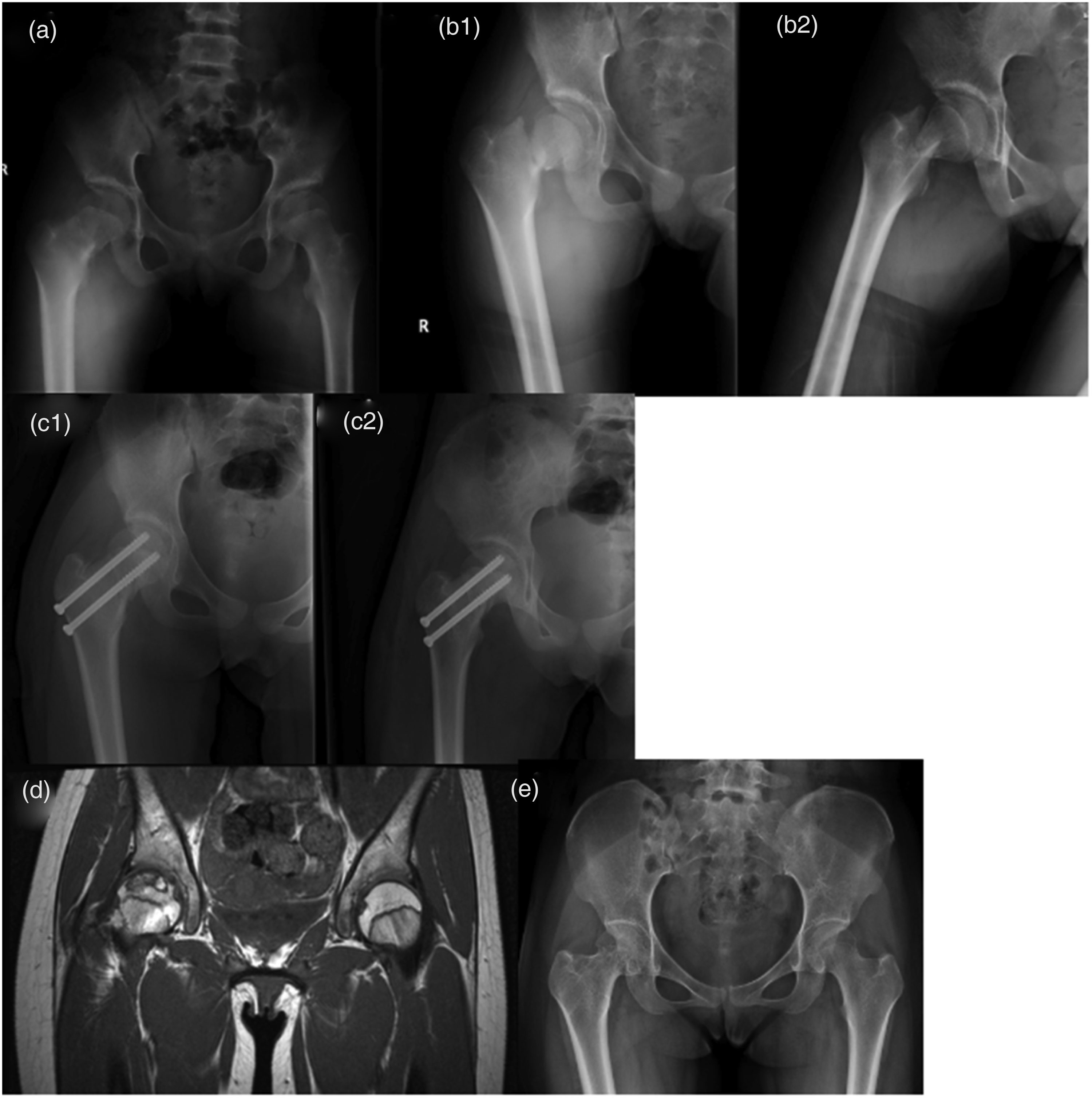
Index case 14. (a) A 10-year-old girl fall from father's back. X-ray on first attendance to emergency department. (b1, b2) 14: X-ray on second attendance to emergency department on 8 days following initial injury. (c) Post-operative X-ray: closed reduction and fixation with two cannulated screws. (d) MRI taken post-operatively 5 months. (e) X-ray taken post-operatively 6 years and 5 months showed no sign of avascular necrosis.
Regarding the ambulatory status (Figure 1b) upon presentation to our emergency department, most patients required stretcher (66.7%) or wheelchair (11.1%), but there were also patients able to walk independently with limping or handheld aid (16.7%).
A total of 78% patients received surgery within 24 h from injury. The remaining patients failed to received operation within 24 h from injury due to delayed presentation. All patients underwent surgical management with internal fixation. Three (16.7%) had fracture fixation in situ, 13 patients (72.2%) had closed reduction and two patients (11.1%) who had unacceptable alignment on closed reduction required open reduction. In both cases, anterior approach was adopted for open reduction.
All transcervical fracture (16 cases, 88.9%) was managed with screws, and all cervico-trochanteric fracture (2 cases, 11.1%) was managed with screw-plate system (Figure 3). Among cases using hip screws for fixation, 10 (62.5%) patients were fixed with three screws, five (31.3%) were fixed with two screws, and one (6.3%) was fixed with one screw. Seven (38.9%) underwent capsular decompression. Two-thirds of the cases with traceable operative time recorded, the mean operating time was 84 min with a range of 27 to 382 min.
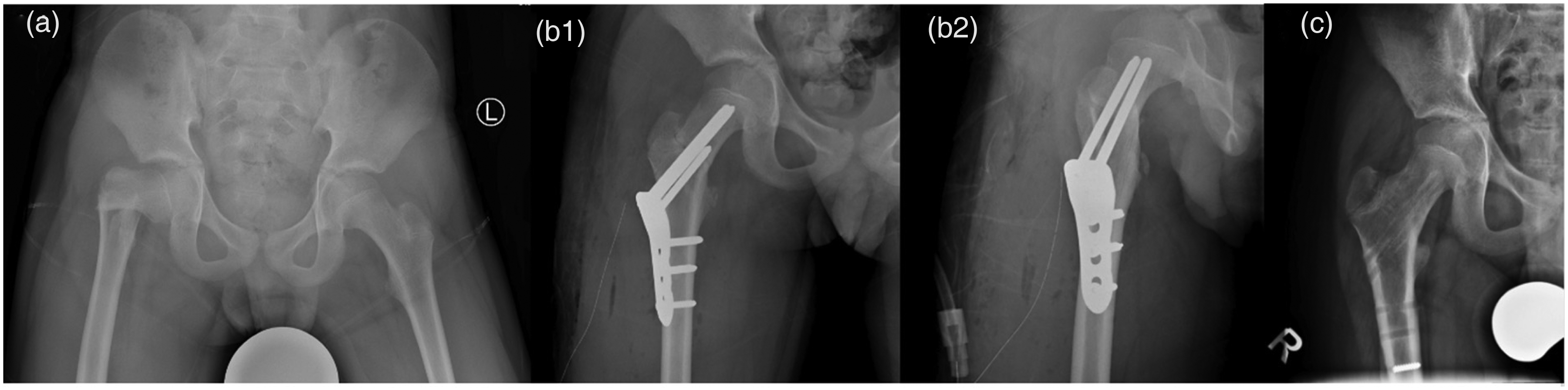
Index case 17. (a) Injury film: 10-year-old boy fall from one step of stair resulted in Delbet III fracture right hip. (b1, b2) Post-operative X-ray: closed reduction and fixation with paediatric hip plate. (c) X-ray film post-operative 13 months showed no avascular necrosis.
Immediate post-operative plain radiographs were reviewed and assessed for the quality of reduction. Immediate post-operative radiographs were available in 61.1% of the cases for assessment of immediate quality of reduction. The radiographs of the remaining had been discarded as part of institutional policy. Six (33.3%) were graded excellent, two (11.1%) were graded good, and three (16.7%) were graded fair. 10
Eight patients (44.4%) developed radiological avascular necrosis detected by plain radiographs or MRI. Three of them had avascular necrosis diagnosed by MRI alone without plain radiographs changes. Among all the eight patients complicated with avascular necrosis, four patients remained asymptomatic and four patients were symptomatic. Only two patients with symptomatic avascular necrosis underwent remedial surgery because of disturbing pain and stiffness that affected their activities of daily living. One had hip arthroscopic decompression for femoral impingement syndrome at 13 years post-injury and finally total hip arthroplasty for osteoarthritis at 15 years post-injury. The other had pelvic osteotomy performed four years post-injury in another hospital with untraceable record.
No patient suffered from non-union. A total of 22.2% cases suffered from malunion, as evidenced by neck shaft angle < 125° or >140° in post-operative X-ray. In all these cases with fracture malunion, all patients had concomitant avascular necrosis.
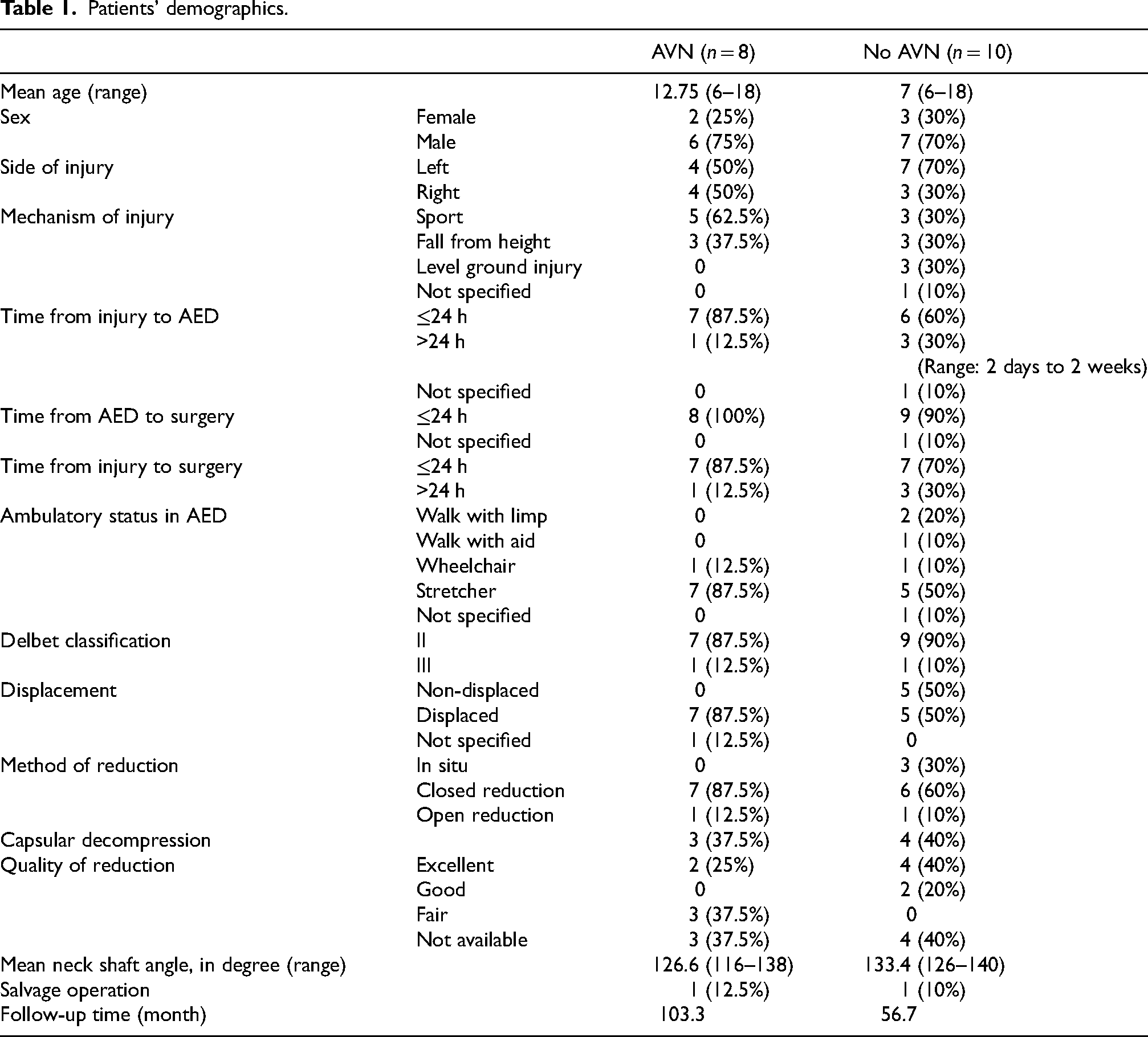
Statistical analysis had been performed to evaluate the significance of demographics between the two outcome groups with and without avascular necrosis. However, no statistical significance was detected, which was likely due to relatively small study size (Table 1).
Patients’ demographics.
Discussion
This series of 18 patients with prolonged follow-up interval reflected the change in epidemiology in our locality compared with the study done in 1999 by Cheng 7 et al.
While majority of patients injured due to road traffic accident (36%) and fell from height (57%) in older days, 7 it was now replaced by sports injury, accounting up to 44.4% of our cohort of patients (Table 2). Skateboarding, roller skating, and scooter riding became the newer trending sports activities enjoyed by many adolescents and children. The high velocity sports and deceleration type injury after landing from a certain level of height might result in high energy trauma. Epidemiological study reported a large number of paediatric fractures causes by skateboarding, roller-skating, and scooter-riding accidents, particularly open fractures of the forearm. 11 Other than a few skate parks in Hong Kong, it was not surprising to see adolescents and children playing skating sports in playgrounds and cycling trails. Potential crash injuries with other playground or cycling trail users were undoubtedly a concern. In addition, skate park users must wear a safety helmet, while other protective gears, such as elbow pads, knee pads, wrist guards, and hip protectors, were used on a voluntary basis. Non-compliance with the use of protective equipment in paediatric population was multifactorial. Peers influence and safety education played an important role. Given the devastating consequence after hip fracture and upper limb fractures, education to skating sport users and their parents about the importance of safe riding practices and the need for protective equipment should be further emphasized.
Demographics comparing study by Cheng and Tang 8 and this series.
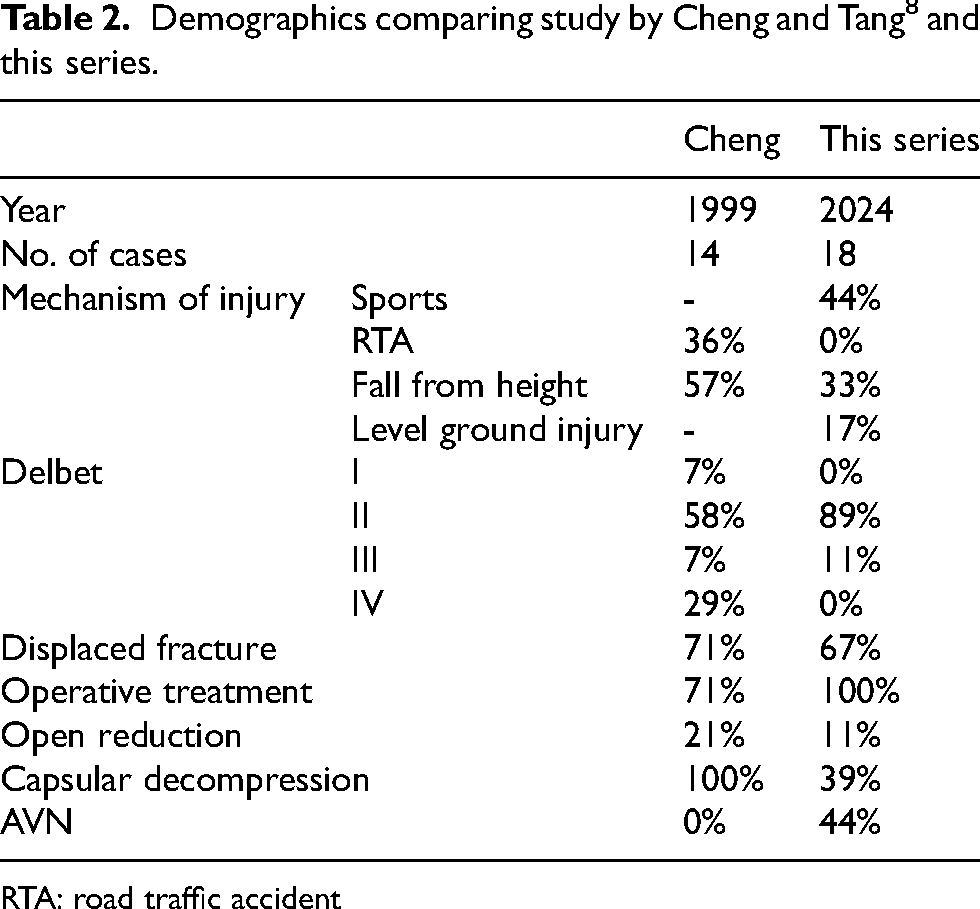
RTA: road traffic accident
Sixteen per cent of patients suffered from hip fracture after a level ground injury. This injury mechanism was less commonly encountered in the older days. 7 One may postulate the deterioration in bone health. Rickets was thought to be less common in developed countries. In fact, epidemiological study in Hong Kong revealed that vitamin D deficiency and insufficiency were highly prevalent among adolescents, 12 which may be related to changes in lifestyle. The availability and prolonged use of computers, habitual watching of television, and heavy amounts of homework from schools kept young subjects away from outdoor activities. In addition, the use of sunscreen leading to reduced amount of sunlight exposure and diminished UV-dependent vitamin D synthesis. 13 Concerns had to be raised for bone health development in adolescent.
Prompt diagnosis and early surgical fixation prevent fracture displacement and complications in paediatric hip fracture. 5 Despite the readily available emergency and general health care services in Hong Kong, there were substantial number of cases (22.2%) with delayed presentation and subsequent delayed diagnosis and treatment in our cohort. It would be important to highlight that paediatric group patients who sustained hip fracture could be the result of high or low energy trauma, and they could give atypical presentations. Among the four cases presented late to our hospital, two cases were able to ambulate with a limp, accounting up to 16.7% of our cohort. Emergency physicians and general practitioners should be vigilant for paediatric patients who presented with hip or knee pain following hip contusion, even they were able to bear weight, or the injury mechanism was less alarming. Management should include immediate bedrest and urgent referral for antero-posterior and cross table lateral view of the hip. ‘Wait and see approach’ would not be recommended.
All patients were managed surgically compared with conservative management by bed rest, traction or hip spica alone in non-displaced fracture in older days. While it was quoted 6–10% of non-union rate in conservative treated patient, 14 none of our cohort suffered from fracture non-union with aggressive surgical fixation. The choice of fixation implant was guided by the fracture pattern by Delbet classification. All the Delbet Class II fractures were fixed with screws while all Delbet Class III fractures were fixed with screw-plate system.
We reported higher incidence of avascular necrosis (44%) compared with Yeranosian 15 et al., who reported 23% osteonecrosis across 30 studies. Despite all cases were managed aggressively by internal fixation and timely within 24 h from admission from emergency unit with acceptable quality of reduction, we still see a significant proportion of patients suffered from the devastating avascular necrosis. Possible reasons include a substantial higher percentage of Delbet II fracture and fracture displacement in our cohort, accounting for 89% and 67%, respectively. In addition, with the increasing availability of MRI imaging made it more routinely performed in the past decade. With the higher sensitivity of MRI in identifying avascular necrosis, there were cases had MRI detectable avascular necrosis without apparent radiographic changes such as sclerosis, cystic change, or collapse; nor any significant clinical symptoms such as pain or hip stiffness. This was reflected from our cohort where 37.5% avascular necrosis was diagnosed on MRI alone without plain radiographs changes. On the contrary, while we might be considering salvage operation such as bone grafting, redirection osteotomy, prosthetic resurfacing, or even arthroplasty, we noticed that some patients may have overt X-ray changes of avascular necrosis but tolerable symptoms (Figures 4b and 5). Spontaneous regression of avascular necrosis was also evident (Figure 4a). Ultimately, only two patients from our cohort decided to undergo salvage operation following symptomatic avascular necrosis – one with pelvic osteotomy, the other with repeated hip arthroscopy and finally total hip replacement. This may echo with the study by Leung and Lam 6 which found that 19 out of 41 patients developed symptoms over a mean follow-up of 18 years. A more prolonged follow-up would be needed to identify patients with symptomatic avascular necrosis requiring salvage or remedial surgery.

(a1) Index case 15 – 10-year-old girl MRI showed right femoral head avascular necrosis at post-operative 5 months. (a2) Repeat MRI at post-operative 29 months showed revascularization and reduction in size. (b1) Index case 7- to 6-year-old boy X-ray taken 7 months post-operatively. (b2) X-ray taken 4 years and 10 months post-operatively – fracture left hip healed in malunion with shorter neck and varus. Patient reported no disturbing symptoms. (c) Index case 9 – 15-year-old boy X-ray taken 11 years and 5 months post-operatively: left hip fracture fixed with screws, complicated with avascular necrosis, cut out implant, almost hip fusion by surrounded osteophyte but patient had tolerable symptoms.
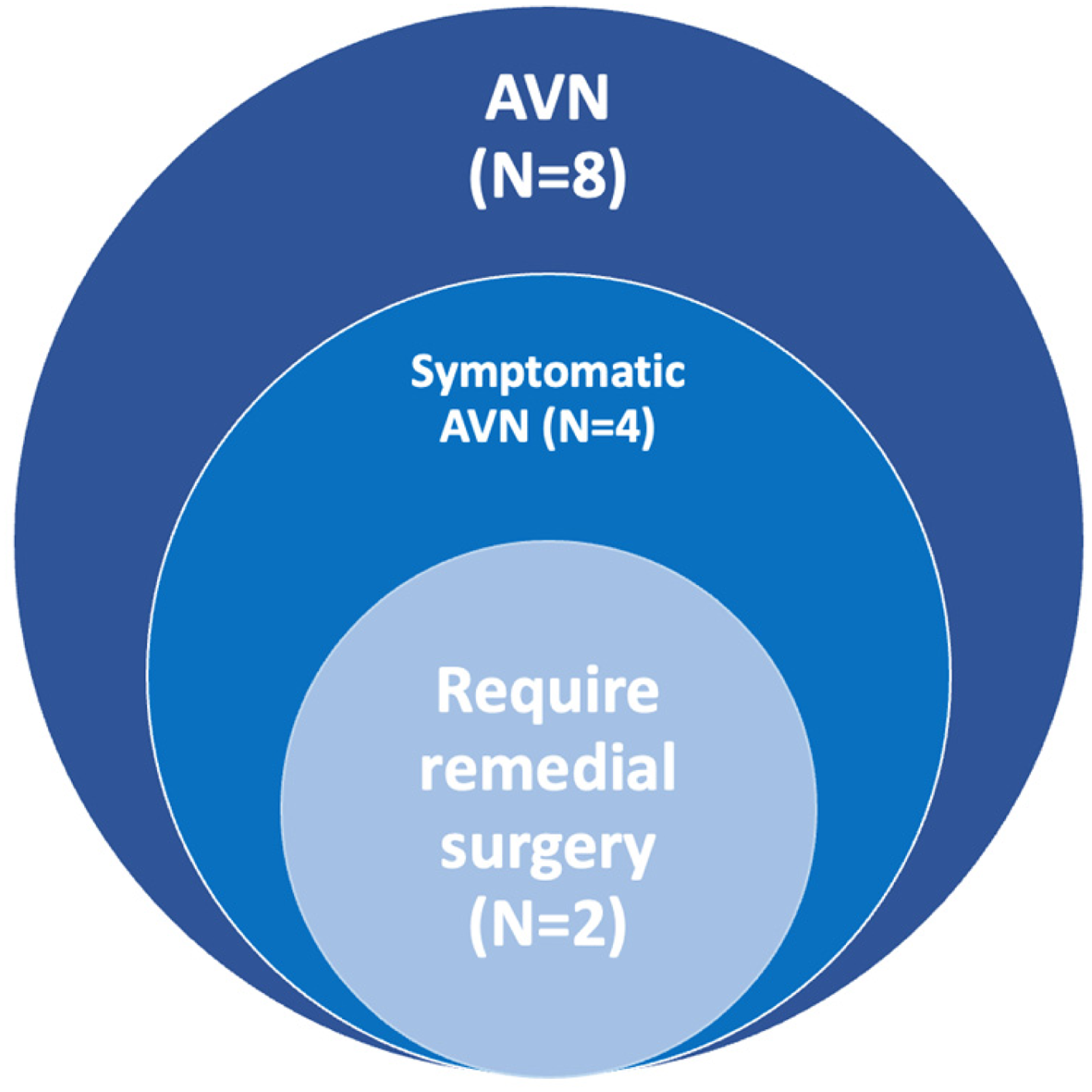
Numbers of patients with avascular necrosis (AVN) requiring remedial surgery.
Limitation
Avascular necrosis in hip fracture was multifactorial. Limited by the number of patients, we were unable to draw conclusion on which factor being the most important risk factor. Larger cohort for future analysis of risk factor associated with avascular necrosis would be needed. Secondly, as no standardized follow-up protocol was adopted, time to union could not be measured. Lastly, as it involved a long study duration, multiple surgeons were involved.
Conclusion
This cohort of patients demonstrated a change in epidemiology on the cause of hip fracture, involving more sports injury. Public safety awareness on the danger of sports and need of personal protective equipment during high risk sport activities should be raised. There was also rise in low energy trauma, as a result, some may be able to bear weight with limping on presentation, in contrast the usual conception that hip fracture patient had difficulty in weight bearing. Management with operative reduction and internal fixation based on the fracture type by Delbet classification allowed effective fixation with no non-union. Larger cohort with longer follow-up time would be needed for analysis for risk factor associated with avascular necrosis, which would help us in counselling parents perioperatively.
Footnotes
Author contributions
All authors contributed to the following items: (a) concept or design; (b) acquisition of data; (c) analysis or interpretation of data; (d) drafting of the manuscripts; and (e) critical revision for important intellectual content. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from Central Institutional Review Board (IRB/REC ref. no.: PAED-2023-011).