
Abstract
Introduction:
The growing impact of fragility hip fracture (FHF) on the healthcare system and the society has become a major concern worldwide. A unified multidisciplinary FHF pathway from admission to rehabilitation and back to community was established in 2015. The acute phase of the pathway was put into pilot in our hospital to evaluate the outcome.
Method:
A designated FHF team was established in our centre since January 2015. The FHF pathway was piloted since June 2015. Patients admitted with a hip fracture resulting from fall on standing height were included. Major outcome parameters were compared in three phases: (1) before FHF team and FHF pathway (January to December 2014), (2) after FHF team but before FHF pathway (January to May 2015) and (3) after FHF team and FHF pathway (June 2015 to May 2016).
Result:
In phases 1, 2 and 3, 631, 263 and 634 patients were included, respectively. From phases 1 to 3, the average key performance indicator (KPI) has improved from 49.2% to 65.8% to 70.0% significantly; average acute length of stay (days) has improved from 13.7 to 13.4 to 11.3 significantly; total surgical complication rates have improved from 6.2% to 7.6% to 5.8%. The 30-day mortality rate and the unplanned readmission rate (within 28 days) have remained below 2.7% and 2.2%, respectively.
Conclusions:
Implementation of an FHF pathway can form a multidisciplinary platform that can improve the standard of care and outcome for our FHF patients in terms of KPI and also length of stay.
New knowledge added by this study:
A newly designed and implemented fragility hip fracture pathway in our centre as a pilot with the results evaluated.
Implications for clinical practice or policy:
With the increasing elderly population in Hong Kong and globally, there is a need to design and implement a fragility hip fracture (FHF) pathway to improve the care and effectiveness for FHF patients.
Introduction
With an increasing ageing population, there is a growing impact of fragility hip fracture (FHF) on the healthcare system and the society as whole. It has become a major public health concern worldwide. According to the Japanese Health and Welfare Ministry Report, Hong Kong has the highest life expectancy in the world in 2015, with the mean age of 81.2 and 87.3 years for males and females, respectively. The number of FHF has been increasing and the projected annual incidence of geriatric hip fractures in 2040 will be more than 14,500, which is more than a threefold increase in a 30-year period from 2011 to 2040. 1 This increase will have considerable burden on the patients, their families, the healthcare system and the society in different aspects.
Between 2009 and 2015, there has been an increase from around 3500 to 5400 cases of FHF, respectively, in the public hospitals of the Hospital Authority (HA). The average length of stay was 11 days and a 5-year readmission rate was 7.78%. It is well-known that those patients who have already sustained a fracture are the ones who are at higher risk for further fracture leading to readmission. 2
Osteoporosis and more recently sarcopenia are associated with an increase in fragility fractures. 3 There has been a growing need to not only address the fracture management in FHF patients in the acute setting but also to prevent secondary fracture. Furthermore, the 1-year excess mortality rate ranged from 8.4% to 36% is seen in previous studies. 4 It is, therefore, increasingly important to utilize a multidisciplinary approach to provide a standardized and holistic care for this group of patients from admission to operation to rehabilitation, for secondary fall prevention, bone health management and for reintegration back to the community. 5
The blue book from the British Orthopaedic Association (BOA) 6 has set standards for surgeons to comply to improve the quality and outcomes of care and also reduce costs. They outlined six key standards involving a multidisciplinary approach, access to orthogeriatric medical support from the time of admission, early pressure management, bone health management and all medically fit patients should receive surgery within 48 h of admission and during normal working hours.
A cross-sectional survey concerning FHF patients admitted to six major hospitals in Hong Kong in the year 2012 lead by The Hong Kong Fragility Fracture Registries (FFR) Working group was performed. 7 Parts of the results were compared to the six BOA standard mentioned earlier. According to their results, only 60.5% of patients received surgery within 48 h from admission, over 65% of patients have no orthogeriatric medical support throughout the admission and over 75% of patients have not received any anti-resorptive therapy within the admission. The results were far from satisfactory when comparing to the BOA standard. In view of this, a unified multidisciplinary FHF pathway was established in 2015 by a multi-centred working group and was piloted in our centre. It was designed to meet the international standards as well as to provide multidisciplinary care from admission to early rehabilitation to secondary fracture prevention in the community.
Methods
A designated FHF team was established in our department since January 2015. The FHF team composed of a team coordinator who was a consultant, two associate consultants and two residents who were also involved in the care for polytrauma patients. The designated coordinator was responsible for interdisciplinary and intradisciplinary communication as well as operative session arrangement and allocation. The FHF team members were responsible for daily ward rounds, preoperative physical optimization, operation, postoperative care and discharge from the acute hospital. Dedicated daytime operative sessions were also specifically designated for FHF in the same period.
The FHF pathway was established and piloted in our department since June 2015. The key features of the pathway were (1) a designated coordinator, (2) multidisciplinary, (3) a standardized protocol, (4) a dedicated FHF team, (5) dedicated surgeons, (6) daytime operative sessions and (7) bone health management.
The standardized protocol for clinical documentation for the entire period of acute hospital management from admission to operation to discharge is shown in Figure 1. It aims for better patient management with less mistake and management deviation from our frontline medical and nursing staff. It also provides a multidisciplinary platform where orthopaedic surgeons, nursing staff, anaesthetists occupational therapists, physiotherapists, prosthetics and orthotics, speech therapists, social workers and dieticians can be involved and can communicate effectively in the acute phase of patient’s management. They can then continue to provide their care throughout the rehabilitation process to speed up recovery as well as educate the patient and their families for secondary fracture prevention.
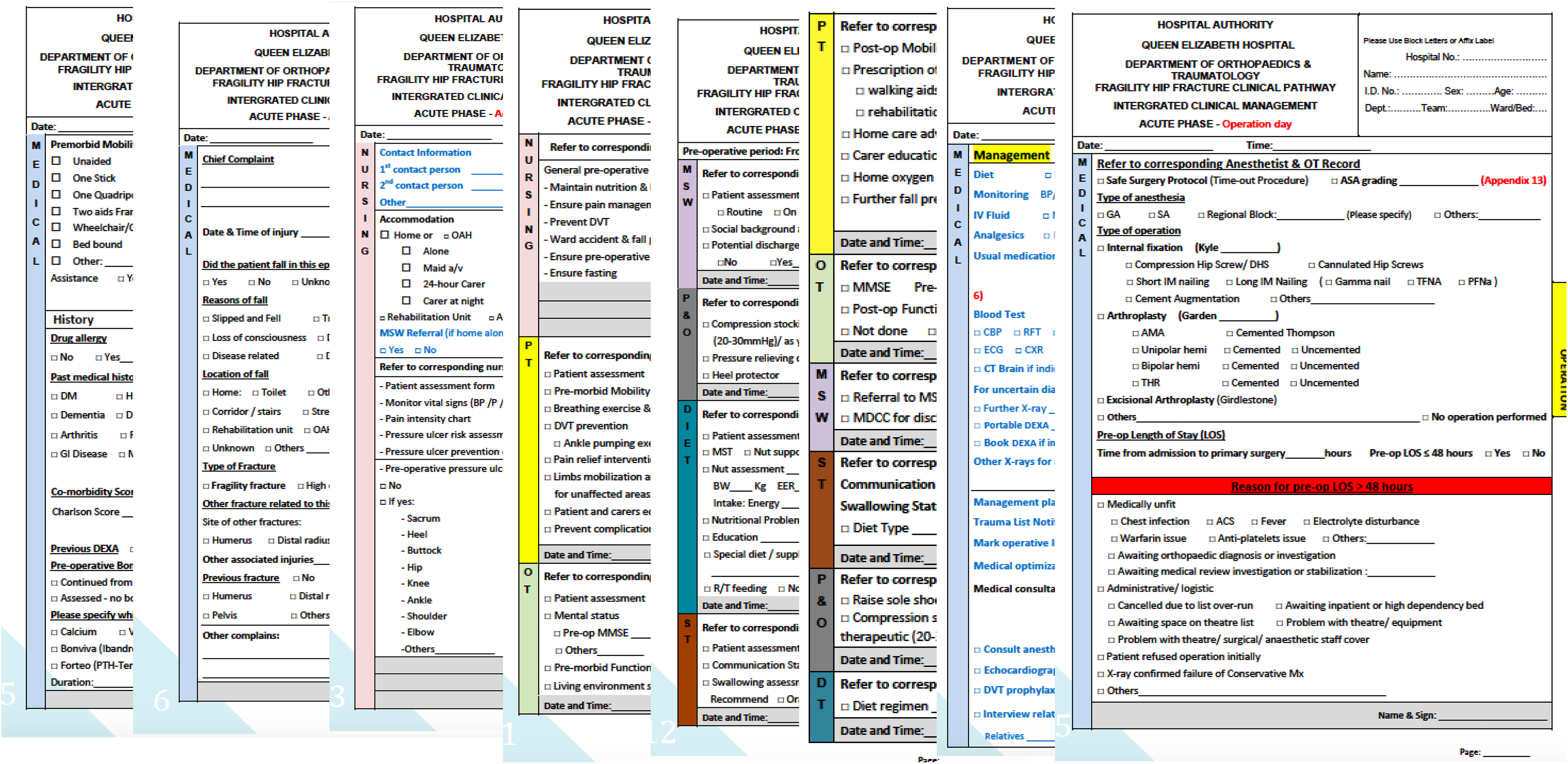
FHF pathway standardized protocol, established and piloted in our department since June 2015, serves as a multidisciplinary platform used for the entire acute hospital management from admission to operation to discharge. FHF: fragility hip fracture.
There have been three major phases in our management of FHF: phase 1: before the FHF team and FHF pathway were established (from January to December 2014); phase 2: after the FHF team but before FHF pathway were established (from January to May 2015); and phase 3: after the FHF team and FHF pathway were established (from June 2015 to May 2016). Since phase 2, there have been six sessions per week during day time designated for FHF surgeries.
All patients admitted with hip fractures resulting from a fall from standing height were included. The exclusion criteria included patients who had significant clinical variances such as complications requiring reoperation, readmission or severe medical complications, those with atypical or pathological fractures, those whom non-operative treatment was decided and those who were transferred out of public hospitals. Major outcome parameters were compared over the three phases, which included (1) the number of patients who received their operation within 2 days of admission, (2) the acute length of stay, (3) the 30-day mortality, (4) unplanned readmission within 28 days of discharge and (5) surgical complications.
For the statistical analysis, it was performed using SPSS Statistic Software Version 23 and differences were considered statistically significant at p < 0.05. Continuous variables such as age and acute length of stay were compared using the Student’s t-test, and the categorical variables such as gender, the number of patients receiving operation within 2 days, 30-day mortality, unplanned readmission and surgical complications were compared using the χ 2 test. To see whether the number of patients who received their operation within 2 days had any significant differences between the three phases, the data were analysed on a monthly basis to see whether it had reached the key performance indicator (that 70% of hip fracture patients received surgery within 2 days) for a certain month.
Result
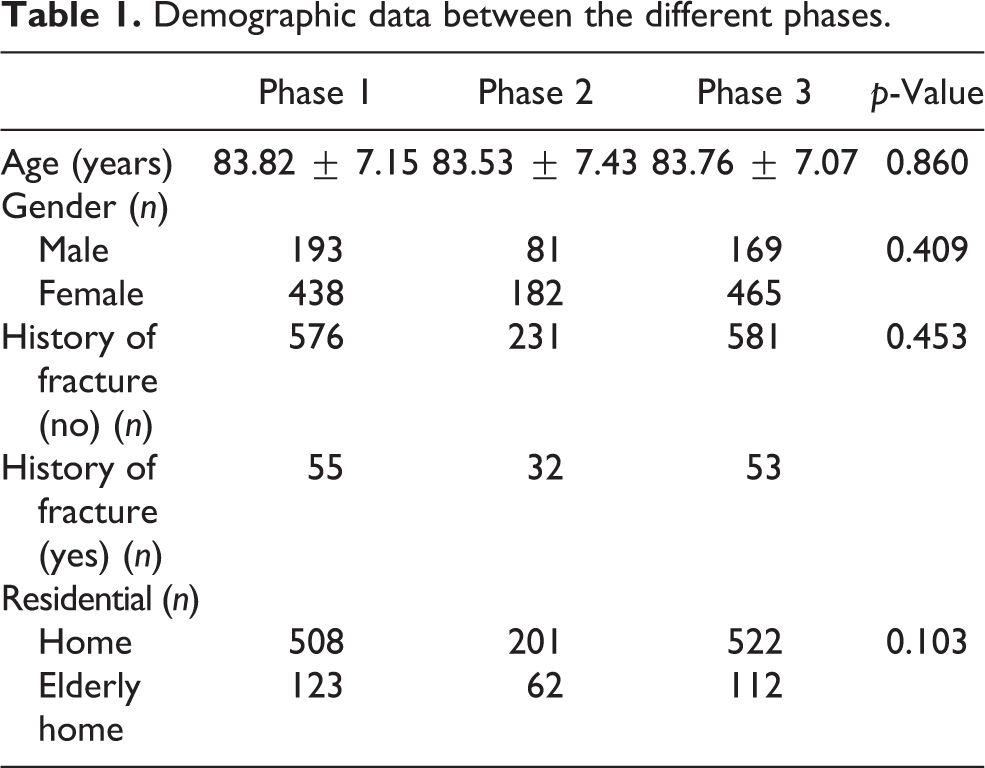
A total of 631, 263 and 634 patients were included in phases 1, 2 and 3, respectively. A total of 1528 patients were captured in the study period and the average age was 83.70 ± 7.19 years. Of the patients, 1085 were female and 443 were male, 1222 came from home and 306 came from an elderly care home. The demographic data were compared between the three phases and there was no significant difference between the phases in terms of age, gender, history of fracture and their place of residence before admission as seen in Table 1.
Demographic data between the different phases.
From phases 1 to 3, the average percentage of patients receiving operation within 2 days for their FHF has improved from 49.2% to 65.8% to 70.0% (p = 0.008), respectively, over the three phases as seen in Figure 2(a). By comparing phase 1 against phases 2 and 3 (p = 0.004) and similarly when comparing phases 1 and 2 against phase 3 (p = 0.004), there were significant differences. This shows that there is a gradual significant improvement in the number of patients receiving their operation within 2 days of admission with the introduction of the FHF team in phase 2 and then a further improvement in phase 3 with the implementation of the FHF pathway.
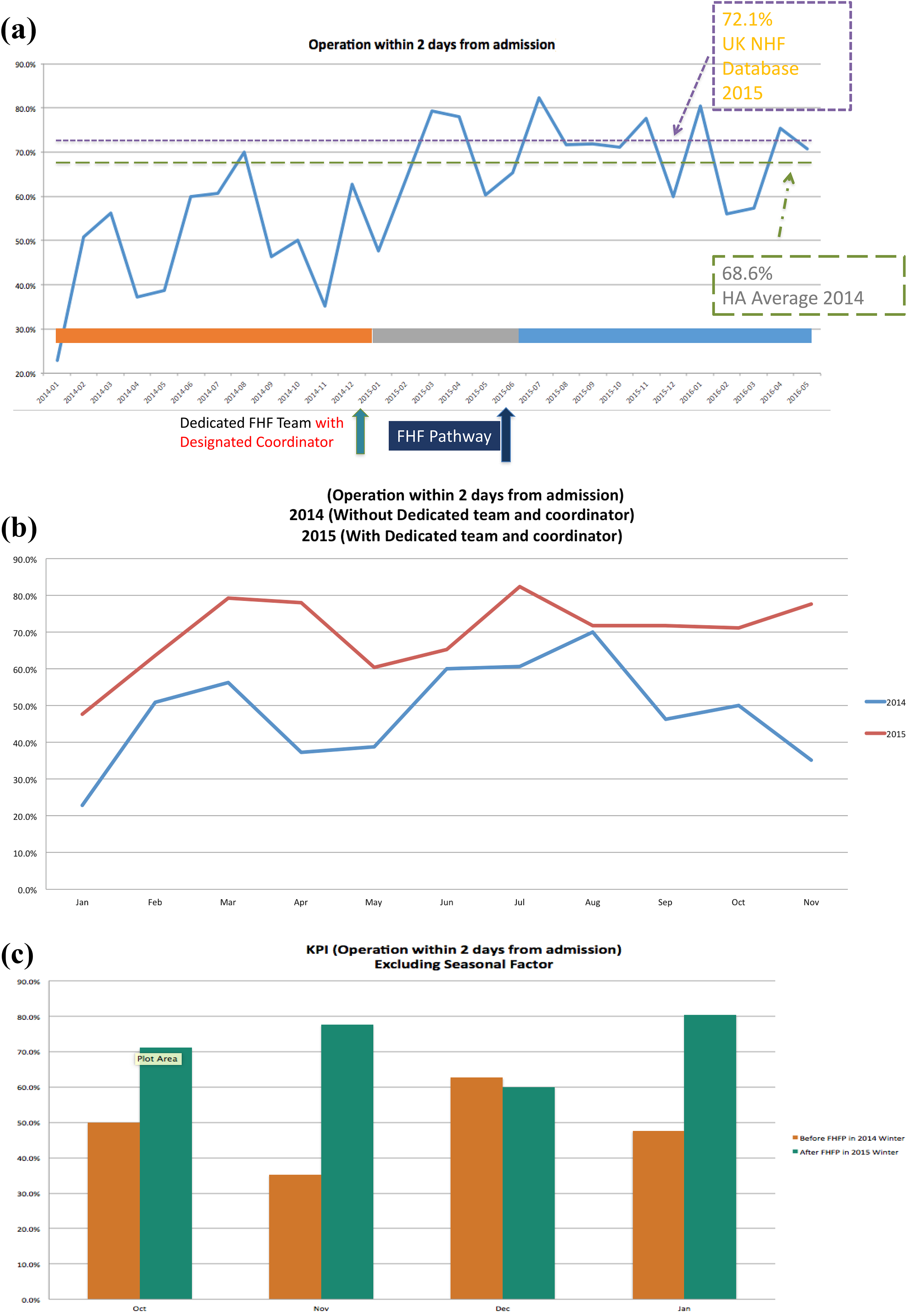
(a) From phases 1 to 3, the average percentage of patient receiving operation for their FHF has improved from 49.2% to 65.8% to 70.0%, respectively (p = 0.008). The results are also comparable to the national average from the NHFD from the United Kingdom, which had 72.1% of the FHF patients receiving their operation within 2 days of admission. (b) There is an improvement in the number of patients receiving their FHF operation after a dedicated team and coordinator was in place. (c) Seasonal variations also overcome: excluding seasonal variations, the number of patients who received their operation within 2 days was higher in phase 3. FHF: fragility hip fracture; NHFD: National Hip Fracture Database.
The results after the FHF pathway was in place are comparable with data from the National Hip Fracture Database (NHFD) 2015 from the United Kingdom. Their national average for FHF patients receiving their operations within 2 days of admission was 72.1%. It was also an improvement from the HA average of 68.6% in 2014 and an improvement from the data from the FFR working group average of 60.5%. Figure 2(c) also shows us that even excluding seasonal variations, the number of patients who received their operation within 2 days was higher in phase 3.
The average acute length of stay (days) has improved from 13.7 to 13.4 to 11.3 (p = 0.000), respectively, over the three phases. By comparing phase 1 against phases 2 and 3 (p = 0.016) and similarly when comparing phases 1 and 2 against phase 3 (p = 0.000), there were significant differences. The results show that with the implementation of the FHF team in phase 2, there was a significant reduction in the length of stay and a further significant reduction in the length of stay with the implantation of the FHF pathway in phase 3. The results are comparable with data from the UK NHFD 2015 and the HA average in 2014, 15.5 and 11.4 days, respectively (Figure 3).
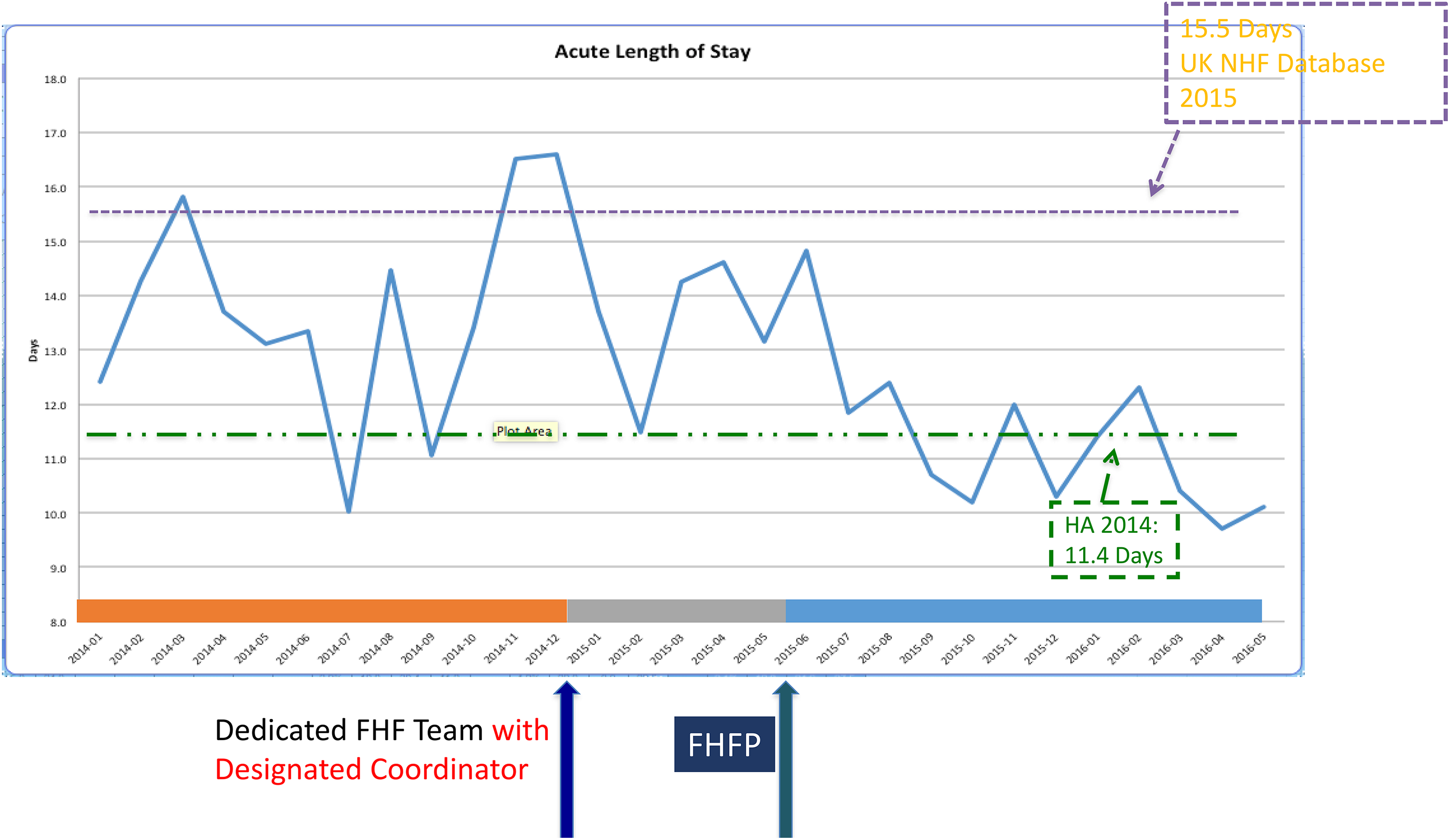
The acute length of stay has improved from 13.7 to 13.4 to 11.3, respectively, over the three phases. The results are comparable with data taken from the UK NHFD 2015 and the HA average in 2014, 15.5 and 11.4 days, respectively (p = 0.000). NHFD: National Hip Fracture Database; HA: Hospital Authority.
The total surgical complication rates have improved from 6.2% to 7.6% to 5.8% (p = 0.116), respectively (Figure 4). If we further break this down, we can see that towards the end of phase 3 from December 2015 to May 2016 after the FHF pathway had been running for 6 months, the total complication rate was at its lowest 3.74%. The complications showed an improving trend from phase 1 to phase 3. It is most evidently seen in the fixation failure rate which was 1.27% and 1.14%, respectively, in phases 1 and 2. This decreased to 0% in phase 3. For the other complications such as iatrogenic fracture, periprosthetic fracture, dislocation and infection remained comparable over the three phases with slight improvements towards the end of phase 3.
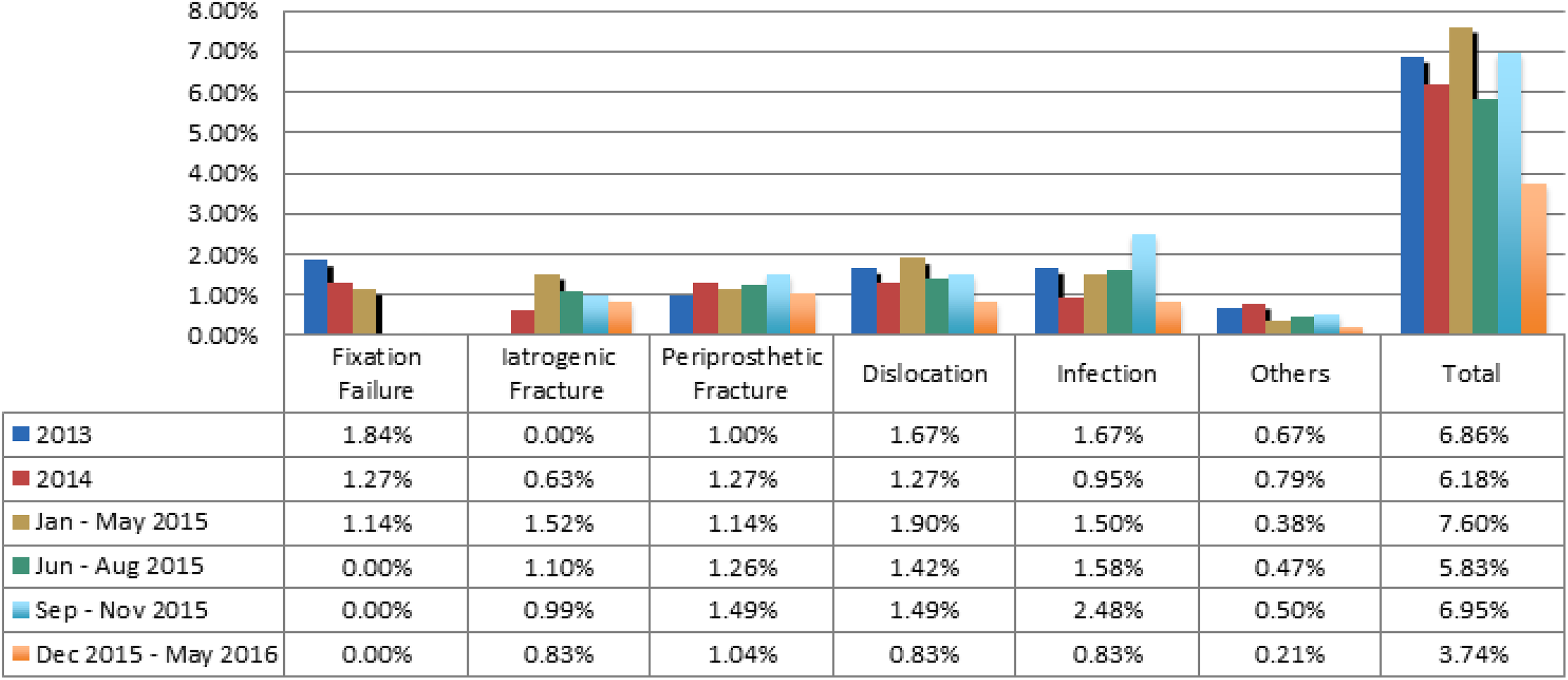
The total surgical complication rates have improved from 6.2% to 7.6% to 5.8%, respectively (p = 0.116) over the three phases. The graph and table show the breakdown comparing the complication rates over the three phases.
The 30-day mortality rate remained low and was comparable below 2.7% (p = 0.374) over the three phases (Figure 5). The unplanned readmission rate (within 28 days) also remained low less than 2.2% (p = 0.907) over the three phases of the study (Figure 6). These data are slightly lower than the overall HA average of 2.5%.
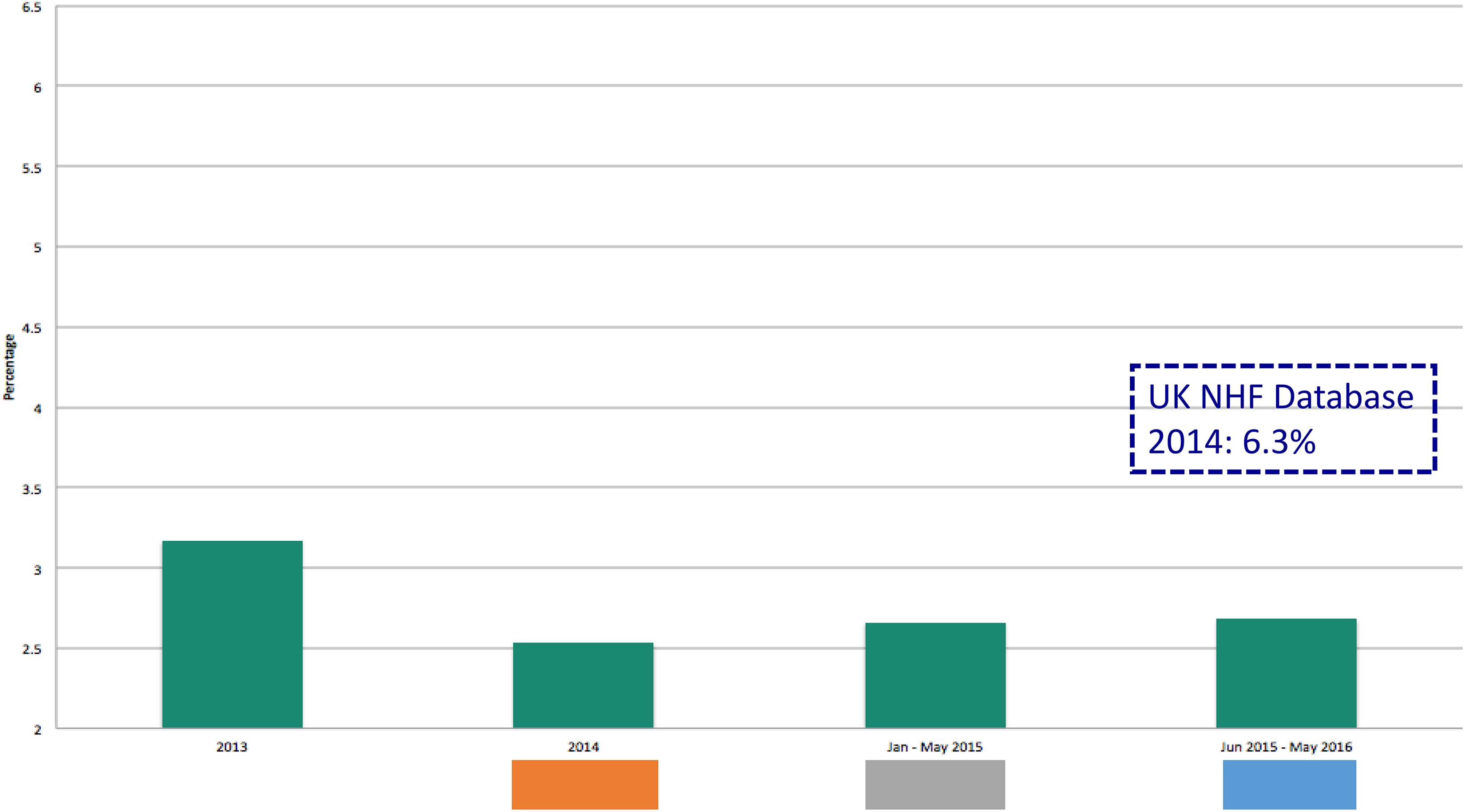
The 30-day mortality rate remained low and below 2.7% (p = 0.374) over the three phases, which is less than data taken from the UK NHFD database. NHFD: National Hip Fracture Database.
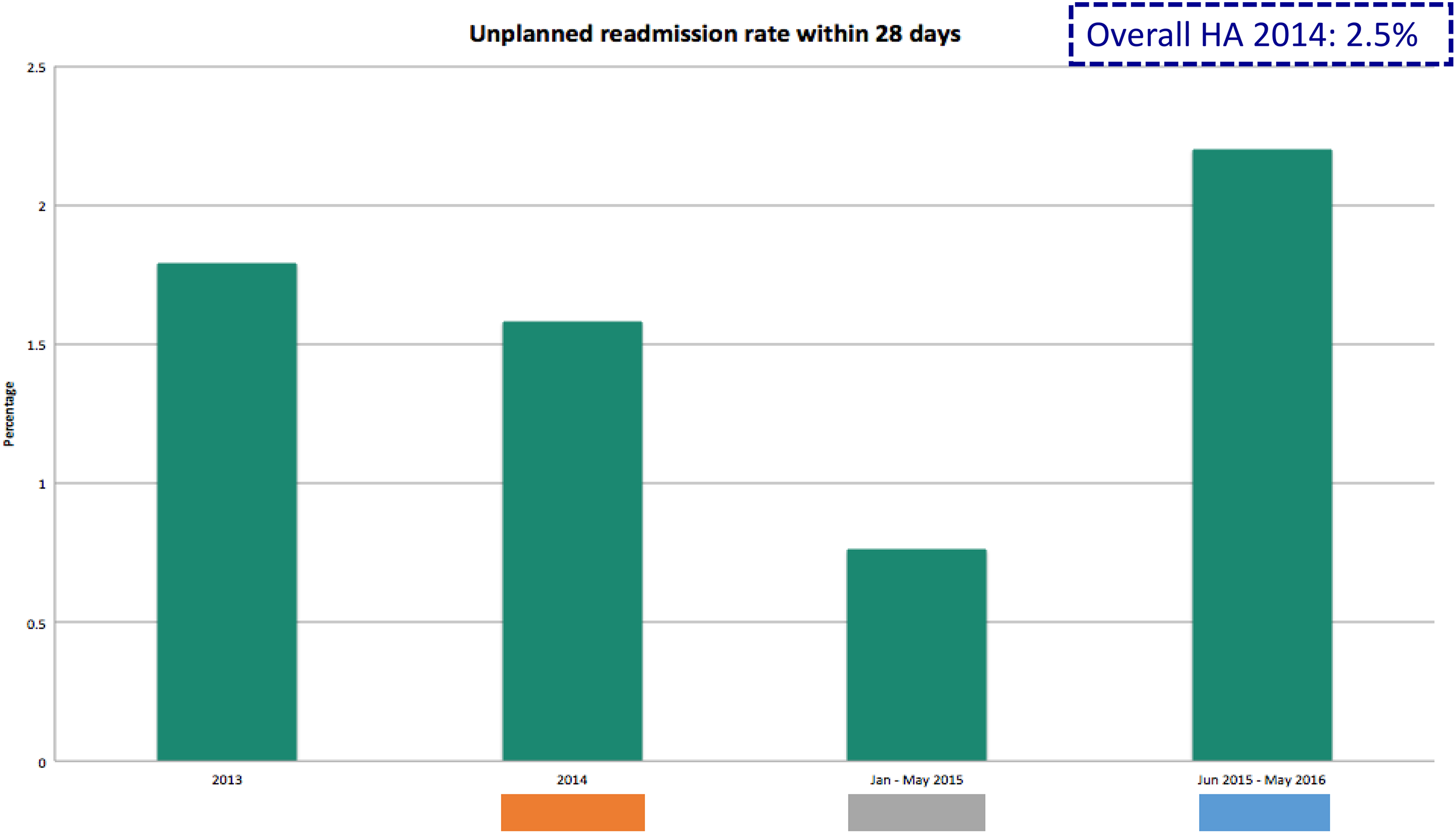
The unplanned readmission rate (within 28 days) also remained low and less than 2.2% (p = 0.907) over the three phases of the study. These data are slightly lower than the overall HA 2014 average of 2.5%. HA: Hospital Authority.
Discussion
The results show a gradual yet significant improvement in the number of FHF patients receiving their operation within 2 days of admission in our hospital after the implementation of both the FHF team and FHF pathway. Operation within 48 h is an important target to meet as outlined by the FFR working group and in the Blue Book from the BOA. There has been much debate in the literature as to when to perform hip surgery in the elderly suffering from an FHF, but the general consensus is by delaying the time to surgery, there is a higher rate of complications and increased mortality. 8,9 This is further supported by a local observational study by Liu et al. on elderly Chinese patients with hip fractures, which showed that there was a significant increase in 30 day, 1 year and long-term mortality rates for patients with a longer preoperative stay before their FHF surgery. 10
There has been a significant improvement in the acute length of stay since implementing the dedicated FHF team and FHF pathway. By shortening the time to surgery as well as decreasing the acute length of stay, we can prevent our patients suffering by stabilizing their hip fractures earlier as well as speeding up their training and rehabilitation. In doing so, there are implications that there is a reduction of costs in the management of FHF. The improvements revealed in this set of early results are encouraging. Ongoing modifications and fine tuning of the protocol are in progress to facilitate daily practical usage.
Bone health management is an important aspect in fragility fracture management. This is outlined in the article from Leung et al. 7 that only 23% of Hong Kong patients were discharged with bone protection medication compared with 70% in the United Kingdom. This may be explained by the fact that osteoporosis management is driven by bone mineral density measurements rather than suffering from a fragility fracture. 11 Upon implementation of the FHF pathway, dual-energy X-ray absorptiometry (DXA) scan became our routine investigation in the FHF patients for osteoporosis screening to identify the high-risk group. Routine referral to osteoporosis outpatient clinics headed by geriatricians was given for indicated patients for timely appropriate bone health medication to prevent secondary fractures.
Over the recent two decades, sarcopenia has been an increasing discussed topic in the literature being a risk factor for fragility fractures. Sarcopenia is defined as the loss of skeletal muscle mass and strength that occurs with ageing and is thought to increase the risk of falls in the elderly and therefore fragility fractures. 12 To further enhance the FHF pathway, sarcopenia assessment including hand grip strength and the relative appendicular skeletal muscle mass in DXA scan has been incorporated in since July 2016. Assigned auditors for collection of primary data and secondary parameters including functional and mental scores in the rehabilitation phase will allow us to have interval outcome evaluation.
More recently in late December 2016, a designated ‘elder friendly ward’ was opened for FHF patients. This new ward centralizes the same group of patients in the centre so as to provide a more focused multidisciplinary care, simplify perioperative logistics and speed up the rehabilitation process, aiming at allowing patients to reintegrate into the community earlier. 13 In the near future in early 2017, a new version of the protocol will be released with a friendlier layout, tailored made to our frontline doctors’ feedback to enhance daily utilization. We also plan to extend our pathway into the post-discharge period by establishing a designated FHF clinic and having a standardized follow-up plan for our patients with FHF. Last but not the least, an FHF liaison nurse will be appointed in 2017 to facilitate multidisciplinary coordination for all the FHF cases. With these improvements not only will the quality of care continue to improve but also the healthcare for FHF patients would become more cost-effective.
Although the pilot pathway has yielded promising early results, certain aspects of care are still lacking and there is certainly room for improvement which is also outlined by the FFR working group. 7 Lacking ortho-geriatric collaboration is one, in which geriatricians can give timely assessment and management for FHF patients perioperatively. This can shorten the timing to surgery, reduce the number of postoperative complications and mortality and reduce the acute length of hospital stay. 14,15 We are also unable to provide 7 day a week physiotherapy for our FHF patients who will be mainly bed bound over the weekend possibly increasing acute length of stay. More improvements in primary prevention of FHF by increasing public awareness and education on fall prevention and extending osteoporosis screening to the elderly public population could be implemented. These are aims of our future care model.
Conclusions
In conclusion, the pilot implementation of the multidisciplinary FHF pathway in our centre has shown that there is a significant improvement in the number of patients receiving their operation within 2 days and the acute length of stay. We hope this pathway can be integrated into other centres in Hong Kong, with modifications based on corresponding needs to maximize its benefits. In the long term, we not only hope to provide a high quality of care towards our patients to increase public awareness and prevent secondary fracture but also hope that our pathway can be used to collect data to analyse our long-term results and to improve on our current practice.
Footnotes
Authors’ note
Previously the material has been presented at the Annual Congress of the Hong Kong Orthopaedic Association in Hong Kong Convention and Exhibition Centre on November 6, 2016.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.