
Abstract
Introduction
The occurrence of fragility fractures, hip fractures in particular, is associated with significant morbidity and mortality. Despite a reduction of annual risk of hip fracture in Hong Kong, its incidence is rising steadily with ageing population. 1 This has become a huge public health burden. Using the projected percentage of elderly aged more than 65 years in Hong Kong, and assuming that the annual risk of hip fracture remains the same, it was estimated that the annual incidence of geriatric hip fracture will be more than 14,500 by 2040, more than a three-fold increase from 2011. 1
Prescription of antiosteoporotic medications is widely recognised by medical professionals as an effective measure to prevent secondary fractures. Bisphosphonates were shown to be useful for secondary prevention of osteoporotic fractures in a meta-analysis, and alendronate was most likely to be successful at secondary prevention of vertebral and hip fractures compared with other bisphosphonates. 2 That being said, workup and treatment of osteoporosis following a fragility fracture remain under-utilised in clinical practice worldwide. Patients, on the other hand, are not well aware of the potential risks of refracture and benefits of secondary prevention. It was observed in Hong Kong that only 23% of patients with fragility hip fractures received antiosteoporotic medications on discharge, and that only 35.1% of patients attended out-patient follow-up one year later. 3 The concept of imminent fracture risk, referring to markedly elevated fracture risk within next 12–24 months, has been emphasised in recent years, making timely initiation of osteoporotic treatment a crucial action. 4
Capture the Fracture is a global campaign organised by the International Osteoporotic Foundation established in 2012 to facilitate the implementation of fracture liaison service worldwide. This model of care works in a coordinator-based and multidisciplinary manner in order to identify patients with fragility fractures, refer them for bone assessment, initiate anti-osteoporotic treatment, and improve their long-term compliance. It serves the purpose of preventing future fractures and closing the current care gap. 5 In Hong Kong, Fracture Liaison Service (FLS) was first introduced in three acute public hospitals in 2017. The service coverage has been expanding in terms of participating hospitals, while the target population is limited to geriatric hip fracture patients. Numerous studies about FLS have been done worldwide to review its outcomes.6–8 We would like to assess its effectiveness using our hospital data and evaluate whether the findings are consistent with former studies.
Methods
Programme description
Princess Margaret Hospital is a public hospital located in the Kowloon West Cluster of Hong Kong offering specialised orthopaedic care. It is one of the five major trauma referral centres in the city. FLS has been officially implemented in our centre since July 2020, which involved a coordinator-based system and established a standard of care for geriatric patients admitted to our Orthopaedic ward for hip fracture requiring operation. Multi-disciplinary care from orthogeriatricians, anaesthetists, dietitians, physical therapists, occupational therapists and medical social workers are involved to optimise peri-operative management, nutritional status, rehabilitation, fall precaution, home safety and discharge planning. A senior orthopaedic specialist works as the programme leader and plays an important role in patient flow and communication within the FLS team. A designated fracture liaison nurse (FLN) works as the coordinator and plays a crucial role in facilitating delivery of consistent comprehensive care and engaging patient as a partner throughout their recovery journey. During the hospital stay, FLN takes part in case identification, invitation for subsequent investigation and management, as well as education with respect to bone health maintenance and fall prevention. Written educational materials are given to patients and their respective families. Osteoporosis treatment is commenced within same hospital admission if patient is eligible for participation in FLS programme. Exclusion criteria are supplemented in the study design section. Alendronate is considered as the first line treatment as long as there is no significant renal impairment or active dental issue. Patients are referred for bone density assessment upon discharge.
Fragility fracture clinic (FFC) sessions run by orthopaedic surgeons and nurses are arranged after discharge. Individuals who are actively under specialised care of the Department of Medicine & Geriatrics (M&G) are excluded and referred to their respective clinics for further management of osteoporosis instead. Blood tests, including renal function test, calcium and phosphate levels, and radiographs of bilateral femurs are monitored regularly. Doctors are responsible for reviewing investigation results and drug regimen for osteoporosis in FFC. Alternative medication instead of alendronate may be considered in patients with more severe osteoporosis (T score < −3), multiple recurrent fragility fractures, gastrointestinal upset or significant renal impairment. FLN reinforces patient education and drug compliance via both FFC and regular phone consultations.
Study design
A retrospective single-centre cohort study was conducted to collect historical data from the Department of Orthopaedics and Traumatology, Princess Margaret Hospital before and after intervention. Patients aged over 65 years admitted to our unit from October 2020 to September 2021 for a fragility hip fracture were recruited in the intervention group. Those admitted from April 2019 to March 2020 were regarded as the control. All of them received fracture fixation or arthroplasty. Cases from April 2020 to September 2020 before the official launch of FLS were not recruited because the programme was in a pilot stage and not yet fully implemented. Data was retrieved by searching for the diagnostic code of fracture hip via the Clinical Data Analysis and Reporting System of Hospital Authority. Medical record was evaluated individually to assure validity. Study was approved by the Kowloon West Cluster Research Ethics Committee (reference number: KW/EX-23-025(182-07)). Informed consent from participants was waived as it was a retrospective analysis which did not cause harm or privacy concern to individuals. Relevant data was solely used for research purpose and discarded after usage. Fracture cases owing to high energy trauma, malignancy, infection or bisphosphonate use were excluded. Those who were bed or chairbound, severely demented with Abbreviated Mental Test score <5 or Montreal Cognitive Assessment test score <8, lived out of the area, or passed away during hospital stay were considered ineligible to participate in the programme.9,10 Patients who had regular follow up in outpatient clinic of M&G would be referred back for further management of osteoporosis instead of being recruited in the FLS programme. Cases in the control group were selected based on the same criteria as in the cases in the FLS group. Our primary outcomes were to evaluate the incidence of fracture recurrence and mortality within the follow up period, i.e. 15 months following index admission. The term fracture indicated a fracture event, in which one or more fractures may occur on the same occasion. Vertebral fractures, which can be difficult to assess, were excluded. The secondary outcomes consisted of bone health assessment, initiation of anti-osteoporotic treatment, types of medication, and discontinuation of treatment. Treatment initiation rate was calculated based on patients who were started on anti-osteoporotic medications (bisphosphonate, denosumab or bone-forming agents) within the follow-up period. Treatment discontinuation signified that one was no longer on any anti-osteoporotic medications at the end of follow-up time. Baseline characteristics of the study population were collected, including age, gender, premorbid function, type of operation, history of fragility fracture and preoperative health status.
Statistical analysis
Both baseline characteristics and outcomes were compared between intervention and control groups for any statistical differences. Chi-squared test or Fisher's exact test was performed for categorical variables, whereas differences between continuous variables were investigated using independent t test. Univariate logistic regression analysis was conducted to evaluate the association of patient characteristics and composite outcome (re-fracture and mortality). A p-value of <.05 is justified for statistical significance.
Results
Patient characteristics
A total of 139 patients were included in the study, with 68 in the intervention group and 71 in the control group. The selection process of the intervention group was illustrated in Figure 1. Baseline characteristics of two groups were compared and listed on Table 1. The mean age of study population was 80.8, in which 78.4% were female. There was no statistical significance between two groups with regard to age, gender, premorbid function in terms of walking status and modified Barthel index (MBI) on admission, pre-operative health in terms of American Society of Anaesthesiologist (ASA) score and various medical comorbidities, as well as type of operation performed.11,12
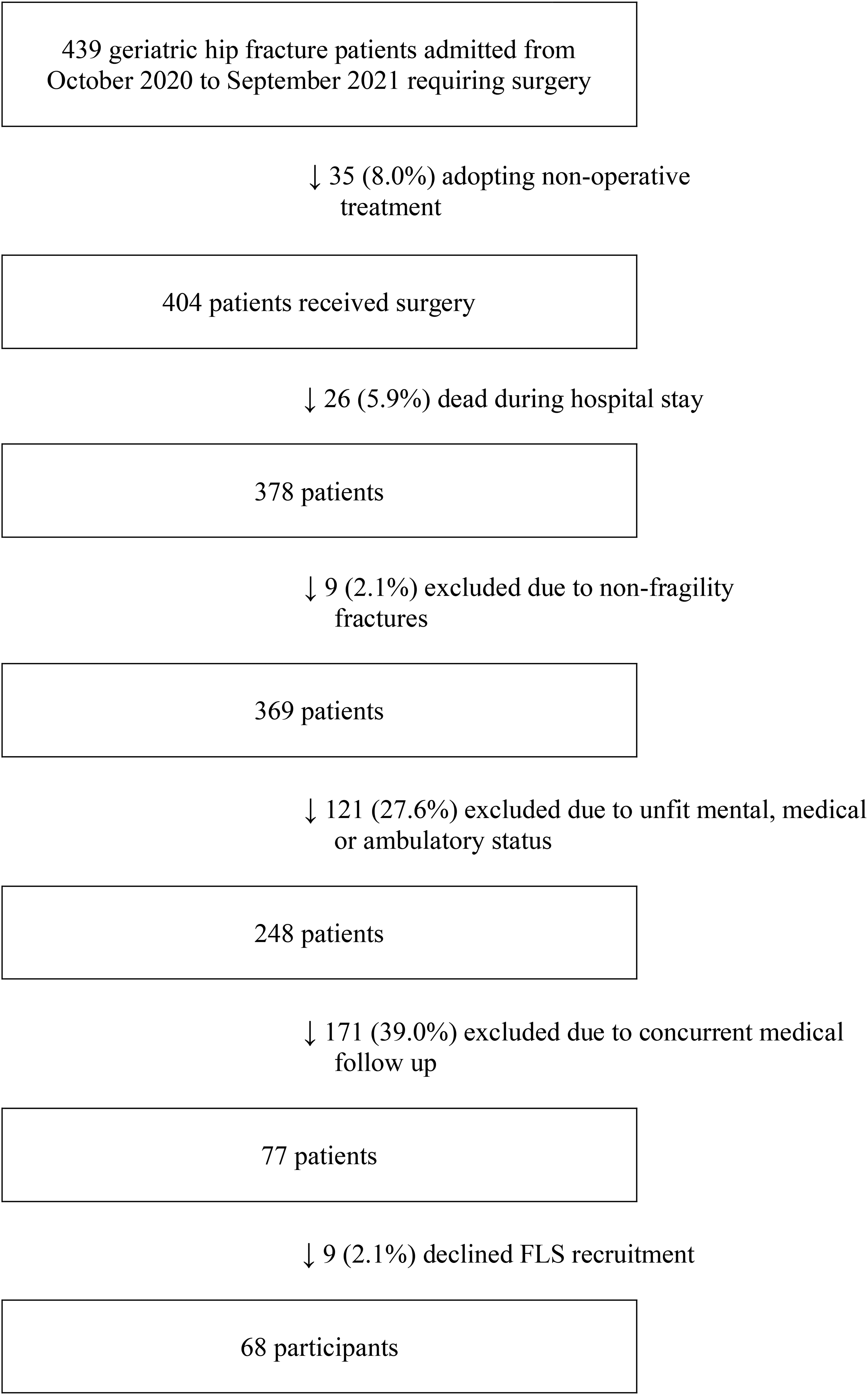
Patient selection flow chart.
Demographic profile of study population.
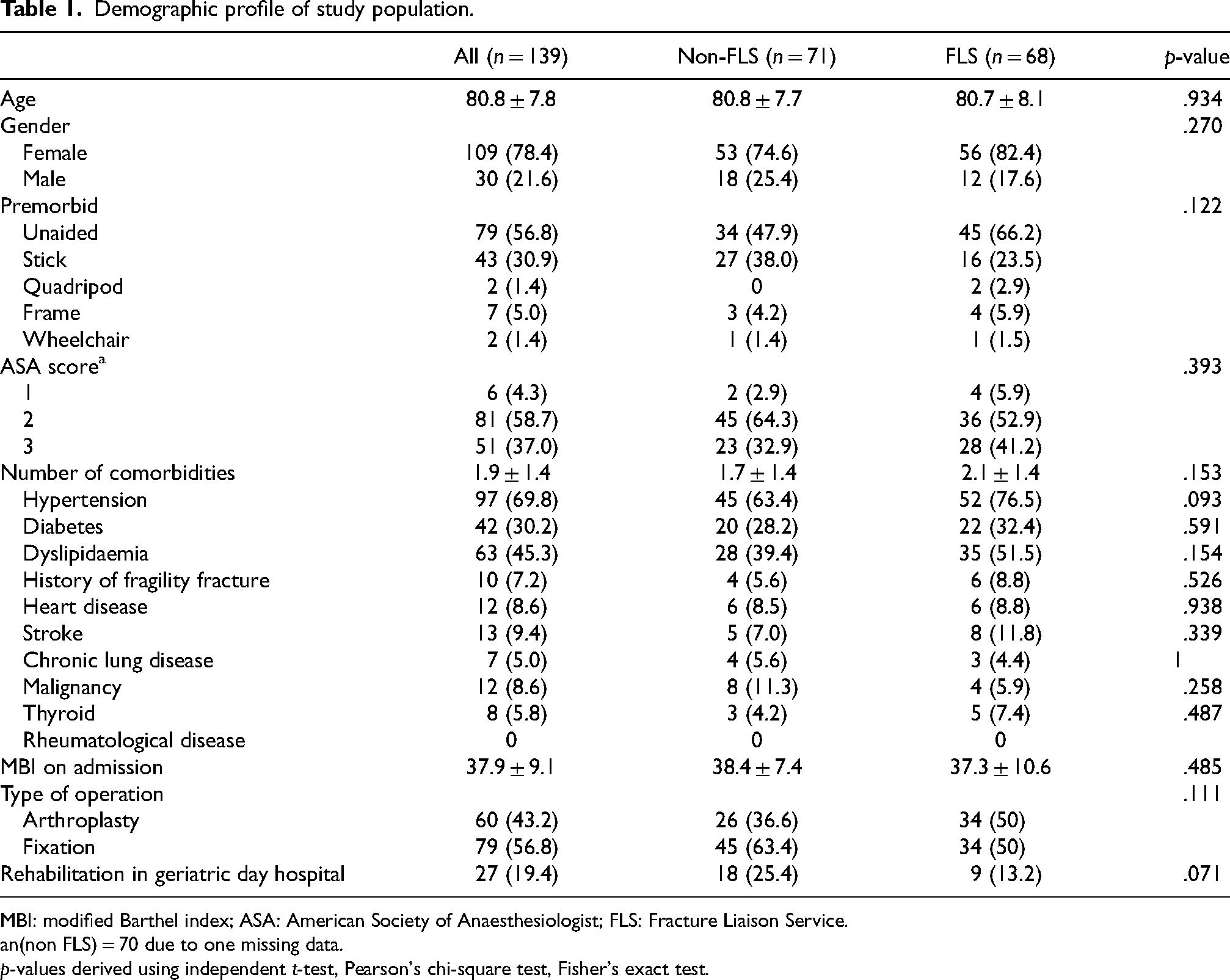
MBI: modified Barthel index; ASA: American Society of Anaesthesiologist; FLS: Fracture Liaison Service.
n(non FLS) = 70 due to one missing data.
p-values derived using independent t-test, Pearson's chi-square test, Fisher's exact test.
When it comes to association between baseline characteristics and composite outcome (Table 2), univariate logistic regression analysis showed a statistically significant positive relationship regarding number of comorbidities, with an odd ratio of 3.71 and a p-value of .004. There is a positive relationship between ASA score and outcome (OR 3.55) but it is statistically insignificant. In terms of activities of daily living, patients with a lower MBI score tend to achieve a slightly better outcome (OR 0.93) with a p-value of .085. Age and gender appeared to be less relevant in this setting.
Association with composite outcome (15-month refracture or death): Univariable logistic regression.
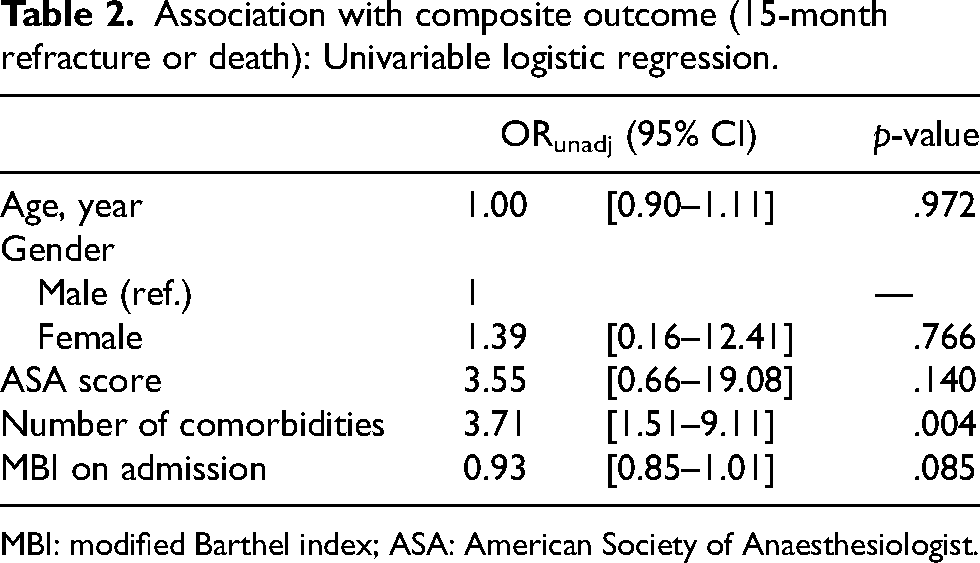
MBI: modified Barthel index; ASA: American Society of Anaesthesiologist.
Refractures and deaths
No refracture was reported in the FLS group within the follow up period, while four were noted in the pre-intervention group (5.6%). Two of the refracture patients sustained a contralateral side hip fracture at post-injury three months. Oral bisphosphonate was prescribed by us for one of them after refracture. Another sustained foot and ankle fractures after 5 months. The remaining one suffered from distal ulnar and proximal humerus fractures after 13 months, despite being put on denosumab by an oncologist 8 months after initial fracture in conjunction with hormonal treatment of breast cancer. No statistical significance was demonstrated between the two groups with a p-value of .120.
On the contrary, the two deaths recorded within the follow up period belonged to the FLS group (2.9%). Both were found arrest before arrival to hospital and the exact causes of death were uncertain. They succumbed at post-index fracture 10 months and 12 months respectively. The difference in mortality rate remained statistically insignificant with a p-value of .238.
Follow-up bone density testing
The majority of intervention group were arranged for a DXA scan after index fracture. Forty-one patients (60.3%) completed the scan within the follow up period. On the other hand, only 6 (8.5%) in the control group did so. The p-value was <.001.
Anti-osteoporotic treatment
Table 3 also illustrated the use of anti-osteoporotic medications in our patients. Overall 80 patients (57.6%) received anti-osteoporotic treatment within the study period. Prescription rate was markedly elevated in the intervention group (p-value <.001). Sixty-six out of 68 (97.1%) were put on treatment, as opposed to 14 out of 71 (19.7%) in the control group. In the FLS group, 59 patients received our first line treatment alendronate, while 12 received denosumab injection. Medication change from alendronate to denosumab was recorded in five cases because of low T-score on DXA (n = 3 with T score < −3), gastrointestinal upset (n = 1) or renal impairment (n = 1). In the non-FLS group, nine were on alendronate, four were on denosumab, and one was on teriparatide. None of their medications were modified.
Results before and after FLS project in a follow-up time period of 15 months.
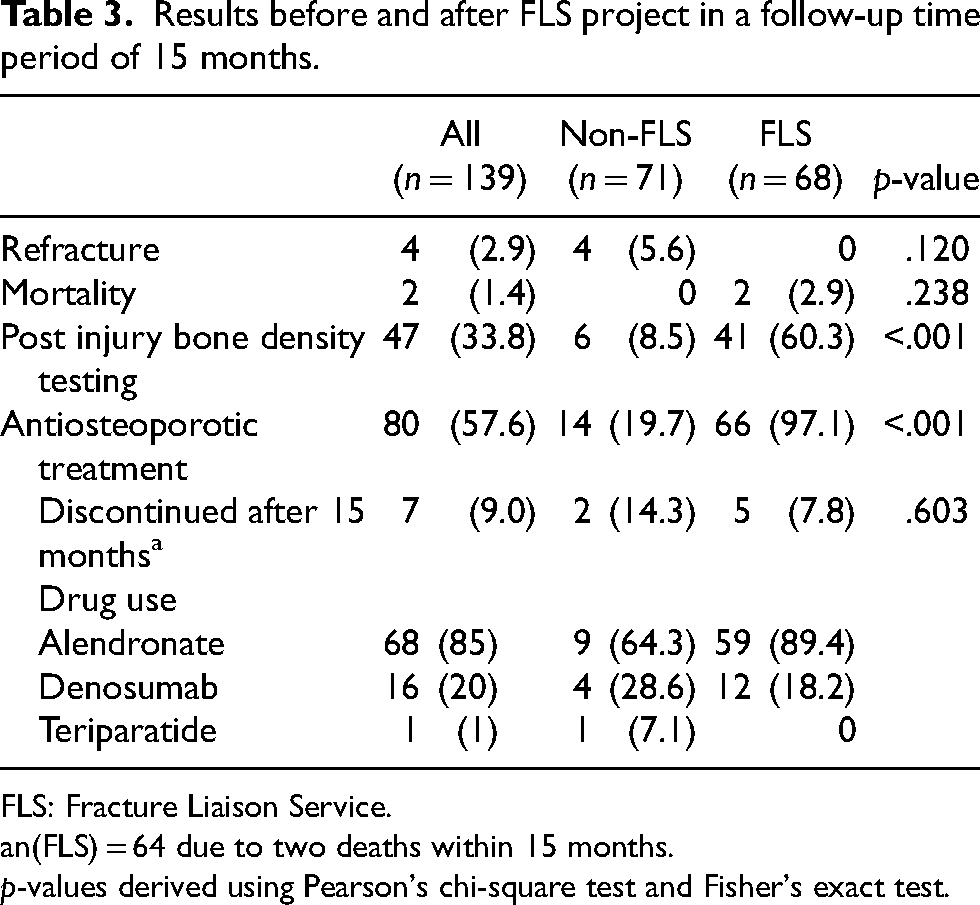
FLS: Fracture Liaison Service.
n(FLS) = 64 due to two deaths within 15 months.
p-values derived using Pearson's chi-square test and Fisher's exact test.
Treatment was discontinued in five patients with FLS (7.8%) at the end of study period for the following reasons. Three of them defaulted follow up without drug refill. One was no longer fit to continue in the light of deteriorating medical condition, and the other could not tolerate alendronate because of gastric reflux. As for the control group, treatment was terminated in two (14.3%) cases. One of them declined to continue treatment. The other became chairbound during follow up period, and was considered physically not fit for continuing treatment. No statistical significance was shown between two groups (p = .603).
Discussion
Before the era of FLS, even though anti-osteoporotic medications were known to doctors as treatment and secondary prevention of fragility fractures, management in multiple aspects including drug initiation, investigation, patient education, treatment monitoring and follow up, remained largely insufficient in clinical practice. Lack of clinical responsibility and coordination were likely key contributing factors. Majority of patients with fragility fractures were presented to and subsequently followed up in orthopaedic specialty, yet issue of underlying osteoporosis was commonly not addressed. The problem may be simply ignored or patients may be referred to other clinics such as medicine and primary care for further management. Patients could hardly realise the importance of early secondary prevention without proper education and timely management due to the long waiting time in public sector. Without clear clinical responsibility and management guidelines, orthopaedic doctors may not play a proactive role in writing anti-osteoporotic drug prescriptions and monitoring treatment effects in the long run. In addition, discussion of anti-osteoporotic drug treatment only after availability of investigation results was a common practice among medical professionals. Time delay in investigation in public sector and subsequent treatment initiation was another major problem. These are some of the key reasons why FLS is established worldwide in attempt to close the care gap and offer standardised care to this group of patients.
Our programme demonstrated several fundamental operational features of a hospital-based FLS, which involved a coordinator-based system and established a standard of care for fragility hip fracture patients to prevent secondary fracture. The programme was set up with reference to the Best Practice Framework developed by Capture the Fracture. 5 It is believed that a coordinator-based system could break down barriers that constitute the widely reported low rate of outpatient intervention in fragility fracture patients. 13
Ganda et al. grouped FLS models into four types—type A: identification, assessment and treatment of patients as part of the service; type B: similar to A, without treatment initiation; type C: alerting patients plus primary care physicians; and type D: patient education only. 14 Types A and B adopting more comprehensive care tend to accomplish better outcomes. 15 Our model of care belonged to type A, which may contribute to the favourable outcomes in the intervention group.
According to a previous study in Hong Kong, only 23% of patients were discharged with bone protection medication following fragility hip fractures, excluding calcium and vitamin D, and only 35.1% of patients attended out-patient follow-up one year later. 3 Another local study showed that 33% were prescribed medications for osteoporosis in the 6 months after discharge, and that osteoporosis diagnosis and treatment were driven by BMD measurement, not fracture history. 16 Our study justified the implementation of FLS as an effective tool with a surge of bone assessment and anti-osteoporotic drug prescription rate. Of note, even though every patient recruited in FLS was referred for bone density assessment upon discharge, there was considerable discrepancy between referral and investigation rate. One major barrier was the long queueing time in public hospital. In such scenario, referral to the private sector for the scan should be considered as long as patients can afford. This group of patients who are susceptible to early refracture should be prioritised for investigation so as to optimise anti-osteoporotic treatment regimen, and potentially improve adherence to treatment.
When it comes to reducing subsequent fractures and mortality, previous studies showed positive results in general. A systematic review and meta-analysis conducted by Li et al. revealed that the FLS care was associated with a significantly lower probability of subsequent fractures (OR 0.70, 95% CI [0.52–0.93], p-value = .01), but the association became insignificant for studies with a follow-up time fewer than two years. No significant difference in the odds of mortality was observed, yet a significantly lower probability of mortality was identified in the six pre–post FLS comparisons (OR 0.65, 95% CI [0.44–0.95], p-value = .03). 8 With reference to a cohort study in Thailand, which compared refracture and mortality rate between FLS and non-FLS group after 1-year follow up, they noted a significant decrease in refracture rate from 30.0% to 2.93%, while the mortality rate reduction from 9.2% to 5.95% was insignificant. 7 It was reported in FLS service review from another hospital in Hong Kong, Queen Elizabeth Hospital, that the rate of secondary fracture was 4.67% in the first year of implementation in 2017 and 2.82% in the third year, with a 40% reduction in percentage. 6 Our study showed a reduction in refracture rate from 5.6% to 0% but it was not statistically significant. Further studies of FLS with an extended follow-up period and larger sampling size may help convey statistically significant benefits. Additional statistical analysis could be employed, such as by Cox proportional hazard regression model for time dependent analysis when the number of primary outcomes increase. Other contributing factors for the insignificant findings could be the relatively healthy status of our study population, exclusion of vertebral fractures and concomitant care by geriatric day hospital (GDH).
Owing to resource constraints, a significant portion of fragility hip fracture patients were screened out of our FLS programme. It consisted of individuals with active regular M&G outpatient follow up in public sector, poor cognitive, ambulatory or health status, as well as those who adopted non-operative treatment. Anti-osteoprotoic drug treatment and FFC follow up were reserved for patients with reasonable quality of life. Presumably the study population represented a healthier bunch of patients with fewer medical comorbidities. In other words, generalisability of our findings may be affected. As per our results in univariate regression analysis, number of medical comorbidities was significantly associated with refracture and mortality. This could account for the comparatively small amount of primary outcomes in our setting. As a side note, further studies regarding effectiveness of FLS focusing on healthier group of geriatric hip fracture patients, which are commonly seen nowadays, may have useful implications for public health resource allocation.
Osteoporotic vertebral collapse is the most common fragility fracture with an estimated incidence of 30–50% of people over 50 years old. 17 Yet they are often clinically silent and difficult to be recognised. It was observed that only approximately one-fourth of incident radiographic vertebral deformities were clinically diagnosed as new vertebral fractures. 18 Less than 20% of radiologically identified fractures were recorded in medical record or discharge diagnosis. 19 The finding of a vertebral fracture may not be stated in a radiology report either. Even if they are picked up on imaging, their chronology is often indistinguishable especially in absence of baseline film comparison. In view of these diagnostic challenges, it was omitted in our study despite its frequent occurrence. In an ideal setting, spine radiographs taken right before and after study period and imaging interpretation by experienced doctors could accurately capture these refractures.
GDH is a day rehabilitation service run by geriatricians, physiotherapists and nurses, which allows elderly patients to receive rehabilitation and comprehensive geriatric assessment without hospitalisation. 20 The programme has been implemented for decades in several Hong Kong hospitals. Hui et al. reported that the cost of day hospital treatment in Hong Kong was much cheaper than an equivalent period of inpatient rehabilitation. 21 The service is available for hip fracture patients in our hospital as well, and it runs independent of our FLS programme. In our study, almost 20% of them were recruited. Among those in the control group receiving anti-osteoporotic medications, majority of treatment were indeed initiated by geriatricians during GDH consultation instead of orthopaedic surgeons. By providing additional rehabilitation, education and management of osteoporosis for both groups, GDH likely mitigated the positive effect of FLS implementation in this study. In presence of FLS nowadays, further discussion focusing on how these two services should collaborate to optimise patients’ outcomes with limited resources is warranted.
Some other limitations of this study were related to data collection. Since only medical record in public system was reviewed, patients with refracture episodes who were treated in the private sector could hardly be captured, although they likely just constitute a small proportion. Death occurring outside of Hong Kong could not be traced either.
Our review period overlapped with COVID pandemic which can have mixed impact on the results. There may be negative impact on long-term outcome after hip fracture owing to reduced medical support, increased complications from delayed surgery and prolonged hospital stay, and lack of rehabilitation or social support from social distancing. COVID infection can be directly detrimental to patients’ health as well. When elderly refrained from outdoor activities and probably exercise within this period, their general health including bone health can be affected. The positive side is less injury may occur if they cut down outdoor activities. Regarding FLS participation, COVID pandemic could potentially be a reason for declining recruitment. Small bunch of patients may opt not to attend the clinic in person and send relatives to refill medications instead. Fortunately, from our observation, majority still achieved good attendance to follow up and compliance to medications.
There are several strengths of our study. Since our study population was from the same hospital, they shared similar demographic information. Selection bias could be minimised. Besides we used same inclusion and exclusion criteria to recruit patients in both groups to reduce confoundings. Data was retrieved via electronic medical record to assure validity.
Conclusions
FLS implementation in Hong Kong was an effective tool to increase investigation and treatment rate of osteoporosis in geriatric hip fracture patients. Its impact on refracture and mortality rate remained insignificant in this cohort of patients. Further study with a longer follow up time and more delicate selection of participants may demonstrate a better outcome.
Footnotes
Author's contribution
Siu Sheung Kan: concept, design, definition of intellectual content, literature search, clinical studies, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing and manuscript review; Wan Yue Ting Ophelia: concept, design, definition of intellectual content, literature search, clinical studies, manuscript editing and manuscript review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics committee approval
Kowloon West Cluster Research Ethics Committee (reference number: KW/EX-23-025(182-07)).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Waived as it was a retrospective analysis which did not cause harm or privacy concern to individuals. Relevant data was solely used for research purpose and discarded after usage.