
Abstract
Introduction
The primary function of the wrist is to provide a mobile yet stable platform for the hand. 1 Traditional treatment for end-stage wrist destruction pathologies such as rheumatoid arthritis, psoriatic arthritis, and post-traumatic arthritis was wrist fusion. 2 Although improvement in wrist pain from arthrodesis is often predictable and reliable, it comes at a major functional cost, most notably in mobility which results in dissatisfaction. According to Adey et al., 3 91% of patients who underwent total wrist fusion expressed a desire for a procedure that could restore wrist motion. As a result, Total wrist replacement (TWR) was developed with the intent of preserving motion while still providing pain relief. To achieve a pain-free, stable, and durable wrist replacement, proper patient selection, meticulous preoperative planning, and accurate implantation are essential. Low-demand patients with specific wrist motion needs tend to be the best candidates due to reduced risks of implant wear and loosening which indicated mostly for patients with end-stage rheumatoid arthritis (RA). With the evolution of TWR designs, the indication of TWR became wider and broader to include patients who suffered from end-stage osteoarthritis and post-traumatic arthritis. 4 Despite ongoing improvements in implant design and surgical techniques, complications after wrist arthroplasty remain common and can have severe consequences.5–11
TWR is, however, infrequently performed in Asia-Pacific region. We would like to share our case series with complications encountered during TWR and our experience in management.
Materials and methods
This study represents a single-center retrospective review of all patients who underwent TWR at the Department of Orthopedics and Traumatology, Prince of Wales Hospital in Hong Kong. The study period spans from 1 January 2004 to 1 March 2023. All patients included in the study were of Southern Chinese ethnicity. A retrospective review of all past medical records of the patients was performed. Prospective clinical follow-up assessment was arranged for those patients who had lost to follow up. A prior study 2 was conducted to report the surgical outcomes and experience of TWR in patients with advanced arthritis. In contrast, our current study will specifically address complications within our case series and highlight technical insights.
Surgical technique was performed similarly to that previously described for TWR. Generally, the wrist was exposed through a dorsal ligament-splitting approach using a distally based T-shaped capsular incision as described by Wan et al. 2 All surgeries were performed by the senior author (P-CH) or under his direct supervision.
The choice of implants was primarily influenced by their commercial availability in Hong Kong. For surgeries conducted between 2004 and 2006, biaxial implants from DePuy Orthopaedics Inc (Leeds, UK) were utilized. Subsequently, the ReMotion implant from Stryker (Kalamazoo, MI, USA) became the standard implant for the study. However, there was one case in 2012 where the Universal II implant from Integra (Plainsboro, NJ, USA) was used.
After the surgery, we immobilized the wrist for 10 to 14 days to promote wound healing and reduce swelling before initiating mobilization in the flexion–extension and circumduction planes. Early finger mobilization began within the first week to prevent finger stiffness, unless there was concurrent extensor reconstruction (which occurred in a few cases in our series). During the initial 2 weeks, we used the Muenster splint (also known as the reverse sugar tong splint) to protect the Darrach stabilization. Forearm rotation exercises were introduced after this period. Night splints were maintained for 6 to 8 weeks, and longer if the patient had preoperative flexion contracture or volar subluxation. All patients were referred to occupational therapists and physiotherapists for rehabilitation.
Patient gender, age upon surgery, pathology, types of implants, and follow-up period were recorded. Surgical details regarding implants and type of fixation used for each surgery were also documented. We defined our primary outcomes as postoperative complications and need for revision surgery. Secondary outcomes included time interval from surgery to complications, total number of revisions or subsequent procedure performed, and reason for revision.
Results
The research analyzed 12 wrists from 10 Chinese-Asian patients who underwent TWR. Their mean age at surgery was 61.4 years. Among the patients, 50% had Larsen grade V arthritis, 16.7% had grade IV arthritis, and 33% experienced volar subluxation. The average follow-up period was 97.4 months (ranging from 21 to 205 months). Complication rates included 16.67% for loosening, 8.3% for metallosis, and 8.3% for infection (Table 1). Survival analysis was shown in Figure 1 and Table 2.
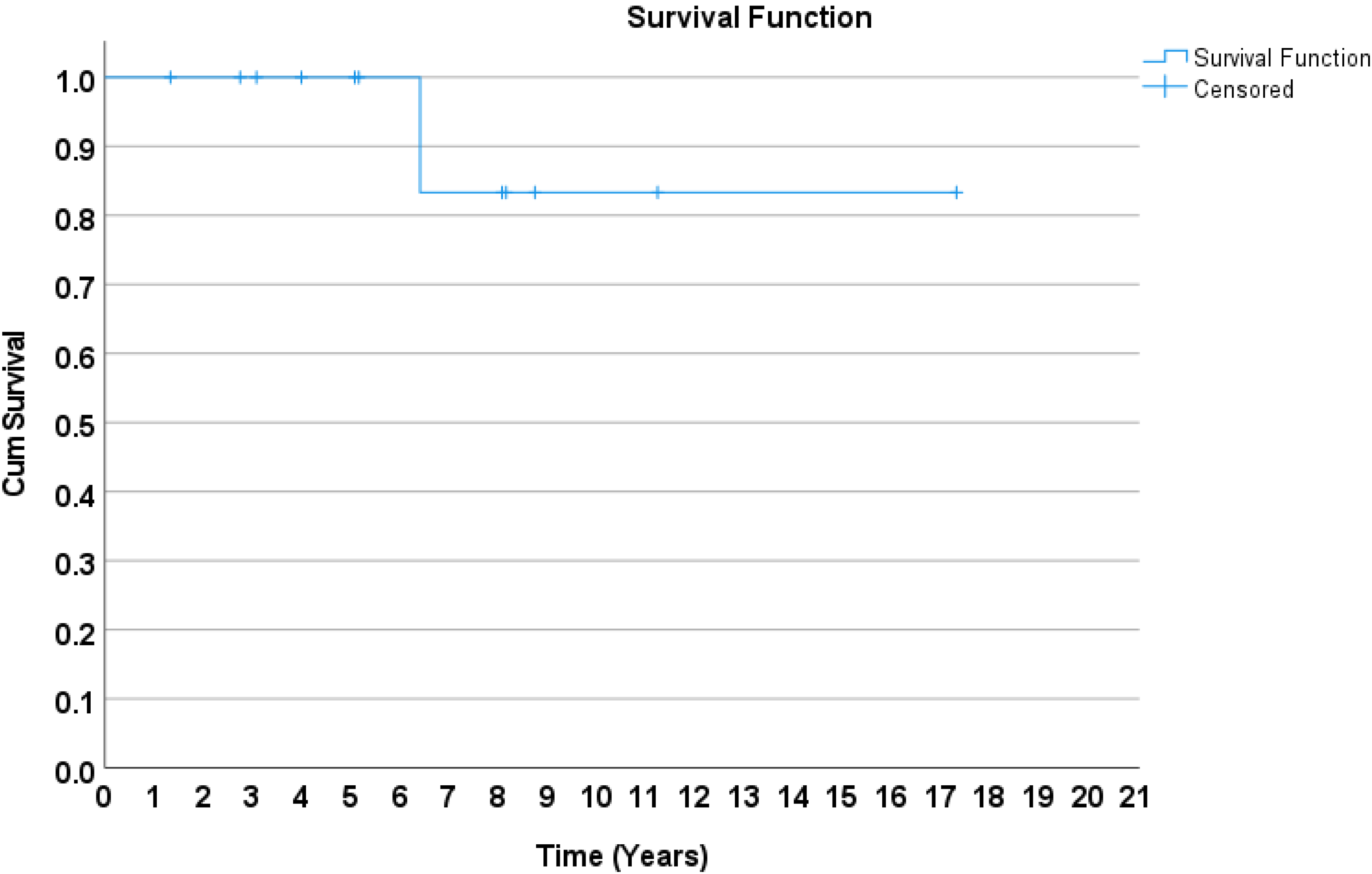
Survival analysis of total wrist arthroplasty.
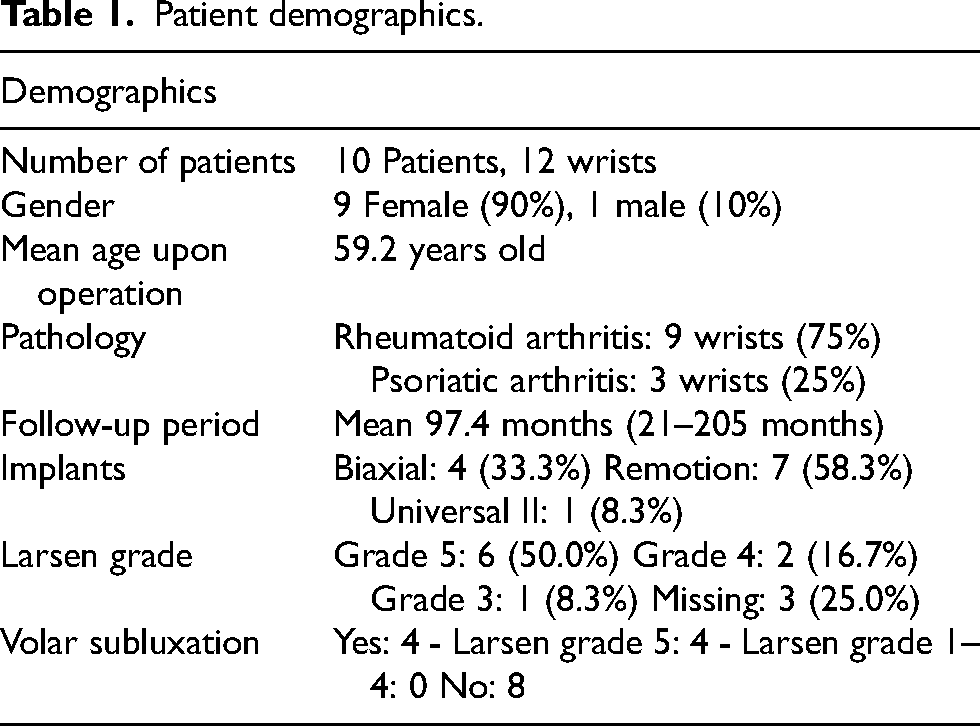
Patient demographics.
Summary of complications.
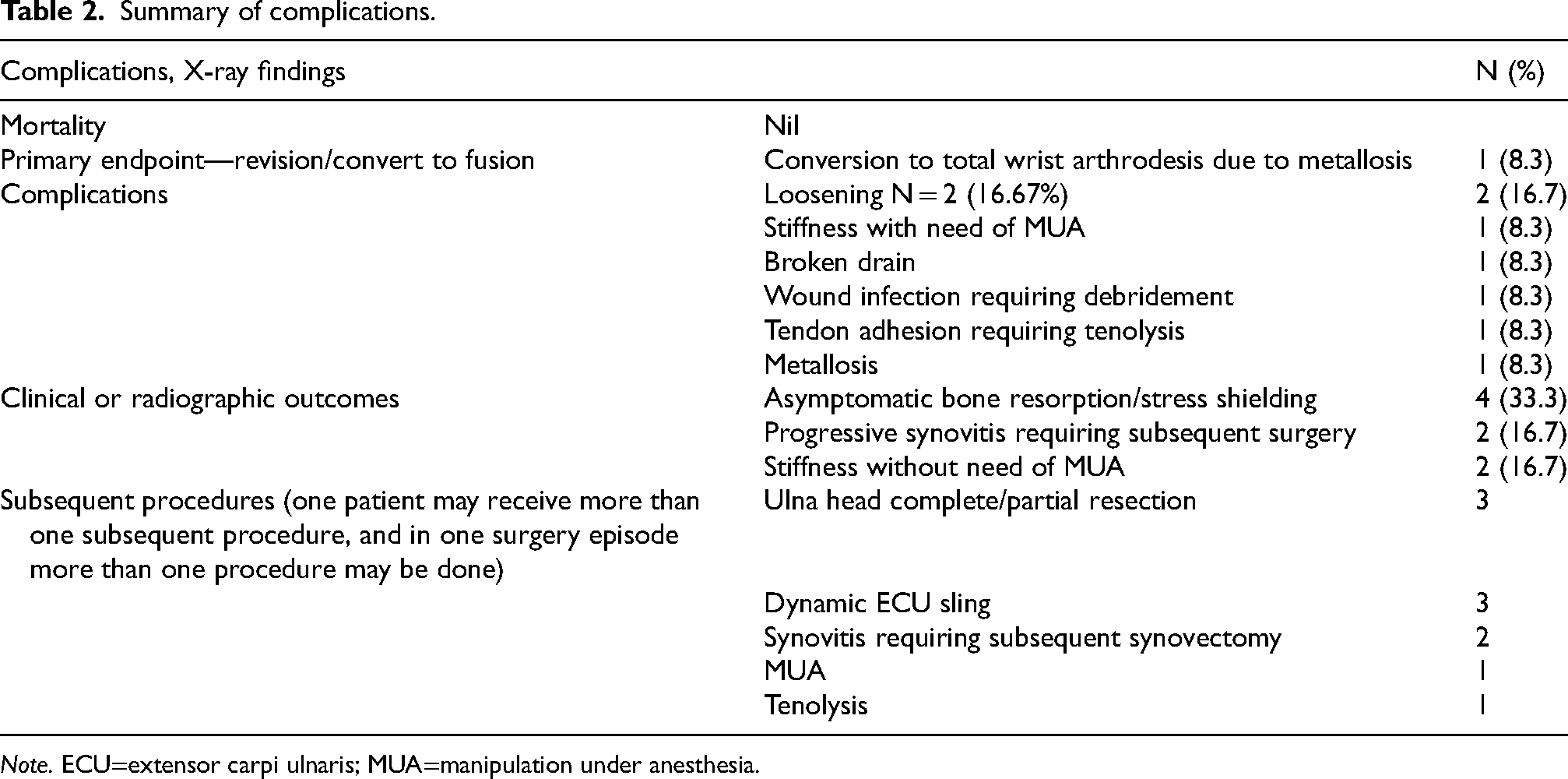
Note. ECU=extensor carpi ulnaris; MUA=manipulation under anesthesia.
Discussion
TWR is an attractive alternative to wrist fusion in which it preserves the range of motion for patients with painful wrist arthritis. Despite the less predictable outcomes associated with arthroplasty, patients often lean toward the potential functional benefits it offers. Takwale et al. 12 found that a majority of patients with RA, who underwent wrist arthroplasty on one side and arthrodesis on the other, expressed a preference for bilateral arthroplasties. We will discuss specific complications and our experience.
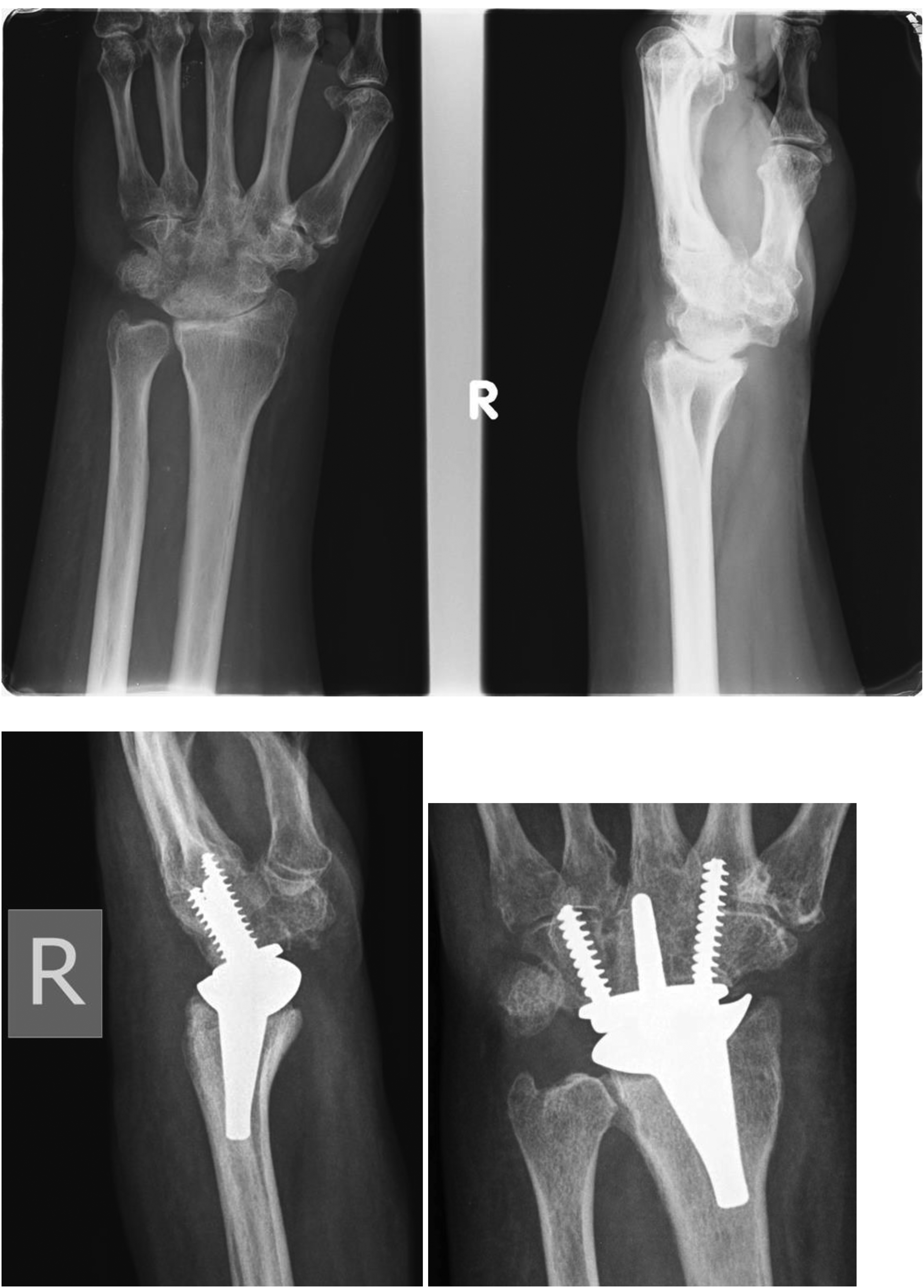
In the context of TWR surgery, complications related to the distal radioulnar joint (DRUJ) can be significant. Yeoh et al. 4 reported that approximately 16.7% of TWR patients experienced DRUJ complications necessitating further surgical intervention. Our clinical experience has led us to prefer the Darrach procedure to mitigate the risk of secondary DRUJ surgery in the future. Additionally, we utilize a dynamic extensor carpi ulnaris (ECU) sling to prevent stump instability. Despite distal ulna resection, we encountered a case with recurrent symptoms due to osteochondral overgrowth. Specifically, this patient was 68 years old with RA who underwent biaxial TWR in 2004. Although distal ulna excision was performed during the same surgery, stabilization of the distal stump was not carried out. Twelve months later, the patient presented with wrist pain and swelling, along with impingement sensations during ulnar deviation (UD) of the wrist. The diagnosis of ulna stump impingement was confirmed intraoperatively, revealing radiolucent osteochondral overgrowth. We excised the overgrowth along with part of the distal ulna stump and performed a dynamic ECU sling. The impingement symptoms resolved after surgery, and the patient remained symptom-free for 3 years until she succumbed to gastrointestinal bleeding (Figure 2).
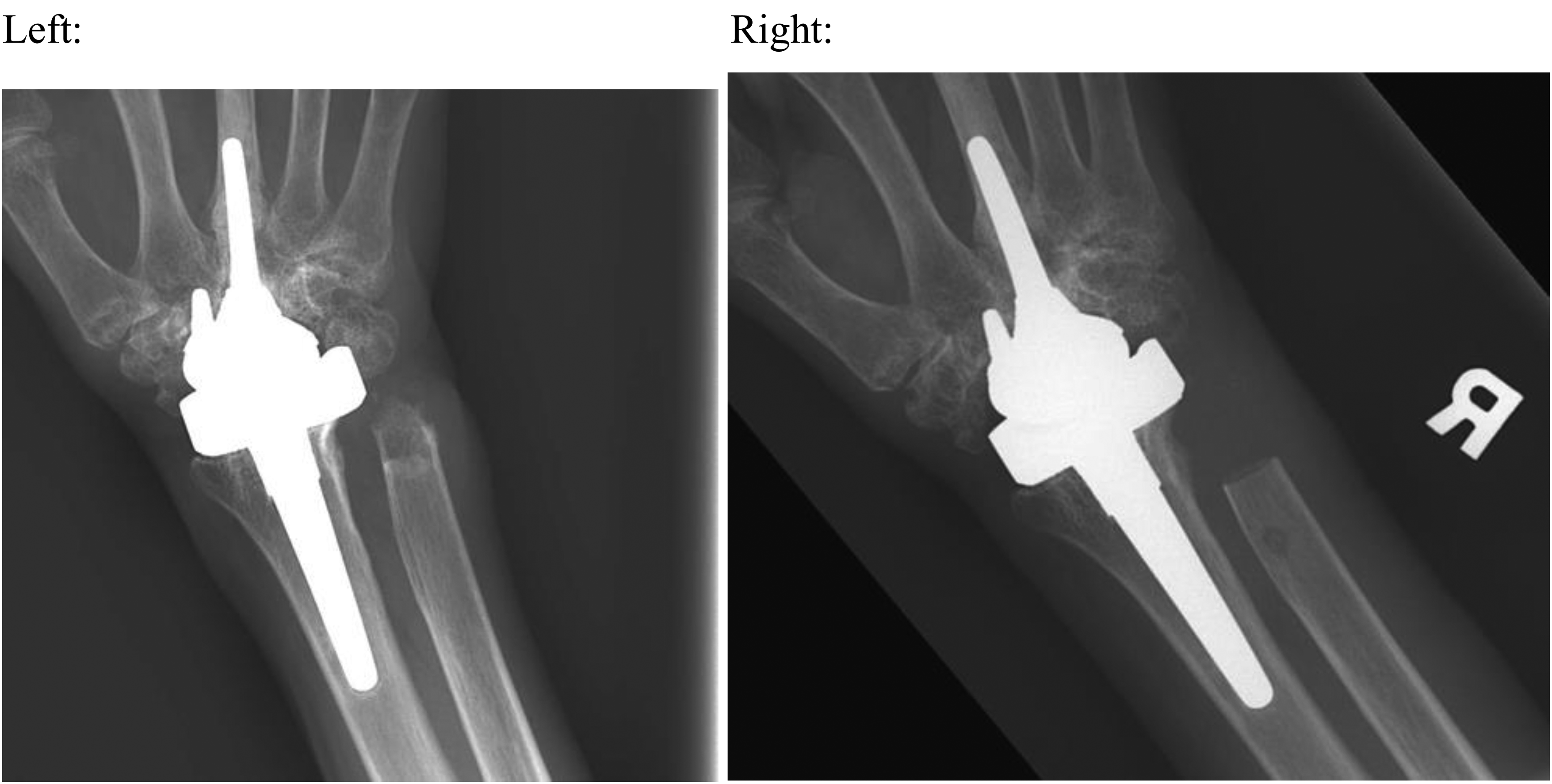
X-ray after osteochondral overgrowth before excision (left) and after excision (right).
Postoperative stiffness is a recognized complication following TWR. 13 In our series, we observed that patients with radiographically advanced and stiff wrists prior to surgery tended to experience more postoperative stiffness. However, further investigation and a larger sample size are needed to establish this correlation definitively. Poor preoperative mobility of the wrist cannot be expected to improve postoperatively, and patients should be counseled preoperatively regarding this to avoid high expectations. 14
We would like to share a challenging case from our experience: A 35-year-old female patient presented with advanced destructive wrist arthritis secondary to rheumatoid disease. She stopped medical treatment and relied on herbal medicine in mainland China. Her chief complaint was stiffness and functional limitation. Physical examination revealed UD of the wrist. Her range of motion was as follows: radial deviation (RD) 0°, UD 30°, extension −20°, flexion 55°, full supination/pronation. Grip strength was significantly reduced in the left wrist (<1 kg) compared to the right wrist (1 kg). Radiographs showed severe destructive arthritis, with a 65° volar inclination of the radial surface and a “hook of hamate”-shaped overgrowth extending to the volar cortex (Figure 3). We proceeded with TWR, using a small-sized carpal plate and radial component implant. To address stiffness and achieve balanced motion, we made a more liberal bone cut (2–3 mm beyond the usual) at the distal radius to allow shortening and tension relief. Intraoperative assessment demonstrated passive 50° flexion and 20° extension without subluxation risk. Given the imbalanced range of motion, we performed fractional lengthening of the flexor carpi ulnaris (FCU) tendon. Two cuts were made at the FCU musculotendinous junction with passive stretching. Additionally, we augmented the extensor carpi radialis longus and extensor carpi radialis brevis tendons (the latter affected by tenosynovitis) using a palmaris longus tendon graft anchored to the second metacarpal base with mini-mitek sutures. At the patient's last follow up (1 year and 9 months postoperation), her range of motion improved: extension 40°, flexion 40°, RD 5°, and UD 25°. All finger flexion-extension ranges were satisfactory.

Preoperative X-ray (upper row) and postoperative X-ray (lower row).
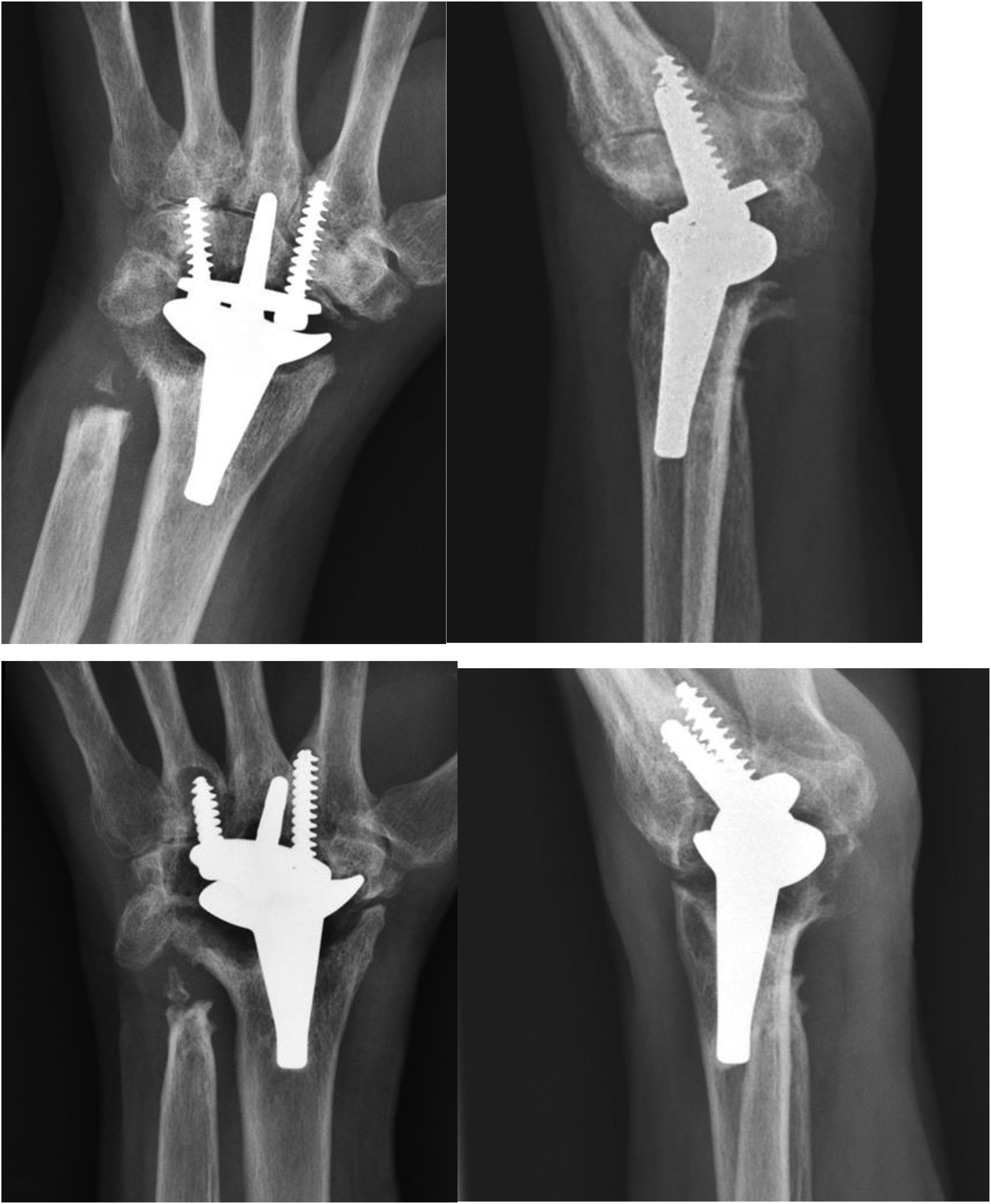
Another case is a 62-year-old woman with RA underwent TWR in 2011. Her preoperative range of motion was severely limited: extension 5 degrees, flexion 10 degrees. Notably, there was near-complete fusion of the mid-carpal joint and carpometacarpal joint. To address this, a revision TWR was performed. Intraoperatively it was found that the preserved radiocarpal joint (RCJ) has no cartilage and there was patchy fusion across the joint with severe arthrofibrosis. During the TWR, modification has been done. For the dissection part, after dorsal capsule has been opened, arthrofibrosis over RCJ was taken down and volar capsule contracture was relaxed, until carpus can be relaxed enough to flexion of 90 degree with distal radius surface exposed. During bone cut, due to the fusion and shortening of carpal bones, the native cutting guide could not be used and carpal cutting level had to be relied on eyeballing and X-ray. For this patient, as radial intramedullary guide insertion position is not ideal, therefore free-hand insertion under X-ray guidance was done. Afterwards, small-sized radial and carpal components were used. On table, the result range of motion and stability was considered appropriate. Postoperatively, the patient developed a superficial wound infection, which was managed with debridement on day 4 (Figure 4). On day 25, manipulation under nerve block (including the radial nerve dorsal branch, ulnar nerve and its dorsal branch, and median nerve and its palmar cutaneous branch) was performed without reopening the wound. Gentle manipulation under local anesthesia, with a short lever arm at the metacarpal and distal radius, improved the range of motion: extension 30 degrees, flexion 20 degrees, RD 15 degrees, and UD 20 degrees. Intraoperative Xi-scan revealed contact between the dorsal parts of both radial and carpal components during extension and RD. Postoperatively the patient again developed stiffness with minimal motion range 5 to 10 degree in all planes again. However, up to the last follow-up 41 months postoperation, she had no pain and no major effect on function. Her function score was 38 out of 40 and pain score 2 out of 20 (10%). She had no intention of receiving further intervention. She succumbed 4 years after operation due to metastatic sigmoid colon cancer.
Preoperative X-ray (upper row) and postoperative X-ray (lower row).
Stiffness may also occur for fingers. One patient with RA with biaxial implant surgery done back in 2004 complained all along weakness of active right little finger flexion, but full flexion under passive motion, since 2004. The active flexion of PIPJ was 0 to 20 degree and distal interphalangeal joint 0 to 10 degree. Tendon adhesion of both flexors is diagnosed. She finally agreed for tenolysis 5 years post-TWR. It was found that flexor digitorum superficialis and flexor digitorum profundus have adhesion over zone IV between dorsal surface of tendon and volar side of carpal bones. There was no wrist stiffness postoperatively.
Infection is a relatively uncommon complication. Althoff et al. 15 reviewed 1137 TWR patients and found risk factors for infection included advanced age >85, tobacco use, diabetes mellitus, chronic kidney disease, and depression. The infection rate was 3.5%. It is complicated by the fact that patients with inflammatory arthritis are using immunosuppressants.
Intraoperative fractures can occur on the radial side or the carpal side. Radial side fractures may result from inadequate preparation of the radius intramedullary canal. To guide broaching, the use of intraoperative xi-scan is recommended. If a fracture occurs on the radial side, cerclage of the radius and postoperative immobilization are necessary. Additionally, intensive mobilization should be performed to prevent stiffness. For carpal side fractures, consider using a longer stem and screws to bypass the fracture site. If bone stock is insufficient, cement augmentation is also an option. 1
Periprosthetic osteolysis is a well-described phenomenon after total joint replacement and is one of the most prominent reasons for revision surgeries. 16 When interpreting X-rays, it is common to observe stable, asymptomatic 1 to 2 mm radiolucent lines, which require monitoring and vigilance. Frank loosening manifests as progressive implant migration compared to bony landmarks and are often symptomatic, causing pain or instability during wrist motion. Boeckstyns et al. 17 suggest that in his study of 44 remotion implants, 84% developed <2 mm radiolucent lines, which did not correlate with loosening. These lines tend to stabilize within 2 to 3 years. Instability and loosening can result from either bony articulation loosening or loosening between the radial and carpal components. Bony loosening is diagnosed by comparing implant migration to fixed bony landmarks. Although loosening between components is less common with modern implant designs, it can still occur. Identifying high-risk populations, such as patients with RA and wrist abusers, is crucial. In patients with RA, loosening often results from a combination of poor bone quality, ongoing bony erosion, and soft tissue attenuation due to synovitis. In our series, there is high rate of asymptomatic bone resorption. After ruling out infection, they were observed and no revision was needed. The author would like to share one case of loosening. A lady suffered from psoriatic arthritis was 55 years old when receiving remotion TWR in 2014. First sign of osteolysis and bone resorption shows 2 years postoperation in 2016. There was progressive radiographic osteolysis and loosening, with migration of implant relative to bone. There was distal and volar migration of carpal implants, with fourth metacarpal volar cortex protrusion from one of the screws. The radial component remained stable, as evidenced by bone welding seen in lateral view, and static position relative to bone. Despite radiographic appearance, she is asymptomatic. Her range of motion is similar, from postoperative extension 20 degree flexion 10 degree to latest follow up (94 months postoperation) extension 20 degree, flexion 10 degree. Pain has much relief, from pain score 45% preoperation, 50% immediate postoperation, to now 20%. Her functional score was 31 out of 40 preoperation, 39 out of 40 immediate postoperation, and 34 out of 40 latest. She had disabilities of arm, shoulder and hand 28.3%, patient-rated wrist evaluation 19.5% in the latest follow up. Patient has no intention of revision surgery after explanation of loosening, as she is symptoms-free (Figure 5).
X-ray taken at immediate postoperation in 2014 (upper row) and 8 years postsurgery (lower row).
Advanced bone resorption and osteolysis cannot be viewed as equal of loosening, if there is no clinical instability or radiographic evidence. A 54-year-old woman with RA underwent biaxial TWR in 2005. Four years after the initial surgery, radiological features of osteolysis and bone resorption appear. Despite these radiographic changes, she remained asymptomatic. There is no radiographic sign of loosening or implant migration (Figure 6).

X-ray taken immediate postsurgery (left) and the latest X-ray taken 17 years postoperation with severe osteolysis (right).
Limitations of this study
This study's weaknesses include its retrospective nature and small sample size. There is a chance that some patients who did not experience complications during the study period might have later developed complications and sought medical attention elsewhere. Despite the limitations, our main purpose was to characterize the incidence, modes of failure associated with these surgeries and share our experience on these complications.
Conclusion
TWR is uncommonly performed in Hong Kong and Asia-Pacific. A major obstacle is inexperience in performing the surgery itself and managing its associated complications. The author has conducted a comprehensive review of our case series and our experience in managing complications. The authors hope this article can promote more knowledge and understanding about the procedure and its complication's management; then, more of this option can be offered to appropriate patient such that they have a motion-preserving choice.
Footnotes
Author's contributions
CT-KL and RC-WW were involved in conception of the study, acquisition, formal analysis and interpretation of data, and writing—original draft. W-WC contributed to formal analysis and interpretation of data, and critical revision of the manuscript. MC-KM and W-LT were involved in conception, supervision and administration of the study, acquisition, formal analysis and interpretation of data, and critical revision of the manuscript. P-CH was involved in supervision and administration of the study. All authors read and approved the final version of the manuscript.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
This study was approved by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee (Joint CUHK-NTEC CREC) with approval number 2022.112 on 27 April 2022.
Informed consent has been obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.