
Abstract
Background
Fragility hip fracture has become a major health burden to the healthcare systems all around the world with the ageing population. United Nations population study showed that the worldwide share of the elderly population aged 65 or above was projected to further increase with time, rising from 10% in 2022 to 16% in 2050. This group of the population is prone to fragility fractures including hip fractures. Previous studies showed increased morbidity 1 and mortality 2 among these patients with fragility hip fractures, which caused detrimental effects on their quality of life.
Surgery remains as the mainstay treatment option for fragility hip fracture patients, while non-operative treatment is adopted in around 3%–4% of cases with high peri-operative risks. 3 Non-operative treatment mainly aims for pain control such as oral analgesics and skeletal traction for splinting of fracture. A prolonged period of time is usually required to achieve pain control and patients are likely to have prolonged immobilization which leads to morbidities and poses a challenge to patient care.
In recent years, chemical hip neurolysis has emerged as an alternative treatment option for fragility hip fracture patients with high operative risks, aiming to improve pain control and aid patient care. Recent studies4–6 investigated on the clinical outcome of chemical hip neurolysis, which showed good pain relief after the procedure and a good safety profile.
This study aimed to compare the clinical outcome and mortality between the patients receiving chemical hip neurolysis and those adopting conservative treatment, as well as to investigate on the risk factors for mortality in patients receiving non-operative treatment in general.
Methods
This is a retrospective cohort study, with the patients screened retrospectively from the Clinical Data Analysis and Reporting System (CDARS) of the Hospital Authority of Hong Kong. Fragility hip fractures referred to hip fractures that had resulted from low-energy trauma such as a fall from a standing height.
Patients receiving chemical hip neurolysis for fragility hip fractures in a regional cluster of Hong Kong were identified as the intervention group (neurolysis group). The targets of the articular branches for the anterior hip capsule were the high and low branches of femoral nerve articular branches (FNABs), the accessory obturator nerve (AON) and the high and low branches of obturator nerve articular branch (ONAB). The targets for the superoposterior hip capsule were the articular branch of the superior gluteal nerve (SGN), the articular branch of nerve to quadratus femoris (NQF), the articular branch of sciatica nerve (SN) and the articular branch of the inferior gluteal nerve (IGN). A total of 5 mL local anaesthetic was injected into the bony surface between the anterior iliac spine and iliopubic eminence to block the FNAB high branch and AON, 3 mL to the iliopsoas plane to block the FNAB low branches, 1.5–2 mL to the inferomedial acetabulum to block the ONAB and 1–1.5 mL onto the superoposterior hip capsule underneath the piriformis to block the articular branches from SGN, NQF, SN and IGN. The injections were first done with 0.5% bupivacaine as a diagnostic block and a pre-treatment before neurolysis. If the diagnostic block was positive, absolute (100%) alcohol was used for chemical neurolysis in the same injection session. The ratio of the absolute alcohol and the local anaesthetic was at least 1:1 so that the resultant alcohol concentration was at least 50%. The patients with admission date between January 2015 and December 2019, diagnosis code of acute hip fracture (ICD-9 820.00, 820.02, 820.03, 820.09, 820.20, 820.21, 820.22 and 820.8) and procedure code of neurolysis (ICD-9 04.49) were included.
Patients receiving traditional conservative treatment for fragility hip fractures were identified as the control group (conservative group). The patients received oral analgesics for pain control. Unless contraindicated, the patients were administered oral paracetamol 1 g for 3 times a day with as required oral tramadol immediate release 50 mg 3–4 times a day. Traction would be applied in selected cases. Patients with admission date between January 2010 and December 2014, the above-mentioned diagnosis code of acute hip fracture and exclusion of procedure codes for operation (ICD-9 81.52, 51.51, 81.40, 79.15, 79.35 and 78.55) were included.
Exclusion criteria included patients with pathological fractures, transfer to hospitals in other clusters or private hospitals within one week of admission or discharged with acknowledgement of medical advice (DAMA). Patients meeting the exclusion criteria were excluded, and the remaining subjects were recruited into the study.
The clinical outcome in both groups of patients was compared. Primary outcomes included thirty-day and one-year mortality for all causes, which were analysed with a chi-square test. The secondary outcome included the length of in-patient stay for index admission, which was analysed with Mann-Whitney U-test. Thirty-day post-discharge emergency readmission rate and conversion rate from home care to old age home care were analysed with a chi-square test. The independent risk factors for mortality were identified using logistic regression models. Independent two-sample t-test and chi-square test were adopted to compare the demographic data between the two groups of patients.
All analyses were performed using IBM SPSS Statistics 29.0. The results were considered statistically significant if the p-value was <0.05. Ethical approval was obtained from the Research Ethics Committee, and consent from subjects was waived. The study was performed in line with the principles outlined in the Declaration of Helsinki.
Results
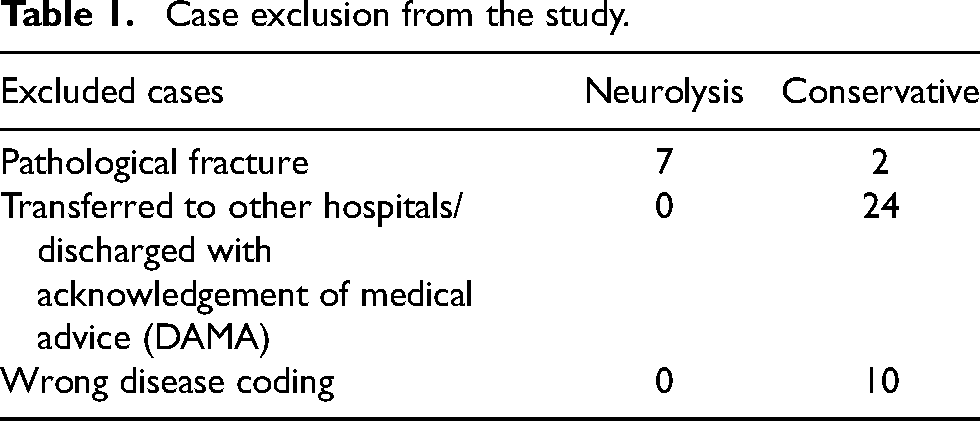
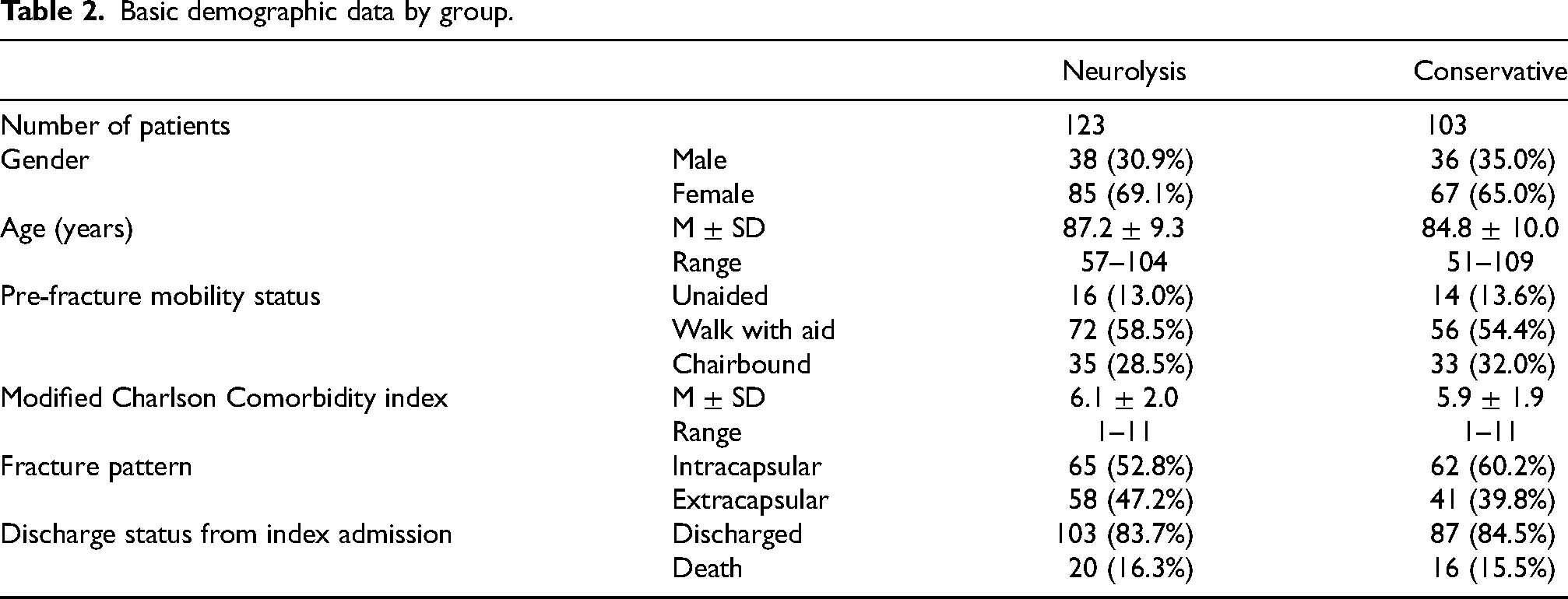
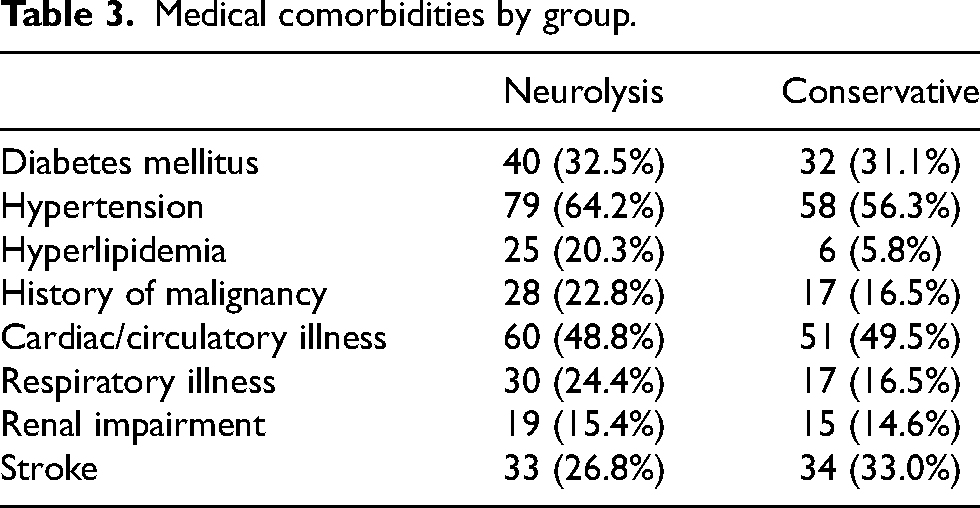
A total of 130 patients in the neurolysis group and 139 patients in the conservative group were identified during the study period. Seven patients and 36 patients were excluded from the study due to the exclusion criteria in neurolysis and conservative groups, respectively (Table 1). As a result, 123 patients in the neurolysis group and 103 patients in the conservative group were included for analysis. The basic demographic data of the patients in neurolysis and conservative groups is shown in Table 2. Hypertension and cardiac diseases were the most common comorbidities in both groups of patients (Table 3). Age (p = 0.07) and gender (p = 0.52) did not differ significantly between neurolysis and conservative groups, and there was no significant difference between the Modified Charlson score (p = 0.55) of the two groups of patients.
Case exclusion from the study.
Basic demographic data by group.
Medical comorbidities by group.
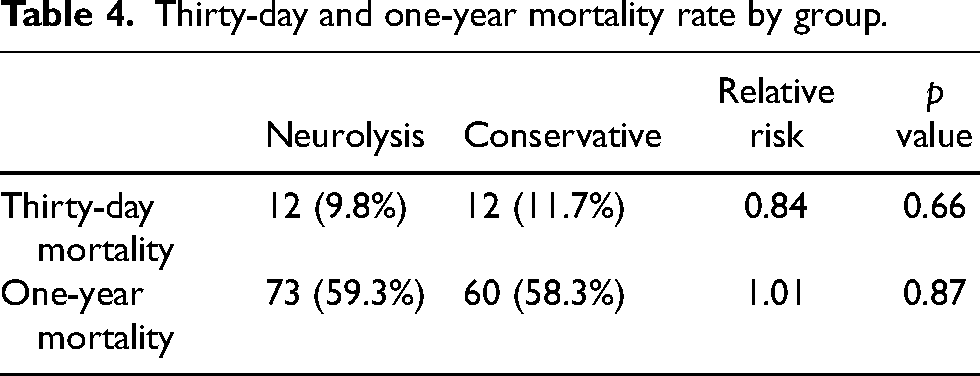
The one-year mortality in the neurolysis group and conservative group were 59.3% and 58.3%, respectively. There was no statistical difference in thirty-day (p = 0.66) and one-year mortality (p = 0.87) between the two groups of patients (Table 4).
Thirty-day and one-year mortality rate by group.
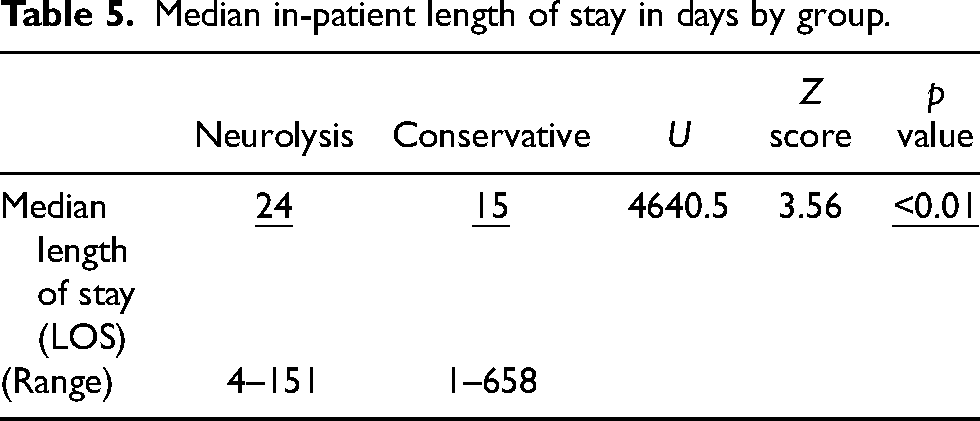
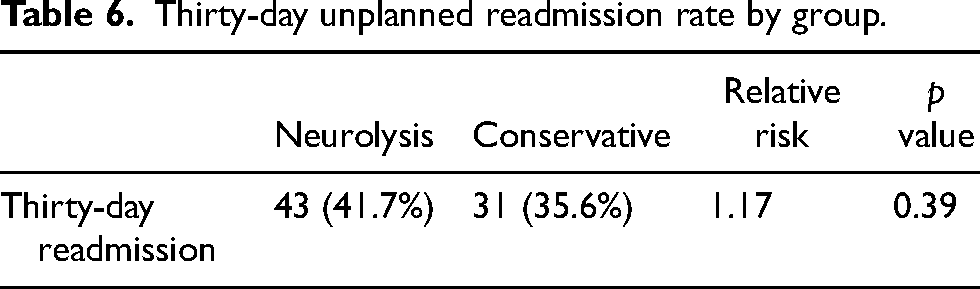
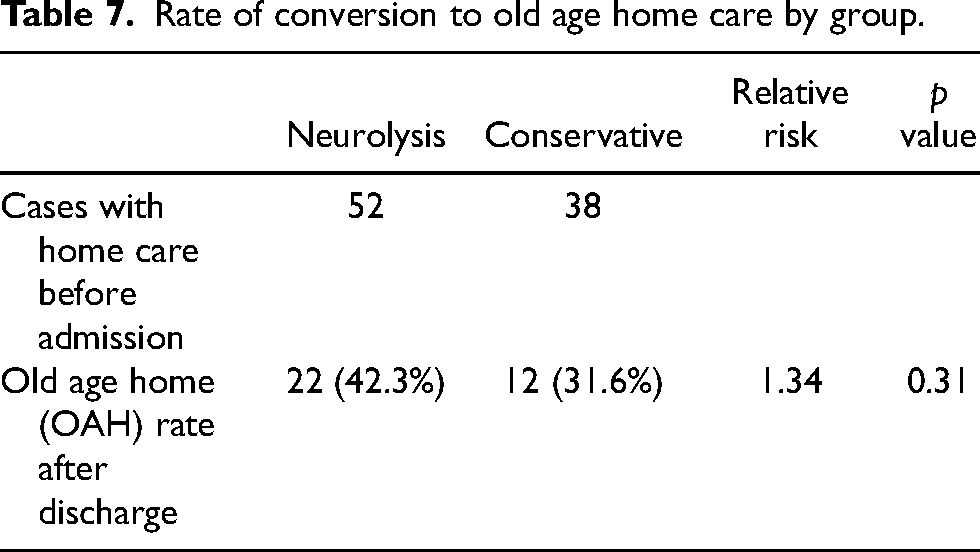
The median in-patient length of stay (LOS) for the neurolysis group was 24 days, and the median in-patient LOS for the conservative group was 15 days. The median waiting time for neurolysis was 7 days, and the median LOS post-neurolysis was 12 days. There was a longer LOS for the neurolysis group compared with the conservative group (p < 0.01) (Table 5). There was no significant difference in the thirty-day readmission rate through the Accident and Emergency Department and conversion rate from home care to old age home (OAH) care between the two groups of patients (Tables 6 and 7).
Median in-patient length of stay in days by group.
Thirty-day unplanned readmission rate by group.
Rate of conversion to old age home care by group.
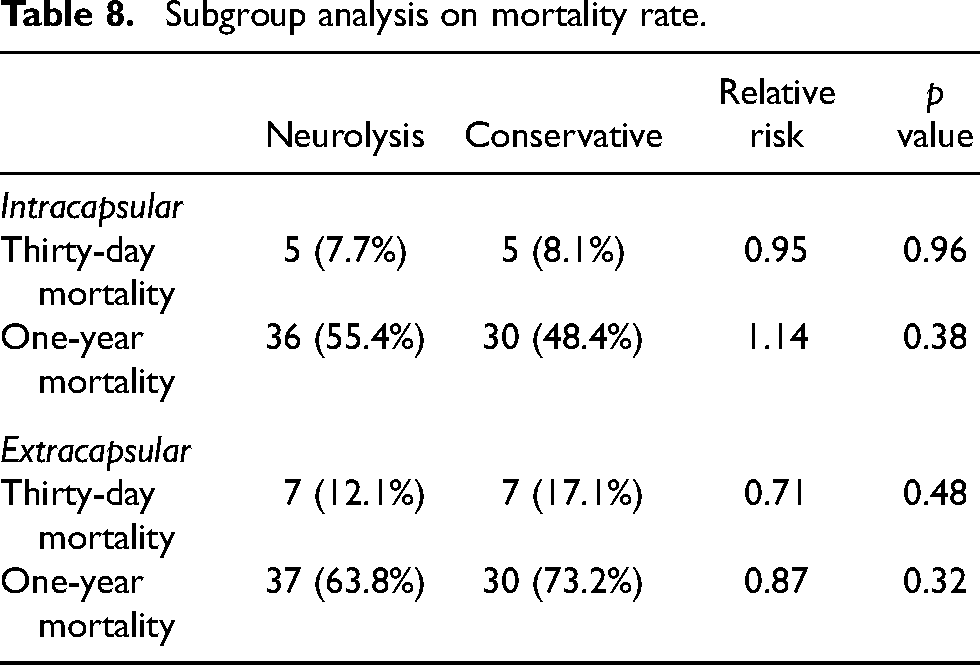
Subgroup analysis of the mortality rate was performed over intracapsular and extracapsular fracture patterns. Results showed that there was no significant difference between neurolysis and conservative groups in thirty-day and one-year mortality for both intracapsular and extracapsular fracture subgroups (Table 8).
Subgroup analysis on mortality rate.
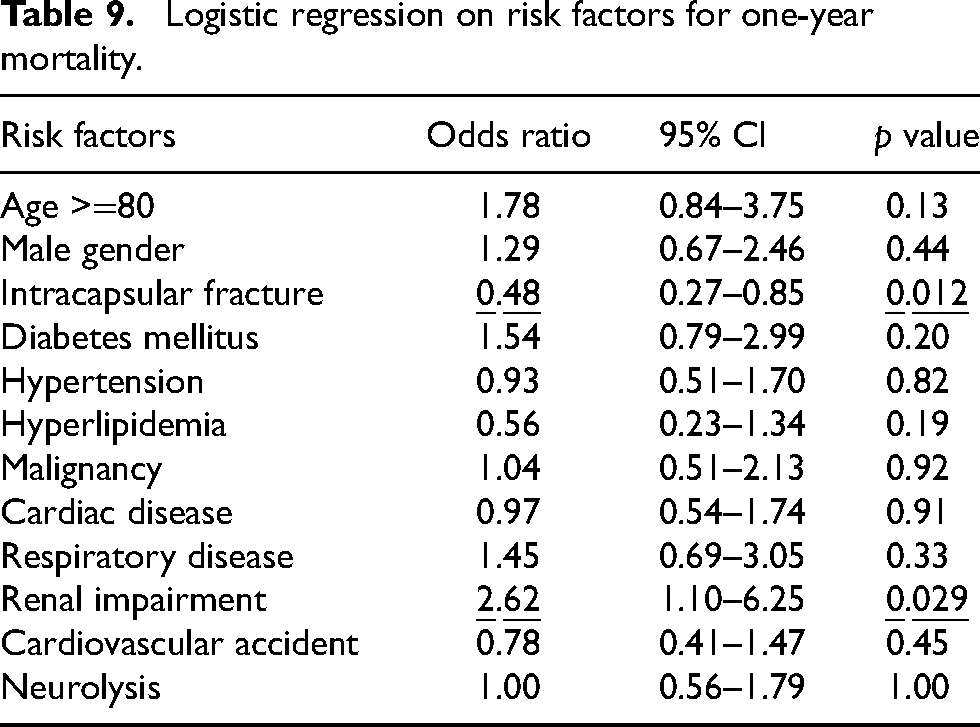
Logistic regression was performed to identify the independent risk factors for one-year mortality among all patients, with neurolysis intervention included as one of the factors. Renal impairment was a strong risk factor for one-year mortality, with an odds ratio of 2.62 (95% CI: 1.10–6.25, p = 0.029). On the other hand, intracapsular fracture was shown to be a protective factor, with significantly lower one-year mortality comparing with extracapsular fracture (OR 0.48, 95% CI: 0.27–0.85, p = 0.012). Other factors did not show a significant effect on the one-year mortality rate (Table 9).
Logistic regression on risk factors for one-year mortality.
Discussion
The current role of neurolysis in fragility hip fractures is an alternative treatment option to surgical intervention, aiming to improve pain control and aid patient care, reducing the period of prolonged immobilization and the associated morbidities such as pressure sore and chest infections and mortality. In this study, the one-year mortality rate for the neurolysis group and conservative group were 59.3% and 58.3%, respectively, which was comparable to the results in another study of a Chinese-based fragility fracture registry. 7 The results from this study suggested that neurolysis was not inferior to previous practice of conservative management in terms of mortality.
The results from this study showed that the neurolysis group had a longer median length of stay during index admission when compared to the conservative group. This may partly be attributable to the waiting time for neurolysis, as the median waiting time was 7 days for the neurolysis group and the median length of stay post-neurolysis was 12 days only, whereas the median LOS for the conservative group was 15 days. Early detection and screening for cases with high surgical risks may facilitate prompt inter-departmental liaison and collaboration with anaesthesia and pain team colleagues. Another possible cause would be the variation of management approach in the conservative group, with early discharge of some patients once after deciding not for surgery.
Logistic regression showed intracapsular fracture pattern as a protective factor for mortality as compared to extracapsular fractures. This echoed with the existing evidence 8 that extracapsular hip fractures were associated with higher mortality and morbidity. On the other hand, patients with renal impairment were shown to be a risk factor for mortality. These results may allow healthcare professionals to pay extra attention to these patients during hospital stays and follow-up sessions.
There are limitations in this study. Pain control was one of the treatment goals in neurolysis, but quantification of pain control such as the use of a visual analog scale (VAS) remained difficult in elderly patients as some of the patients either suffered from cognitive impairment or were non-communicable. The morbidity and assessments on psychological outcomes and quality of life were also difficult to assess. For instance, some patients may be able to sit up and perform self-feeding within a few days after neurolysis, which is beneficial to the quality of life and psychological health. Mortality of the patients in other countries after discharge was not recorded. Besides, this study focused on a single regional cluster, and further large-scale studies may be warranted for the generalization of the results.
Conclusion
Chemical hip neurolysis for inoperable fragility hip fracture patients was not inferior to conservative management in terms of one-year mortality, while total in-patient length of stay was increased taking waiting time for neurolysis into consideration. Intracapsular hip fracture and renal impairment were identified as protective and risk factors for mortality respectively. Further studies and collaboration with pain team colleagues may be warranted to evaluate the functional outcome of neurolysis and compare it with surgically treated patients with similar medical comorbidities.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the NTWC Clinical Research Governance Committee for the advice on the study design and data analysis.
Data availability statement
Raw data were generated from the Clinical Data Analysis and Reporting System (CDARS) of the Hospital Authority of Hong Kong. Derived data supporting the findings of the study are available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical standards are in line with the local guidelines. The research was approved by the NTWC Cluster Research Ethical Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.