
Abstract
Introduction
Since the beginning of Coronavirus disease 2019 (COVID-19) pandemic, schools in Hong Kong were suspended intermittently as part of the anti-epidemic measure. This study aims to investigate the impact of COVID-19 pandemic on the epidemiology of paediatric fracture and bone health of children.
Methods
We recruited patients aged 3–17 admitted to tertiary paediatric orthopaedic trauma centres for fractures from 1st February 2020 till 4th March 2021 during COVID-19 period as study group and compared with patients admitted from 1st February 2019 till 31st January 2020 before COVID-19 as control group.
Results
Total number of admissions due to fracture was reduced by 49% (pre-COVID period: 345, COVID period: 177). Demographic data such as age, age group distribution, sex, location of fractures, energy of injury, prior history of fracture were comparable in the two groups. There was no statistically significant difference in the proportion of patients requiring operative treatment. Significant change was found in injury mechanisms, with injury related to body-powered vehicles (33.7%, n = 58) becoming the leading cause of injury during COVID period (p < 0.001). There was significant drop in proportion of patient with injury from level ground fall (p < 0.001) and sports (p < 0.001). The percentage of obese children increased significantly (p = 0.009) during the COVID period (32.7%, n = 48) than pre-COVID period (21.0%, n = 67). The proportion of patients with hypocalcaemia was found to be higher (p = 0.002) during COVID period.
Conclusions
This study reflects paediatric bone health issues during COVID-19 pandemic. We postulate the reduction in fracture incidence, change in the distribution of injury mechanisms, and more obesity could be related to a more sedentary lifestyle during COVID period. Hypocalcaemia can be associated with reduced sunlight exposure, obesity, and lack of physical activities. If the problem is left neglected, it can lead to long-term bone health problems.
Introduction
The Coronavirus disease 2019 (COVID-19) outbreak was declared to be pandemic on 11 March 2020 by World Health Organization. 1 Since the beginning of the COVID-19 pandemic, the Hong Kong Government has adopted social distancing policy for infection control purposes. The Secretary for Education announced the extension of schools’ Chinese New Year holiday on 31 January 2020, 2 followed by suspension of full-day in-person classes. It marked the start of the suspension of on-campus and extra-curricular activities of schools in Hong Kong. Besides, playgrounds and sporting venues were temporarily closed due to social distancing restrictions. Children were unable to engage in physical activities and group sports as a result. The impact of these policies on paediatric fracture and bone health is uncertain.
Experiences from the UK and US revealed a reduction in incidence of paediatric fracture and referral to trauma centres during COVID-19, as well as an epidemiological shift in fracture characteristics,3–6 including the presenting age, mechanism of injury, location of injury, and anatomical locations. Nonetheless, there is a lack of local data and analysis on the effect of the pandemic on bone health of children in Hong Kong.
The primary objective of this study was to investigate the impact of the COVID-19 outbreak on the incidence and characteristics of paediatric fracture in Hong Kong, by dividing our patients into groups before and after the implementation of the above measures. The secondary objective was to determine the effect of home confinement on paediatric bone health, provide early public awareness and recommendation on preventive measures.
This retrospective study was carried out in New Territories West Cluster (NTWC) which accounted for nearly 1.2 million of population in Hong Kong. 7 Paediatric orthopaedics service was available in both Tuen Mun Hospital (TMH) and Pok Oi Hospital (POH) under NTWC with dedicated paediatric orthopaedic departments led by consultant and attending surgeons. These two hospitals represented specialist tertiary centres for paediatric orthopaedic trauma.
Methods
Data were accessed through the Clinical Data Analysis and Reporting System (CDARS). All patients with paediatric fracture aged 3–17 years old who were emergently or clinically admitted to the Orthopaedics and Traumatology Department of New Territories West Cluster (NTWC) hospitals were recruited. Acute orthopaedic trauma cases included fracture of the upper limbs, lower limbs, clavicles, vertebra, and pelvis.
The study period was from the start of the class suspension announced by the Education Bureau till March 2021 when face-to-face classes, on-campus activities, and extra-curricular activities were gradually resumed. Patients who were admitted from 1st February 2020 till 4th March 2021 in the Hospital Authority (HA) hospitals within NTWC cluster of Hong Kong were recruited as the study group, and will be referred to the “COVID” cohort in the rest of this article. The control group consisted of all patients admitted one year before the study period i.e., 1st February 2019 till 31st January 2020, and will be referred to the “pre-COVID” cohort.
We excluded any patients above 18 years old and under 3 years old. Non-accidental injury (NAI), pathological fracture, tuft fracture of fingers, toes fracture related to crush injury, and those with poorly documented trauma histories were excluded. It was summarized in Chart 1.
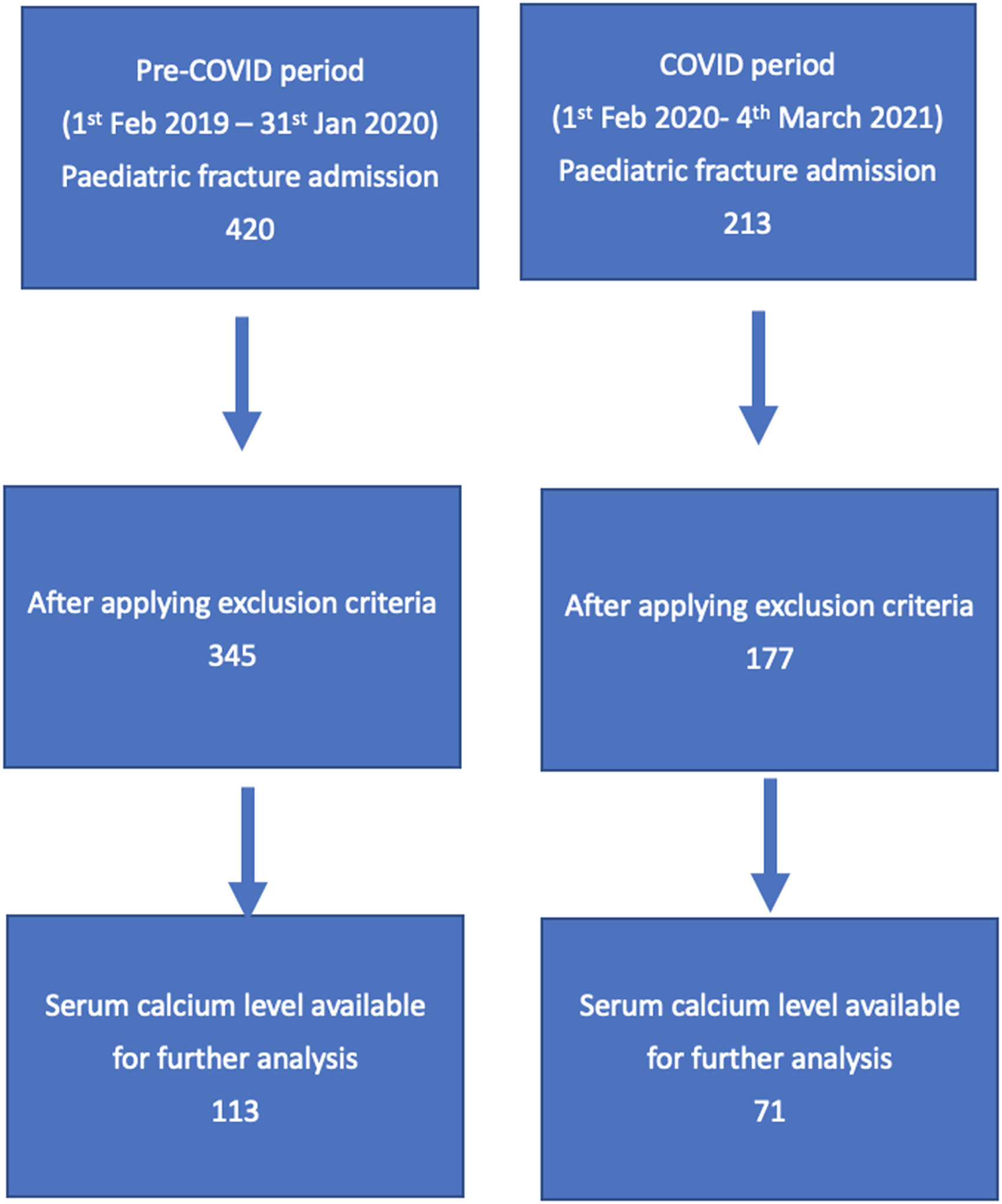
Number of patients recruited in pre-COVID 2019–2020 period (control group) and COVID 2020–2021 period (study group).
Demographics including age, sex, past health, body weight and height, body mass index (BMI) were recorded for all patients. Injury characteristics including the anatomical location, energy of injury, and mechanism of injury were also obtained. Mechanism of injury was categorised into level ground fall, fall from height (< 1 metre, > 1 metre), road traffic accidents (RTA), sports, injury related to body-powered vehicles (such as bicycle/scooter/roller-skating/rollerblading/skateboarding) and others (for injury outside aforementioned mechanisms). Energy of injury was divided into low energy injury, defined by level ground fall or mechanisms that involved equivalent magnitude; and high energy injury, included fall from height, road traffic accidents, sports, injury related to body-powered vehicles, or other mechanisms that involved equivalent magnitude. Fracture management, either by conservative or operative intervention, was documented. Serum calcium level, if measured during hospitalization, was also recorded as an indirect parameter of bone health measurement.
All data were anonymised and verified by two authors separately for accuracy and avoidance of bias. Shapiro–Wilk test was conducted for normality of individual data, which determined whether the data ought to be treated non-parametrically or parametrically. Mann-Whitney U test was used for non-parametric numeric data. The median age, BMI, and calcium level were calclulated. Chi-square test or Fisher's exact test was used to compare the groups for categorical variables as appropriate. All differences were considered to be significant if p value was < 0.05. All analyses were performed using R Statistical Software (v4.0.5; R Core Team 2021).
There were no ethical objections. Both TMH and POH centres gave permission for the use of the data. This study was approved by the Research Ethics Committee of NTWC and was not subjected to further ethical review. All patient details remained concealed. All information was stored on NTWC encrypted servers. This study received no funding. The authors have no conflict of interests to declare.
Results
In total, 522 patients were recruited into our study based on our inclusion and exclusion criteria. The number of paediatric patient admissions to NTWC hospitals due to fracture reduced by around 49% from 345 during pre-COVID period to 177 during the COVID period.
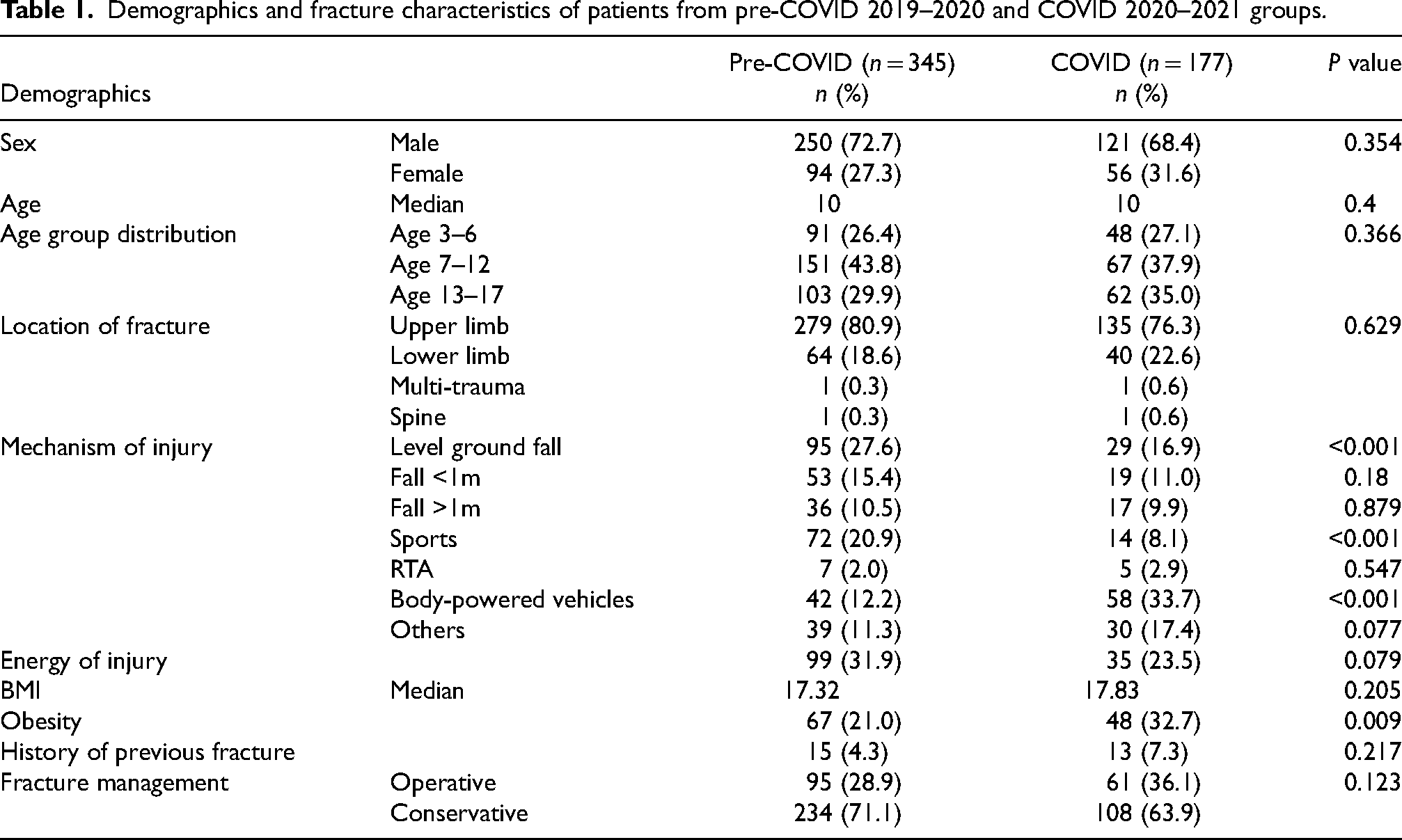
Demographic data such as age, sex, location of fractures, energy of injury, any prior history of fracture were comparable in the two groups. There was no statistically significant difference in the proportion of patients requiring operative treatment during the pre-COVID and COVID periods (Table 1).
Demographics and fracture characteristics of patients from pre-COVID 2019–2020 and COVID 2020–2021 groups.
Largest proportion of patients was from age 7–12, followed by age 13–17, then age 3–6 in both years. There is no significant difference in the age group distribution between pre-COVID and COVID periods (Chart 2).
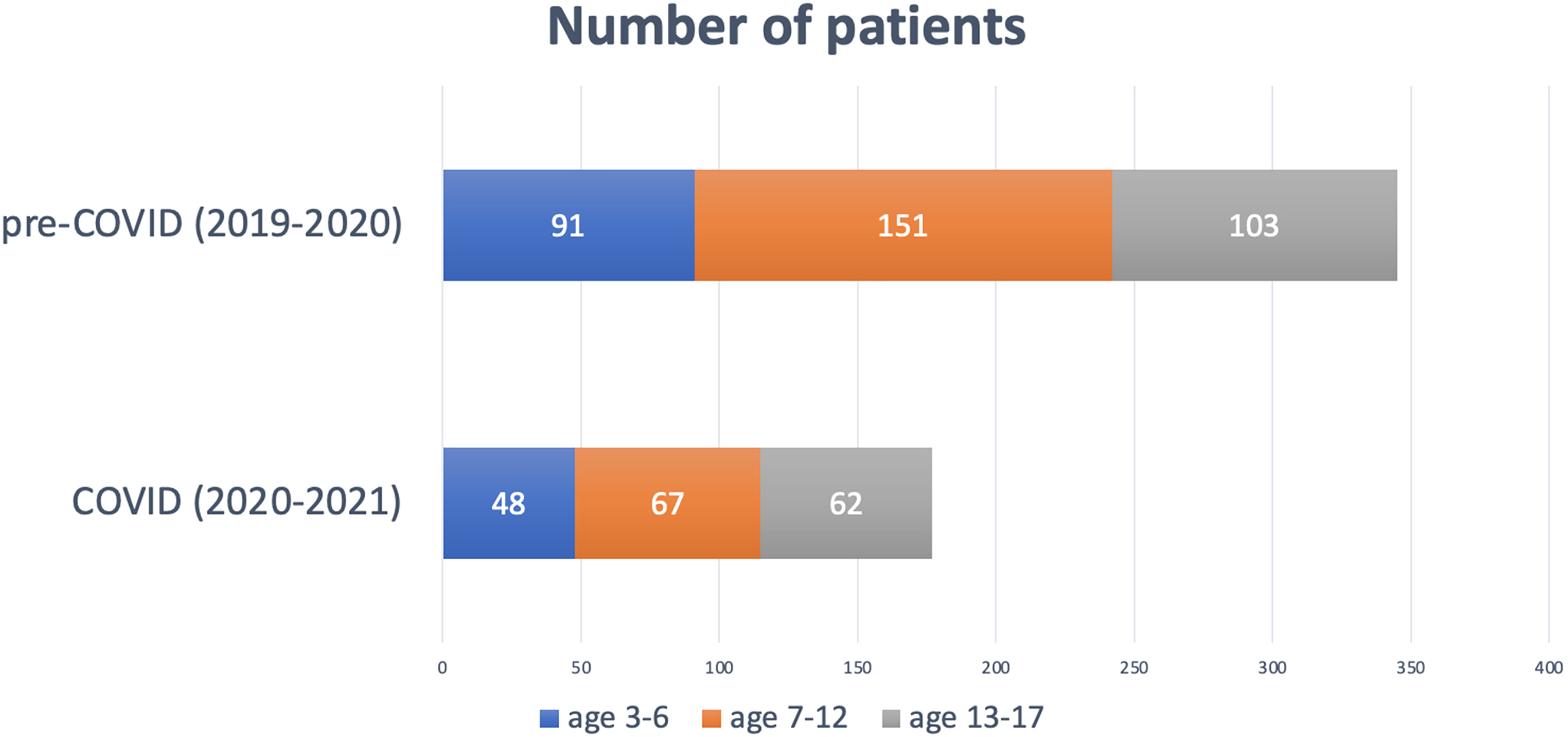
Distribution of patient age group during pre-COVID 2019–2020 and COVID 2020–2021.
During COVID-19 outbreak, injuries related to body-powered vehicles became the commonest cause of injury. Also, the percentage of patients resulting from this type of injury was higher (p < 0.001) during COVID (33.7%, n = 58) when compared to pre-COVID period (12.2%, n = 42). Meanwhile, level ground fall injury was the leading cause of fracture admissions in the pre-COVID period (27.6%, n = 95), but the proportion of this injury was significantly reduced (p < 0.001) during COVID period (16.9%, n = 29). Sports-related injury, being the second commonest injury mechanism in the pre-COVID period (20.9%, n = 72), also demonstrated a statistically significant drop (p < 0.001) during the COVID period (8.1%, n = 14). Other mechanisms of injury, including fall from < 1 metre, fall from >1 metre and RTA did not show any statistically significant difference between the two periods (Chart 3).
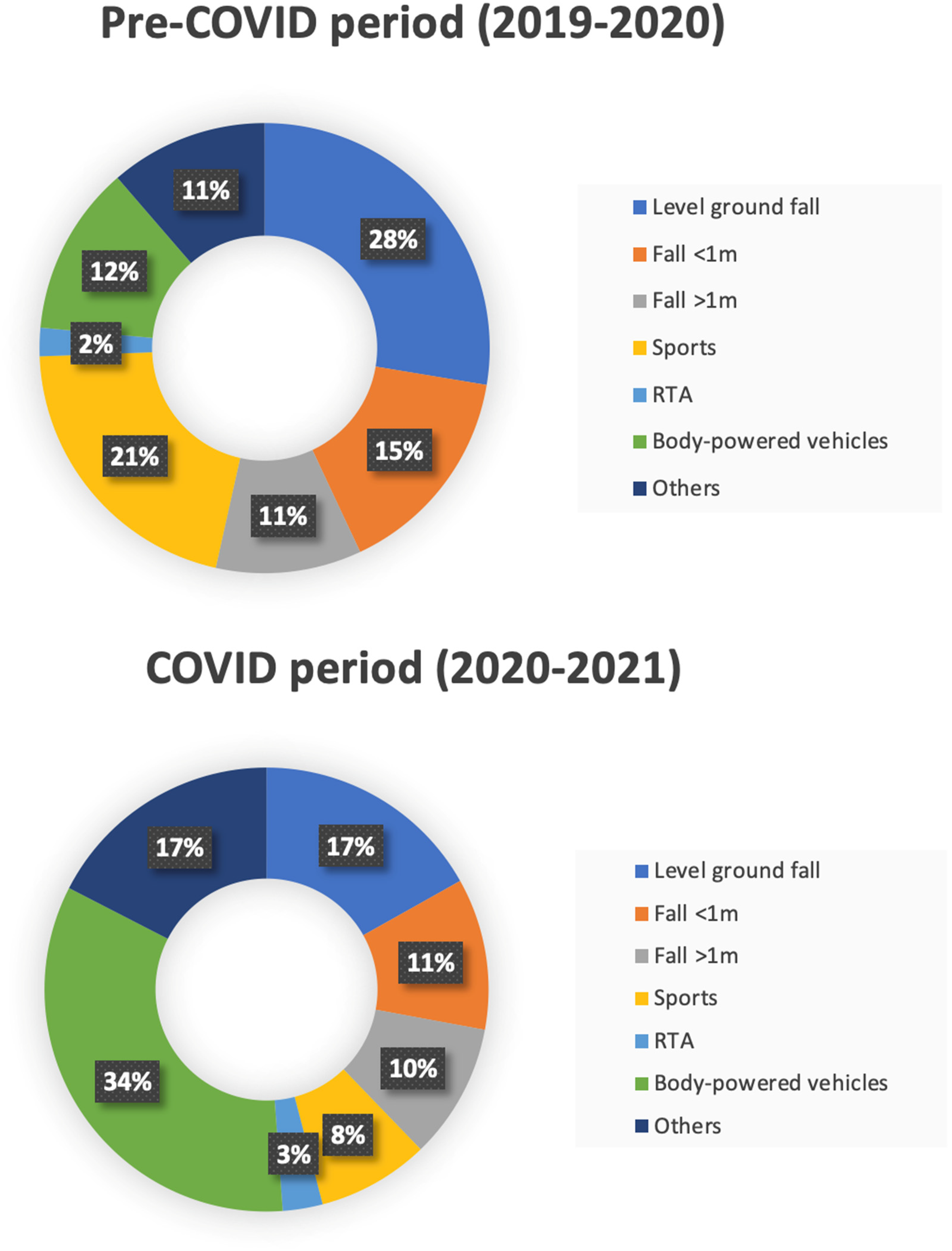
Distribution of mechanism of injury during pre-COVID 2019–2020 and COVID 2020–2021.
BMI was calculated by formula BMI = kg/m2 using a person's height (m) and weight (kg). Albeit not statistically significant (p = 0.205), the average BMI during COVID period (median = 17.83) was observed to be higher than pre-COVID period (median = 17.32).
According to the 1993 territory wide growth survey published by Leung et al. 8 of The Chinese University of Hong Kong, obesity is defined and generally endorsed in Hong Kong as weight greater than 120% of median weight-for-height. The percentage of patients who were obese increased significantly (p = 0.009) during the COVID period (32.7%, n = 48) compared to pre-COVID period (21.0%, n = 67).
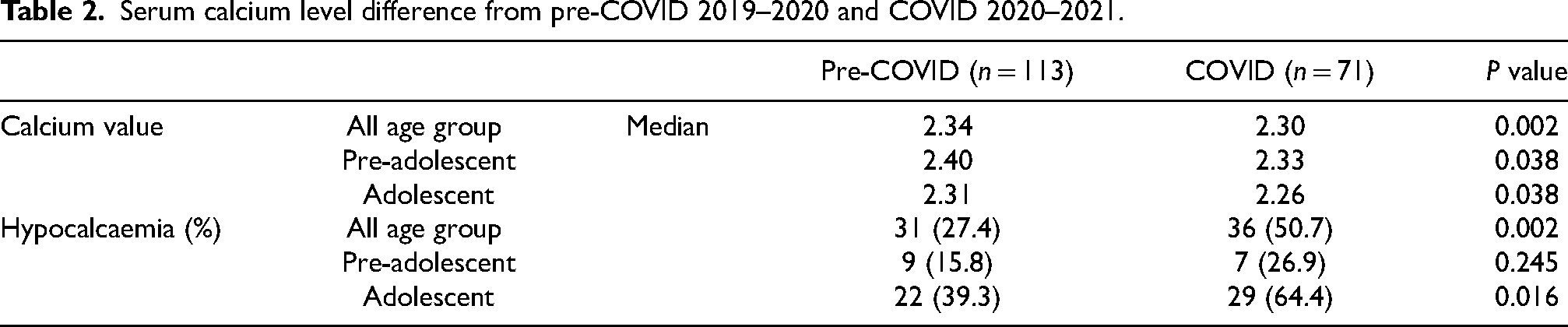
The proportion of patients with hypocalcaemia (with reference to age-appropriate interval) was found to be higher in the study group during COVID period (50.7%, n = 36) than pre-COVID period (27.4%, n = 31), which was statistically significant (p = 0.002). The mean serum calcium level was also found to be significantly lower (p = 0.002) during the study period. Further subgroup analysis was performed by categorizing patients into adolescent (age 13–17 years old) and pre-adolescent (age 3–12 years old) groups. Both groups showed a significantly lower mean serum calcium level during COVID period. A higher percentage of adolescents had hypocalcaemia during COVID period (p = 0.016) (Table 2).
Serum calcium level difference from pre-COVID 2019–2020 and COVID 2020–2021.
Discussion
As a result of the COVID-19 pandemic and related anti-epidemic measures including schools and sports venue closure, changes in paediatric fracture epidemiology, injury pattern and bone health were expected. We found a nearly 50% reduction in hospital admissions to our cluster due to paediatric fracture. This finding was supported by another local epidemiological study of Wong et al. 9 in 2020 showing up to 59% reduction in paediatric and adolescent admissions during COVID period. Similar drop in acute paediatric orthopaedic cases was observed in other countries, ranging from 33% to 81%.6,10 We postulated that the reduced fracture incidence was attributed to the prohibition of physical and outdoor activities in the year of pandemic. The mass closure of schools, parks, playgrounds and sports venues explained the decrease in level ground fall (27.6% pre-COVID period vs 16.9% COVID period) as children had less chance to run around and get injured. The decline in level ground fall injuries could also be related to altered parents’ behaviour. Sugand et al. 5 suggested that parents might be more reserved about attending emergency departments or seeking medical attention due to worries about contracting the COVID-19 virus in hospital. They might attempt to treat injuries from low energy fall conservatively at home.
Before the pandemic, sports were the second commonest cause of injury among patients presented with fractures. We observed a significant drop during the COVID period (20.9% vs 8.1%), which likely resulted from the suspension of sports events at school including physical education (PE) lessons, team sports practices, and closure of sports venues after the implementation of social distancing measures. Bram et al., 3 Baxter el al., 6 and Sugand et al. 5 had demonstrated similar findings. They also raised concerns on possible sedentary lifestyle that children might have during the COVID-19 pandemic.
Regarding the injury mechanism, we did observe an interesting phenomenon with significant increase in the percentage of injuries related to body-powered vehicles (12.2% pre-COVID period vs 33.7% COVID period). We believed that it was related to the difference in social distancing approach and infection control measures between Hong Kong and other countries. Even during the toughest period, whole-city lockdown never truly happened in Hong Kong. Our residents were still allowed to leave their home for work and pursue daily activities despite the closure of schools, playgrounds, and sports venues. In order to substitute for the regularly performed sports, cycling and roller-skating-related activities became the preferred choice of entertainment and physical activities, given that limited options were available. It involved less social interaction and disease transmission. Therefore, it was regarded as a safer type of outdoor activity from social hygiene and personal protection point of view. We proposed that the shift from team sports to individualised outdoor activities like cycling and roller-skating during the pandemic period was the main reason for the change in patterns of injury mechanism for paediatric fractures. Similar rise in trend of body-powered vehicles related injuries was also observed in the UK, US, and Italy.3,4,10 In September 2020, there was a newly introduced 11-km long cycling path “New Territories cycle track network” 11 in the communities within the service district of our cluster of hospitals. We believed that this might also potentiate the climb in injuries related to cycling, particularly during the COVID period being studied.
It was noted that a significantly higher proportion of patients from the COVID-19 pandemic year presented with obesity, and higher average BMI albeit statistically insignificant. We proposed that it could be a consequence of scarce physical activities and sedentary lifestyle after the school and sports venue closure policy. Rundle et al. 12 suggested that the surge in screen time and sedentary activities were expected to expand under social distancing orders. He further suggested that this had the largest impact on urban children who did not have access to safe, accessible outdoor spaces where they could maintain social distance. Living in Hong Kong, one of the most urban and densely populated countries in the world, 13 most of our younger population relied heavily on school-based programs or extra-curricular activities for physical exercise. Following the conversion of physical classes to digital online teaching, students were confined to home and limited outdoor space. We worried that this trend might affect children's general health particularly bone health in the long run. Indoor physical exercise should be promoted in the critical period and public awareness should be raised on the impact of behavioural and lifestyle change on potential health challenges.
We observed a raising trend in the proportion of patients presented with hypocalcaemia in the pandemic year among those required hospital admission for fracture management. Although not all paediatric fracture patients had their serum calcium level checked during admission and therefore may not truly reflect the whole population in our cluster and in Hong Kong, it still alerts us on the possible consequence of anti-epidemic measure on children's bone health. It was well accepted that hypocalcaemia could be associated with lack of physical activities,14–16 obesity 17 and reduced sunlight exposure due to decrease in outdoor activities. A prospective study by Ivuškāns et al. 17 also showed that sedentary time did have a negative influence on bone mineral parameters in peripubertal boys. In our study, the hypocalcaemia trend was more pronounced in the secondary school children than in the younger age group. It could be explained by the fact that adolescents were more engaged in outdoor activities and sports events compared with other age groups. Therefore, they were more susceptible to the consequence of lack of physical activities and sunlight exposure, leading to long term bone health problems. Mirsa et al. 18 suggested that a mild hypocalcaemia state can represent a subclinical or early stage of nutritional rickets preceding skeletal deformities in a later stage. Vitamin D deficiency will also increase the risk of paediatric fractures. 19 If left untreated, it may result in bone pain and deformity, fatigue, motor delay, proximal myopathy, and immune dysfunction in the worst-case scenario.
There are some pitfalls in our study. Firstly, this retrospective study led to challenges in retrieval of data with particular attention to bone health related factors such as amount of calcium intake, frequency and duration of physical activities, and duration of sunlight exposure. Serum calcium level was not routinely ordered by attending physicians during hospital admission. Only around 35% of the studied population had available serum calcium value. As a result, the subgroup analysis of the association of paediatric fracture with hypocalcaemia might not truly reflect the whole study population. Besides, other objective measures of bone mineral density, bone biochemical markers, and vitamin D level were not included in our study. Finally, this study was carried out in two hospitals within the same cluster, representing around 15% of the Hong Kong population. The study result may not truly reflect the real impact of COVID-19 outbreak on other cluster orthopaedic hospitals in Hong Kong.
Nevertheless, to the best of our knowledge, this is the first study on the impact of COVID-19 pandemic on paediatric fracture epidemiology in Hong Kong, and more importantly its long-term effect on public health issue. Despite noticing a significant reduction in paediatric fracture case admission, it does not imply the improvement of children's bone health in our locality. Instead, the observation of hypocalcaemia trend in our admitted cases during pandemic period reflects the negative influence of the pandemic and the related anti-epidemic measures on our children. As we may face another wave of pandemic of COVID-19 or related mutated virus, or even of another new virus in the future, regional wide study is required to further analyse the trend and review the impact on pandemic on paediatric fracture and bone health.
Conclusion
This study reflects the effect of early strike of pandemic at a tertiary trauma centre with paediatric orthopaedics service in Hong Kong. It reveals potential bone health issues in our younger population during the pandemic year, which deserves more attention from paediatric orthopaedic surgeons, paediatricians, and parents in Hong Kong, and in cities with similar characteristics. Decrease in outdoor activities, sports, and increase in obesity during the pandemic as a result of the social distancing measures is a concern. In the long run, preventive measures such as promoting home exercise, increasing dietary consumption of vitamin D and calcium as supplementation, could be considered at the time of pandemic when children are less exposed to outdoor and sports activities. Schools should also encourage students to do physical activities at home through online class and teaching. Parents are recommended to perform sports and outdoor activities with their children while maintaining vigilance against the virus. Our study also identified an epidemiological shift in paediatric fracture causes in the COVID period. Regarding the result, we would like to emphasize on the importance of proper precaution and fall protection during the use of body-powered vehicles such as cycling and roller-skating. Children should be supervised while doing such sports in order to avoid injuries and fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.