
Abstract
Introduction
Fracture Liaison Services (FLS) has been proven effective in reducing subsequent fractures and related mortality. However, more research is needed on the impact of FLS on the 30-day readmission rate and its effectiveness in rural hospitals. This study aims to assess the impact of FLS on clinical outcomes including readmission rates, subsequent fractures, and fracture-related mortality in rural areas of an Asain country.
Materials and methods
In a rural hospital in Taiwan, we conducted a two-year prospective cohort study on elderly individuals with fragility hip fractures. The study compared the clinical outcomes between the control group and the FLS-cohort group. Logistic regression analysis was used to identify factors contributing to 1-year mortality after injury.
Results
556 patients were enrolled. (304 in the control group and 252 in the FLS group) The mean age was 79.8 years. The findings revealed that the introduction of FLS did not result in significant differences in mortality, readmission, complication, subsequent fractures, or secondary hip fractures. However, there were notable improvements in the length of hospital stay and the proportion of patients receiving surgery within 48 h following the implementation of FLS. Subgroup analysis showed that FLS patients who received anti-osteoporotic treatment had lower mortality and 30-day readmission rates. Factors associated with higher 1-year mortality included male, high ASA level, and delayed surgery.
Discussion
This study provides the real-life evidence of the effect of intensive FLS model in a rural hospital in an Asian country.
Conclusion
While FLS did not show significant differences in certain clinical outcomes, it led to shorter hospital stays and increased timely surgeries. FLS patients receiving anti-osteoporotic treatment had better mortality and readmission rates. Further research is necessary to gain a comprehensive understanding of the impact of FLS care in rural areas of Asia.
Keywords
Introduction
Osteoporosis is a chronic condition characterized by low bone density, increased bone fragility, and a greater risk of fractures. 1 Osteoporosis is typically asymptomatic, and the first clinical manifestation is often a fragility fracture resulting from minor trauma. Hip fracture is the most severe fragility fracture due to its increased risk of early death and subsequent fragility fractures. 2 The mortality rate is around 10% within 1 month and 24% within 1 year after a hip fracture. 3 Besides, 10% of hip fracture patients sustained another fracture within 1 year. 4
However, many patients do not receive any evaluation after a fracture. 5 Fracture liaison services (FLS) are designed to bridge this gap. In 2012, the International Osteoporosis Foundation (IOF) facilitated the implementation of the Fracture Liaison Service globally, a post-fracture model of care that identifies all patients with a higher risk of a secondary fracture. Numerous published analyses have validated the effectiveness of FLS and similar services, which have shown increased patient assessment and treatment initiation, resulting in projected clinical benefits and cost savings.6–10 Such services are increasingly regarded as the gold standard in secondary fracture prevention.11–14 Multiple studies have confirmed the significant impact of FLS in reducing the occurrence of subsequent fractures and related mortality.15,16 The early readmission rate, generally defined as readmission within 30 days, is commonly used to measure the quality of hospital care. Though hospital readmissions are closely related to chronic illness, they are associated with higher morbidity and mortality after hip fractures.17,18 There needs to be more information about the effect of FLS in reducing the 30-day readmission rate. Besides, few studies focused on the impact of FLS in rural hospitals with more elderly patients than in the metropolis. This study examined whether the FLS program could improve the quality of care and clinical outcomes of patients who encountered fragility hip fractures in rural areas, including 30-day readmission rates, subsequent fractures, and fracture-related mortality.
Material and Methods
Study Design
A prospective cohort study was conducted on patients who experienced fragility hip fractures for 2 consecutive years before and after implementing the FLS in our hospital, a regional hospital located in the suburbs of Tainan city, featuring dairy farming. According to the data from Xinying household registration office, Tainan city, the national population density is 646.25 people per square kilometer. Within the hospital's area, the population density is approximately 200 to 300 people per square kilometer. The elderly population accounts for over 20% of the total population, with more than 60% of the elderly having an education level of primary school graduation or below. (https://web.tainan.gov.tw/shinying/).
Study Population
Patients over 50 with fragility hip fractures, including femoral neck and trochanteric fractures, were included between January 1, 2019, and December 31, 2020. Patients with pathological and periprosthetic fractures and high-energy injuries (i.e., those due to traffic accidents or falling from heights) were excluded.
Patients were categorized into 2 groups. The patients who suffered from hip fractures between January 1, 2019, and December 31, 2019, were grouped as the control group. Those who encountered hip fractures between January 1, 2020, and December 31, 2020, were defined as the FLS cohort group. Patients were followed from the date of the initial hip fracture (index date) until the death of any cause or end of the 1-year follow-up. Written informed consent was obtained from all participants before their involvement in the study
Outcome Measures
The primary outcomes included rate of DXA scanning, anti-osteoporosis medication prescribing, length of stays, 30 days re-admission rate, mortality rate within 1 month and 1 year, and surgical related complication rates (i.e., surgical site infection, implant loss of reduction, hip prothesis dislocation). Fragility fractures are fractures that occur as a result of a fall from standing height or less, involving areas like hip, spine, wrist and shoulder. 1-year subsequent fragility fractures (except hip) and 1-year second hip fractures were considered secondary outcomes. Subgroup analysis was also undergone in the FLS cohort group to reveal if anti-osteoporotic treatment is an impact factor in reducing the mortality rate. We divided the patients into those receiving anti-osteoporotic treatment and patients untreated. The data were obtained from medical records and telephone calls to patients or their families by a specialized liaison nurse certified by the Taiwan Osteoporosis Association.
Data Collection
The following information was collected from our electrical medical record system: age, gender, American Society of Anesthesiologists (ASA) score, fracture side, and type of fracture (femoral neck, trochanteric or subtrochanteric). Moreover, surgical-related complications, referral to dual-energy X-ray absorptiometry (DXA) scanning, the rate of time to surgery (TTS) within 48 h of injury, and the length of stay (LOS) were also collected.
Statistical Analysis
Chi-square test and Fisher’s exact test were employed to compare categorical data, i.e., sex, side, fracture type, and so on. The independent t test was used to analyze continuous data, such as age and length of hospital stay. Furthermore, using multiple logistic regression analysis, we evaluated the contribution to death within 1 year after injury with the following variables: age, sex, ASA, FLS intervention, surgery within 48 h of injury, and occurrence of postoperative complications. A two-tailed P-value of <.05 was considered statistically significant. We used IBM SPSS Statistics for macOS (Version 25.0. Armonk, NY: IBM Corp) to analyze the data.
Fracture Liaison Services (FLS)
In the FLS, a specialized liaison nurse systematically evaluated patients within 8 weeks post-surgery. The evaluation included estimating the 10-year fracture risk by FRAX (fracture risk assessment tool), DXA scanning, lifestyle behaviors (amount of supplemental calcium and vitamin D3 intake, protein intake, exercise, smoking, and alcohol, etc.), fall risk assessment & prevention, and blood test to screen for possible underlying secondary endocrine causes osteoporosis. If the patient has received prior treatment for osteoporosis, evaluation of the medication dosage, side effects, compliance, and contraindications were also carefully analyzed. The specialized liaison nurse would also provide comprehensive education on the disease of osteoporosis and its treatment involving medications or other non-pharmacological management options to participants of our program when indicated.
Osteoporosis treatment decisions depend on the National Osteoporosis Foundation (NOF) guidelines,
19
especially for the groups including postmenopausal women and men aged 50 and older presenting with the following: • A hip or vertebral fracture. • T-score ≤ −2.5 at the femoral neck, total hip, or lumbar spine. • Low bone mass (T-score between −1.0 and −2.5 at the femoral neck or lumbar spine) and a 10-year probability of a hip fracture ≥3% or a 10-year probability of a major osteoporosis-related fracture ≥20% based on the US-adapted WHO algorithm.
Results
Patient Characteristics Between the Control and the FLS Cohort Groups.
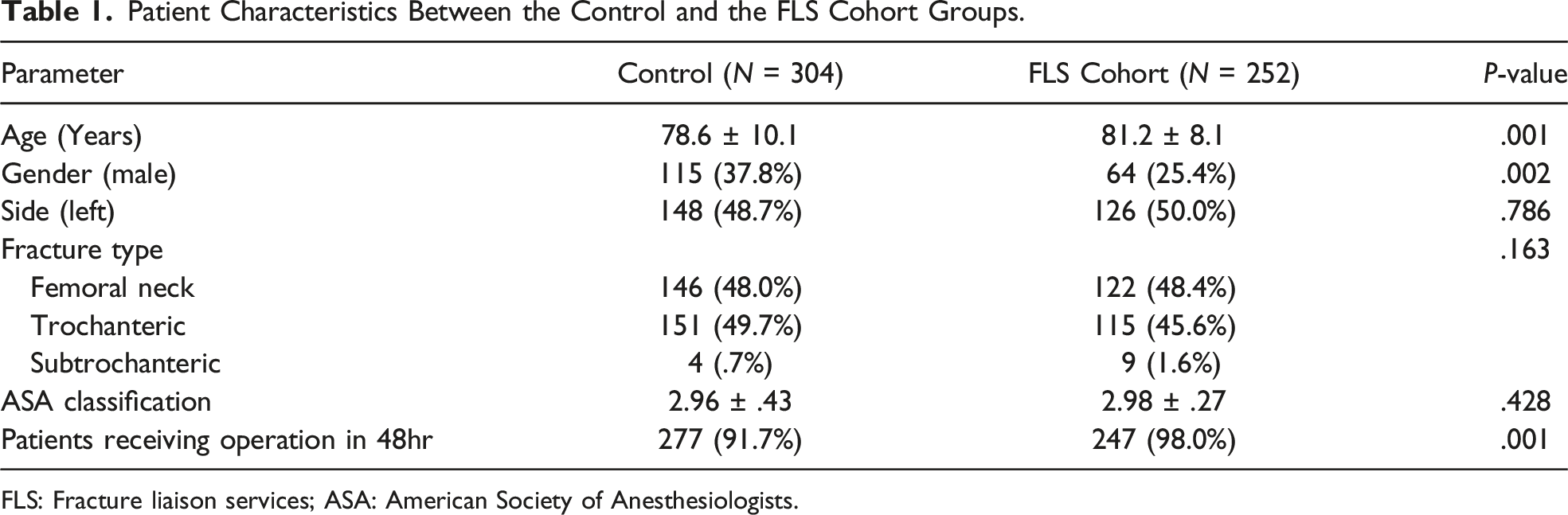
FLS: Fracture liaison services; ASA: American Society of Anesthesiologists.
Primary Outcomes
Outcomes Between the Control and the FLS Cohort Groups.

DXA: Dual-energy X-ray absorptiometry.
Secondary Outcomes
The 1-year subsequent fragility fracture rate was 4.9% (n = 15) in the control group and 4.4% (n = 11) in the FLS cohort group (P = .752). A total of 18 patients (3.2%) suffered a secondary hip fracture in 1 year, with 12 patients (3.9%) before FLS implementation and 6 patients (2.4%) after FLS implementation (P = .299) (Table 2).
Subgroup Analysis
Subgroup Analysis of the FLS Cohort Group.

DXA: Dual-energy X-ray absorptiometry.
Multiple Logistic Regression Analysis to Determine the Factors Contributed to Death in One Year.

ASA: American Society of Anesthesiologists; FLS: Fracture liaison services; OR: Odds ratio; CI: Confidence interval.
Discussion
Doshi et al showed a 2.3% 30-day mortality and 5.9% 1-year mortality rate in hip fracture patients after implementing FLS in Singapore, 20 and Leung had revealed a 1.8% 30-day mortality rate and 11.5% 1-year mortality rate in Hong-Kong following FLS intervention. 21 Our findings correspond to previous studies conducted in Asia. (1.6% 1-month mortality rate and 12.6% 1-year mortality rate) The 2 groups did not show a significant difference in the mortality rate within 1 month and 1 year after injury, although the rate was slightly lower in the FLS cohort group. This outcome could be attributed to the age difference between the 2 groups, as the FLS cohort group had an older population (81.2 ± 8.1 years vs 78.6 ± 10.1 years, P = .001). Heterogenic results have been observed in previous studies. A large Swedish study reported 1-year post-fracture mortality rates in patients of 13.3% and 12.2% before and after the implementation of FLS, respectively, although this difference was not statistically significant. 22 On the other hand, the beneficial impact on mortality associated with the use of an FLS or orthogeriatric model was also reported by previous studies. Hawley et al found improvements in 1-year post-fracture mortality rates in patients following implementation of either an FLS (HR = .84, 95% CI .75-.87) or an orthogeriatric service (HR = .81, 95% CI .77-.93) in the UK. They also observed reductions in age and sex-standardized 30-day mortality (HR = .73, 95% CI .65-.82). Additionally, their findings indicated that the number of patients needed to be treated to prevent 1 excess death within 30 days was 17 for the FLS intervention. 23
Length of stay (LOS) has been used to indicate the efficacy of the provided care. In addition, it may be associated with a lower total cost per patient. Time to surgery is also an essential parameter in the care of hip fracture patients because of its association with mortality. This is explained by the increased risk of respiratory, cardiovascular, thrombotic, and infectious complications resulting from confinement to bed and preoperative stress when surgery is delayed. 24 In this study, the real-life evidence of an FLS in reducing the hospital LOS was observed, and the proportion of surgery performed within 48 h after injury increased after implementing FLS, corresponding to the results reported in previous research. In a meta-analysis of 18 studies by Grigoryan et al, the hospital LOS decreased with ortho-geriatric collaboration. 25 In our FLS program, the primary core is composed of orthopedic surgeons. We have supplied pertinent evidence to other specialized physicians, including emergency physicians and anesthesiologists, to underscore the importance of timely surgery. Furthermore, as the concept of Enhanced Recovery After Surgery (ERAS) becomes increasingly widespread, it promotes collaboration among multidisciplinary teams. These factors might help elucidate the findings mentioned.
To the best of our knowledge, this is the first study to report an association between the implementation of an intensive FLS model and the 30 days readmission rate of patients with hip fractures in a single hospital in Asia. In our data, the effect of FLS on the 30-day readmission rate was insignificant. A systematic review reported a median 30-day readmission rate after hip fracture was 10.1%, and patient-related risk factors such as age, co-morbidities, and functional status are stronger predictors of 30-day readmission than hospital-related factors, including the initial LOS, hospital size, and volume, time to surgery and type of anesthesia; besides, readmission is a strong predictor of mortality at 1 year. Previous studies reported heterogeneous results concerning the LOS, with prolonged LOS associated with both an increase and a decrease in the readmission rate. 26 More research is needed to determine the effect of the FLS models on the 30-day readmission rate.
Surgical management of hip fractures in older people is challenging, and complications relating to surgery could be devastating. The incidence of surgical complications has been estimated in the region of 6.9%, with mechanical failure and infection being the most common. 27 Although the surgical complication rate declined, the difference between the 2 group did not achieve significant difference in our study.
On the other hand, we did neither find a reduction in the second hip fracture or subsequent fragility fracture in patients treated using the FLS protocol. This finding has not corresponded with other studies that showed a significant reduction in second osteoporotic fracture rates. A large-scale study found an 18% reduced risk of recurrent fracture compared with patients in the period before the FLS implementation. 28 However, another study showed that the FLS program did not reduce the risk of suffering a second fragility fracture in patients with hip fractures. 29 Moreover, 1 review article reported studies performed on FLS programs had heterogeneous designs and study populations. 30 Therefore, further studies are needed to determine the effect of FLS protocols on subsequent fracture risk.
Another finding of this study was the increase in the prescription of anti-osteoporotic drugs and DXA exams with the implementation of the FLS program. Numerous studies have proved that FLS increases the initiation of osteoporosis treatment. The comparative analysis of the Fracture Prevention Clinic in Newcastle, Australia, demonstrated increased treatment rates in the FLS group after an average of 2 years of follow-up. 31 Another study examining a cohort of postmenopausal women with hip fractures showed that FLS might result in higher osteoporosis treatment rates. 32 Furthermore, there is strong evidence that FLS is associated with increased number of patients referred for bone density assessment with DXA. Compared to the period before FLS or usual care, there was almost a 2- to 18-fold increase in DXA referrals.22,33–35 As a result, our findings are comparable with previous studies.
Previous studies conducted in Australia have reported that the implementation of FLS in rural hospitals resulted in modest improvements in outcomes, with limited awareness of the implications of fragility fractures.36,37 In our hospital, although the data did not reveal a significant reduction in the 30-day and 1-year mortality rates, as well as the 30-day readmission rate, following the initiation of the FLS, there was an increase in the rate of patients receiving anti-osteoporotic treatment with the implementation of the FLS program. In subgroup analysis, this increase subsequently led to a significant reduction in the 30-day and 1-year mortality rates and the 30-day readmission rate compared with those who did receive anti-osteoporotic treatment. These findings suggest that if the FLS program prioritizes anti-osteoporotic therapy after hip fracture, there is potential for significant improvement in these outcomes. Nevertheless, the subgroup analysis data revealed that among patients without anti-osteoporotic treatment, there were more males and higher ASA classifications, which could potentially act as confounding factors.
Age is a known risk factor for mortality in Multiple logistic regression analysis, probably because of increased comorbidities, fragility, and polypharmacy. Besides, the male gender was a risk factor for higher mortality at 1-year post-hip fracture, which was compatible with previous studies. The men have higher early postoperative mortality 38 and are less likely to return to independent living or mobility. 39 In addition, efforts must be pursued to decrease the time of surgery, as it is 1 of the mainstays of orthogeriatric programs. Previous studies have indicated that delayed surgery is associated with an increased risk of mortality and other complications.40,41 In our hospital, 98% of patients in the FLS cohort group can receive surgery within 48 hours. It may be because orthopedic surgeons dominate the FLS program, and we believe that prompt surgical intervention and early rehabilitation could positively impact long-term morbidity and mortality.
This study had several limitations. First, the sample size was relatively small, and the follow-up period was relatively short. Second, this study was a prospective cohort study, which may have affected the interpretation of the results. However, we acquired data from a robust, accurately constructed database by trained staff. In addition, the before-and-after design does not provide a cause-and-effect relationship between mortality and the FLS model. Further randomized controlled trials examining a large sample are still necessary to understand the influence of the FLS program and the mortality of hip fracture patients.
Conclusion
Implementing an FLS protocol in our rural hospital in Taiwan led to increased BMD tests and prescriptions of anti-osteoporotic drugs for elderly hip fracture patients. The introduction of FLS resulted in more immediate surgeries and shorter hospital stays, potentially improving patient independence. There were no significant differences in mortality, complication rates, or risk of second fragility fractures or hip fractures between patients treated before and after FLS implementation. However, FLS patients receiving anti-osteoporotic treatment had reduced mortality and 30-day readmission rates. Factors contributing to higher 1-year mortality included male gender, high ASA level, and delayed surgery. Further research is needed to establish the full impact of FLS care.
Footnotes
Acknowledgements
We would like to express our gratitude to the Chi-Mei Medical Center for funding this research through grant. (CLFHR10926).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Chi-Mei Medical Center, Liouying (CLFHR10926). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical Statement
This study was conducted in accordance with the ethical principles outlined in the Chi-Mei Medical Center Research Ethics Committee guidelines. The Chi-Mei medical center’s ethical committee approved the protocol and instrumentation (IRB study number: 10908-L01). All participants consented to the study and the publication of data.