
Abstract
We examined the learning curve of Motec total wrist arthroplasty (TWA) of six experienced surgeons in their first 30 cases. Three times more complications/revisions were encountered in the first half of the study compared with the second half. Motec TWA surgery should be concentrated in a smaller number of centres performing higher volumes.
Complex surgical procedures are subject to a learning curve, with acceptance that initial outcomes may be poorer and surgery less efficient until the surgeon, and indeed the entire surgical team, master the procedure (Sarpong et al., 2020). In an accompanying article (Redfern et al., 2023), we detailed the complication and revision rates in a cohort comprising the first 30 Motec total wrist arthroplasties (TWAs) of each of six international surgeons in five centres (171 cases in total). In this article, we analyse the distribution of complications and revisions throughout those series to quantify the learning curve in Motec TWA.
Four surgeons supplied details of 30 cases each, one provided 26 cases and the final surgeon provided 25. Cases were numbered sequentially in chronological order from 1, their first Motec TWA, to 30. Complications were classified from zero (no complication) to five (conversion to fusion).
The series was analysed to assess whether the frequency and severity of complications altered with experience from the first to the 30th operation. Statistical analysis was performed using Fisher’s exact test with 95% confidence intervals and a significance of 0.05. The mean follow-up was 5.8 years (range 18 months to 12 years).
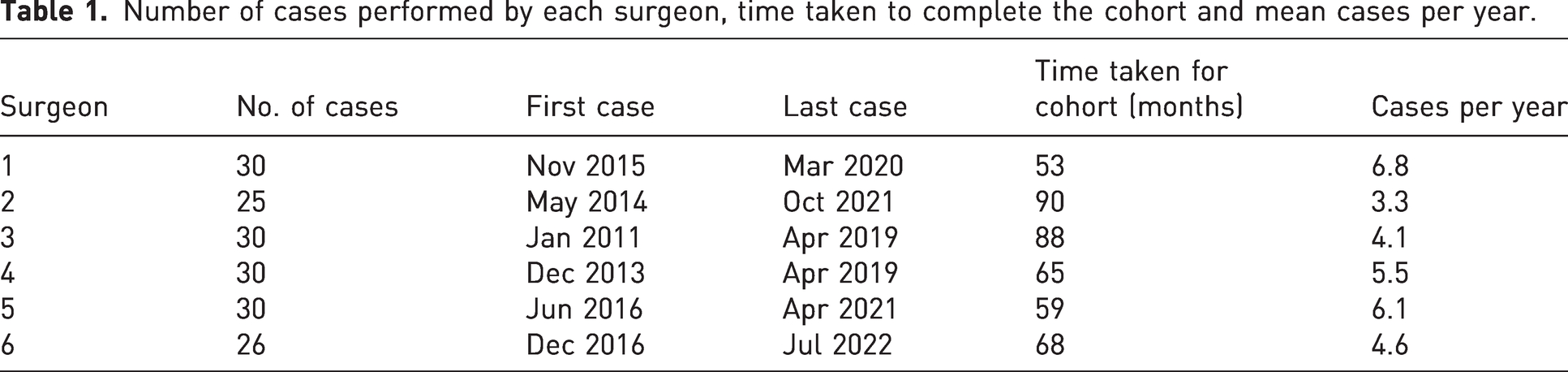
Table 1 details the number of cases by surgeon, the dates of first and last case, time taken to complete the cohort and mean cases per year. In total, there were 33 (19%) complications and 14 (8.2%) revisions across the series.
Number of cases performed by each surgeon, time taken to complete the cohort and mean cases per year.
The mean complication level by case number for the whole series (Figure 1) and the frequency of revisions by case number (Figure 2), both with trendlines, are shown.
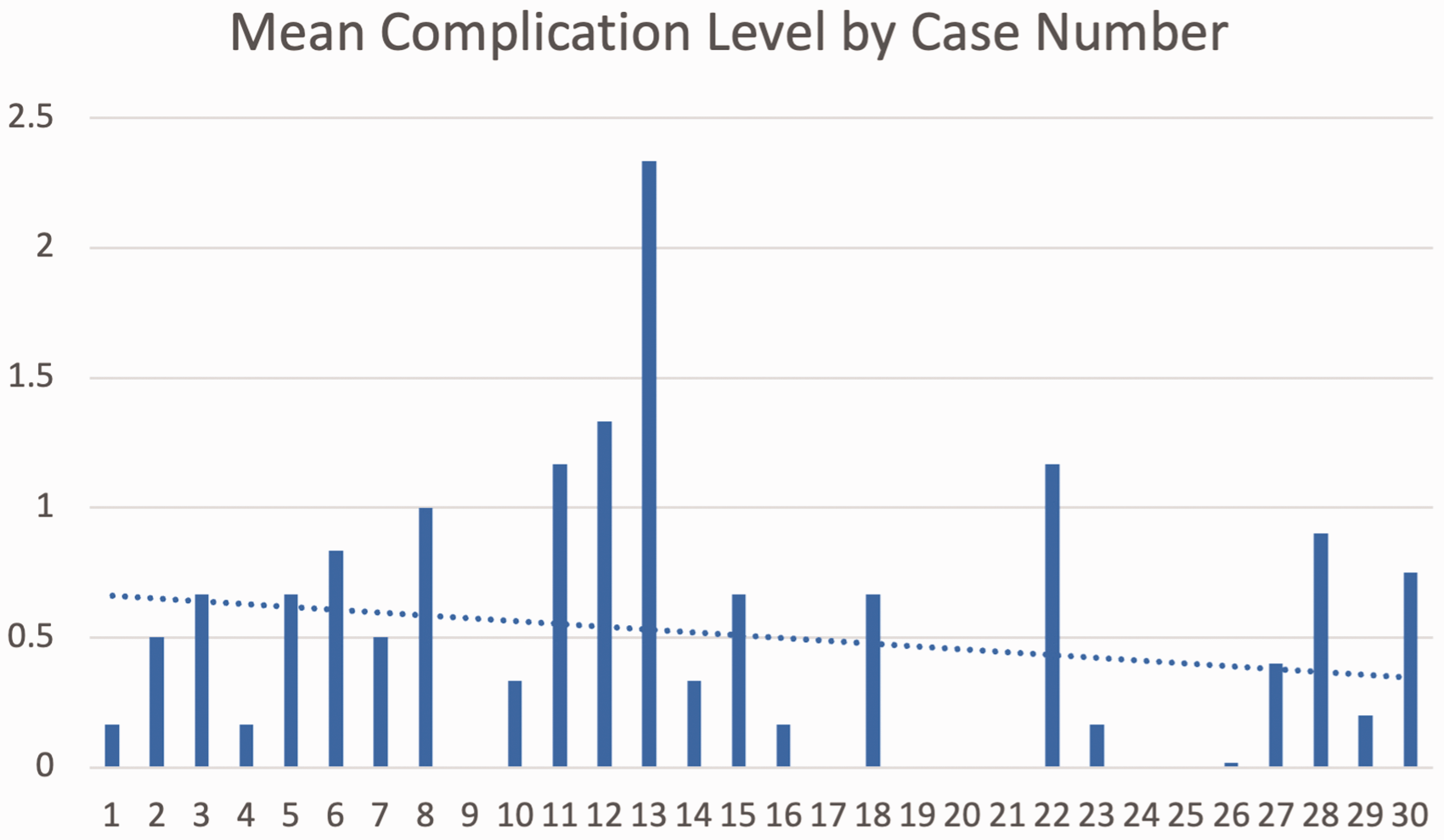
Graph showing the mean complication level for each case number across series (average of the complication levels of each of the six surgeons for each case) with trendline (dotted line).
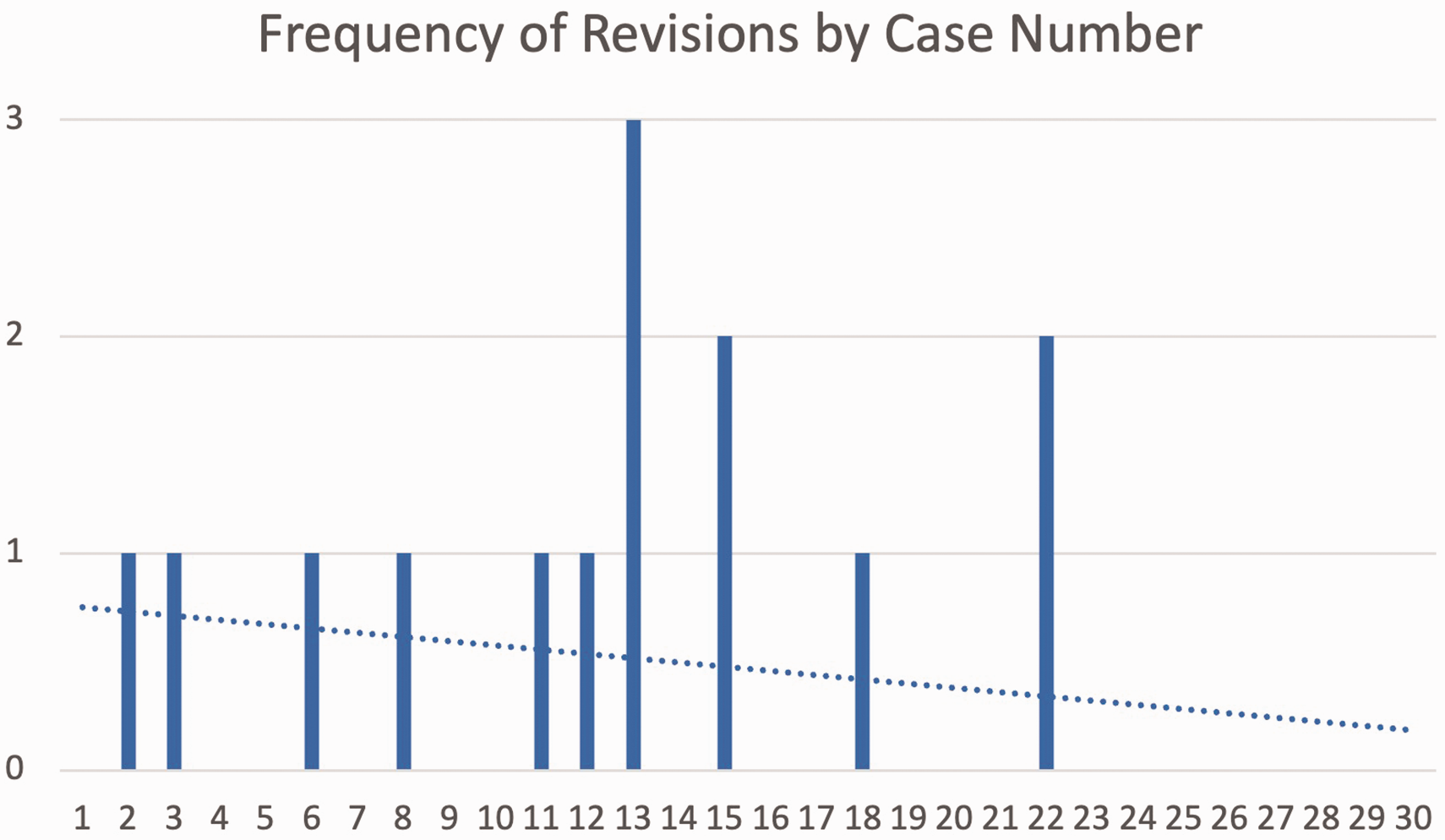
Graph showing the number of revisions for the whole series by case number with trendline (dotted line).
Analysing the complications in the first and second half of the series, there were 25 (28%) complications in 90 operations in the first half (sequential cases 1 to 15), compared to 8 (10%) complications in 81 operations in the second half (sequential cases 16 to 30) (p = 0.0024). Re-operations decreased across the two halves from 17/90 (19%) to 5/81 (6.2%) (p = 0.0109) and revisions decreased from 11/90 (12%) to 3/81 (3.7%) (p = 0.0377).
This study would suggest that there is a significant learning curve with the Motec TWA. Complication and revision rates are over three times higher in the first 15 cases performed by surgeons in this series compared with the subsequent cases.
Learning curves comprise an initial ‘steep’ part where the technique is being learnt, where efficiency is lower and complications are higher. It is followed by a ‘flattening out’ of the curve until a ‘plateau’ is reached where peak efficiency and optimum outcomes are attained. In lower limb arthroplasty, this learning curve is usually measured in number of cases or years of experience. Studies into learning curves traditionally use either time taken to perform the operation as a surrogate for efficiency, or patient outcomes or complication rates as a surrogate for accuracy. Studies in lower limb arthroplasty suggest the learning curve may be around 50 cases (Sarpong et al., 2020).
The results of our study support the concept of complex, and relatively low volume, operations being performed by a smaller number of surgeons, providing a sufficient volume of cases to surmount the steep part of the learning curve, and is the basis of the recommendations outlined by GIRFT (Getting it Right First Time) (Briggs, 2015).
Studying the number of 30 operations was an arbitrary decision based upon convenience rather than any power calculations relating to learning curves. It was the largest number we felt all the surgeons in the study would likely have performed in the time available. Assessing the difference in the first half of the study with the second half was again a decision of convenience. There may well be a continued decrease in complications when the number for each surgeon surpassed 30 procedures and the complication rate may only plateau after more than 15 procedures, but this would only strengthen the argument for increased volumes.
There are several potential confounding factors. As well as a learning curve for the surgeon, there is also a ‘learning curve for the implant’. Since its introduction in 2006, there have been minor changes to the implant and the accompanying surgical technique, with attempts to address issues such as bony impingement and impingement related osteolysis (Redfern et al., 2023). As several surgeons in our series were ‘early adopters’ of the Motec TWA, they may have had complications early in their series that might now, with current knowledge, be avoided. However, even if the six complications in the series that can be directly attributed to the ‘implant learning curve’ are excluded; the difference between the then 20 complications in the first half of the series and the seven in the second half remains significant (p = 0.0121).
Another potential confounding factor is how we learn to perform these surgeries. Three surgeons in our series were the first surgeons in their unit performing Motec TWA and, other than a possible cadaveric workshop, they essentially learnt on their own. Learning from someone else within a unit and dual operating (two senior surgeons operating together) are thought to be beneficial to increasing experience and reducing the time taken to pass the learning curve. There is also the issue of the time it takes to gain the experience. To learn from our experiences, we must remember our previous learning. Information that is not used tends to decay quite quickly, a concept known as Ebbinghaus’ ‘forgetting curve’ (Murre and Dross, 2015). In our series, surgeons were operating on 3.3–6.8 cases per year. Even operating at five cases per year, it will take three years to achieve the 15 cases that we feel are the minimum needed to achieve the plateau of the learning curve. It would seem logical that low-volume surgeons may see more effect of the ‘forgetting curve’ than the ‘learning curve’ and may never reach the level of experience required to get the best results.
It is also likely that prior experience of complex wrist surgery and arthroplasty may shorten the learning curve as many skills will be transferable. The surgeons in our series were all experienced wrist surgeons before their first Motec surgery and some had used other types of TWA previously. Two had experience of Motec TWA before doing these themselves. It is likely therefore that less experienced surgeons, with less prior exposure, may take even longer for the learning curve to plateau.
Finally, there is the concept of the ‘teaming curve’, where as well as the learning curve of the surgeon, there is also the learning curve of the whole surgical team (Xu et al., 2013). There is good evidence that surgery is more efficient, and outcomes are better when the whole surgical team are familiar with the technique and the implant.
This study shows that there is a significant learning curve with the Motec TWA. Adoption of the recommendations in this paper should facilitate results seen in the second half of our series, with complication rates of approximately 10% and early revision rates of 4%.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DB, SF, MS and TT are consultants for Swemac Innovation AB (Linkoping, Sweden). None of the authors received monies for any aspect of this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.