
Abstract
The aim of this study was to analyse the short- and medium-term complications of the Motec total wrist arthroplasty (TWA). Identifying exact modes of failure and their causes should allow surgeons to avoid or mitigate these risks in the future. Retrospective analysis of prospectively collected data from six hand surgeons at five international centres provided details of 171 Motec TWAs. The mean follow-up was 5.8 years (range 18 months to 12 years). There were 33 (19%) complications within our cohort, with a revision rate of 8.2% (14 revisions). There was no difference in complication rates between metal-on-metal and metal-on-polymer articulations. Failure of osseointegration was the most common complication. Problems with soft tissue balancing, implant impingement related osteolysis, bony impingement and metacarpal fracture were found to be other preventable causes of failure in this series. Elimination of these preventable complications will improve survival rates for this implant.
Introduction
Severe arthritis of the wrist joint is a debilitating condition leading to decreased functional performance and quality of life due to pain, reduced range of movement (ROM) and diminished grip strength. When conservative measures fail, traditional surgical management includes neurectomy, proximal row carpectomy, and partial and total wrist fusion. Total wrist arthroplasty (TWA) has been introduced as an alternative to these, with the aim of preserving movement. Earlier TWA implants showed good results initially; however, high complication rates and low survivorship resulted in these being removed from the market. Newer, so-called fourth-generation implants have shown greater promise with longer survivorship and fewer complications (Murphy et al., 2003). One such implant, the Motec TWA (Swemac Innovation AB, Linköping, Sweden) has survival rates of 86% at 10 years (Reigstad et al., 2017). The Kaplan–Meier survival curve from this paper shows most of the failures in that series occurred early, within the first 2 years after implantation.
The Motec TWA is a high mobility modular prosthesis with radial and metacarpal screws made of blasted titanium alloy (Ti6Al4V) coated with Bonit® (calcium phosphate), comprising a distal Cobalt-Chrome-Molybdenum (CoCrMo) ball and a proximal CoCrMo, or carbon fibre reinforced polyether ether ketone (PEEK) socket. Data from the largest single-centre cohort of TWA to date suggest this prosthesis has shown promising long-term outcomes with acceptable levels of complications (Reigstad and Rokkum, 2018).
Given the relative novelty and lower surgical volumes of TWA prostheses performed, in comparison to major joint replacements such as total knee or hip, information regarding the rate and type of these complications remains limited, especially outside the unit that developed the prosthesis.
The aim of this study was to quantify the rate of the various short- and medium-term complications of the Motec TWA by interrogating a large dataset from multiple surgeons performing Motec TWAs. Further, we aimed to identify the exact modes of failure and their causes, to allow us make recommendations on how to avoid or mitigate these risks in the future, reduce the number of early reoperations and improve the long-term survival of this implant,
Methods
A retrospective non-interventional analysis of prospectively collected complication data was obtained from six high-volume surgeons from Newcastle (Australia), Cape Town (South Africa), Linkoping (Sweden), and Southend and Liverpool (United Kingdom). The individual surgeons collected their own anonymized complication data from their own initial cohorts of primary Motec TWAs and submitted this to the authors for collation into a centrally stored database. All data was collected using a standardized data collection form. Data regarding the articulation used, whether metal-on-metal (MoM) or metal-on-polymer (MoP), was also recorded.
Details of the complication and its cause, where applicable, were collected by ‘free text’ from the surgeon to allow thematic analysis and classification of the whole cohort. Complications were grouped into different mechanisms. Whether these complications are ‘definitely preventable’ with current knowledge and improved techniques, ‘potentially preventable’ or ‘unpreventable’ is also discussed.
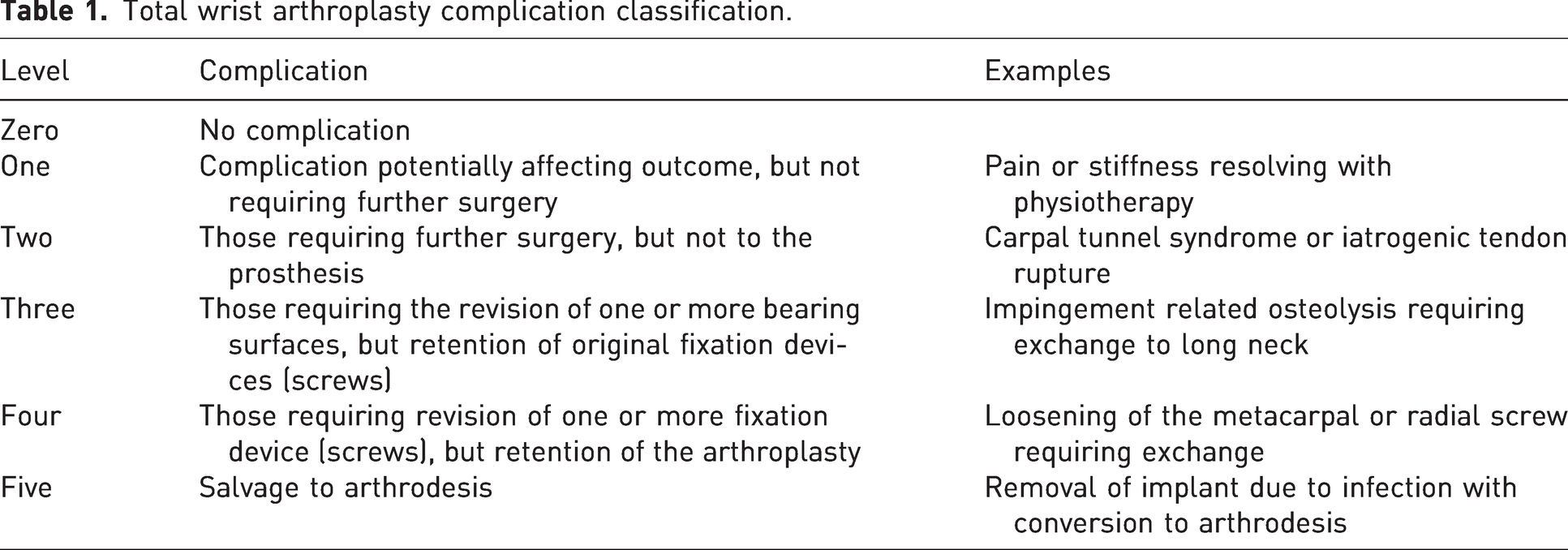
Complications were classified, in the range of 0–5, by the consequence they have for the patient, the requirement for further surgery and the survival of the implant. The classification is detailed in Table 1.
Total wrist arthroplasty complication classification.
Complications were recorded if they occurred at any time from the operation to 5 years postoperatively. Statistical comparison of the complication rates between the MoM and MoP groups was performed using Fisher’s exact test with a significance of 0.05.
Results
Details for 176 Motec TWAs were collected from 159 patients, performed between 24 January 2011 and 28 October 2021. After five cases were excluded, 171 index procedures performed on 153 patients were included in the final analysis. Four patients were excluded due to incomplete data and one patient was excluded for undergoing revision surgery rather than a primary procedure. There were 113 MoM articulations and 58 MoP articulations. All six surgeons would be classified as highly experienced wrist arthroplasty surgeons (level 4 or 5) according to Tang and Giddins (2016).
Data analysis was performed in 2022 but complication and revision data were reconfirmed to be accurate at the time of submission (April 2023). Although we only recorded complications occurring in the first 5 years postoperatively, this gave a mean follow-up of 5.8 years (range 18 months to 12 years).
Complication rates
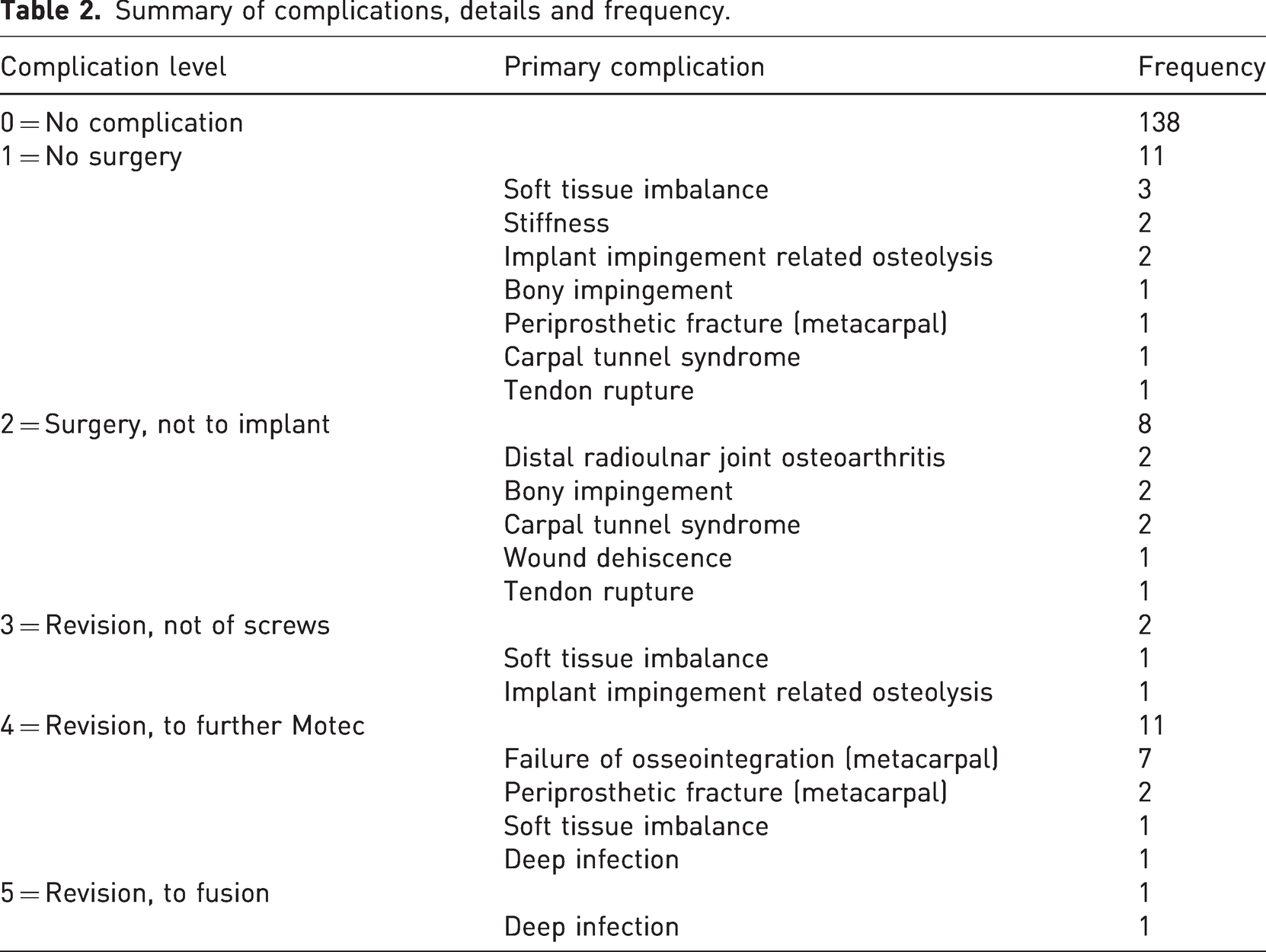
We found 33 (19%) complications overall within our cohort of 171 cases; 11 complications did not require further surgery, 21 required further surgery and, of these, 14 required revision surgery with one requiring revision to fusion. Our revision rate was 8.2% overall and the 5-year Kaplan–Meier survival curve for the cohort is as shown in Figure 1. Breakdown of complications by arthroplasty complication level and frequency is detailed in Table 2.
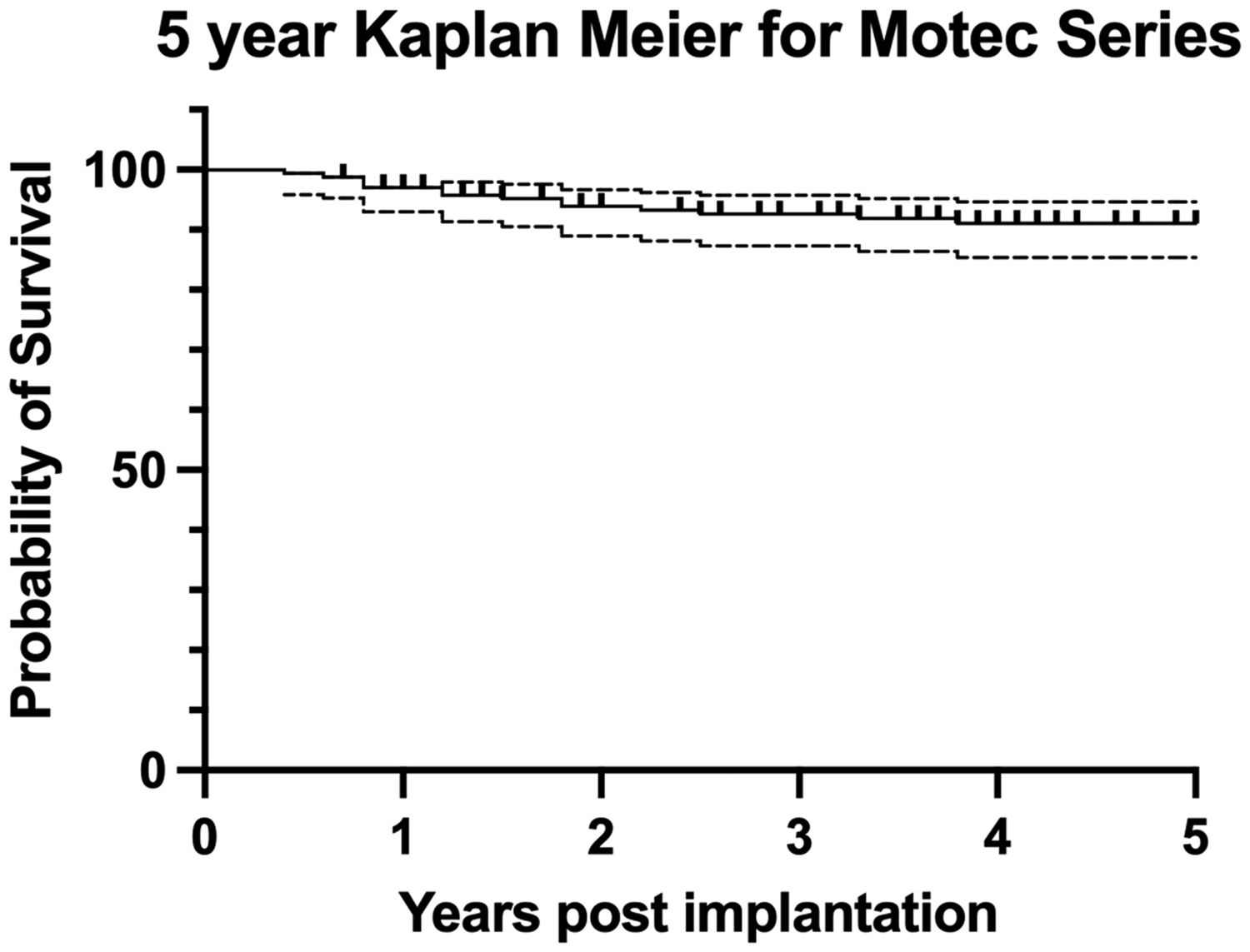
Kaplan–Meier survival curve for the series. Dotted lines represent 95% confidence intervals.
Summary of complications, details and frequency.
Mean time to failure was 591 days (range 131–1400) for patients requiring any form of revision surgery. Time to failure for each individual case of revision is represented in Figure 2.
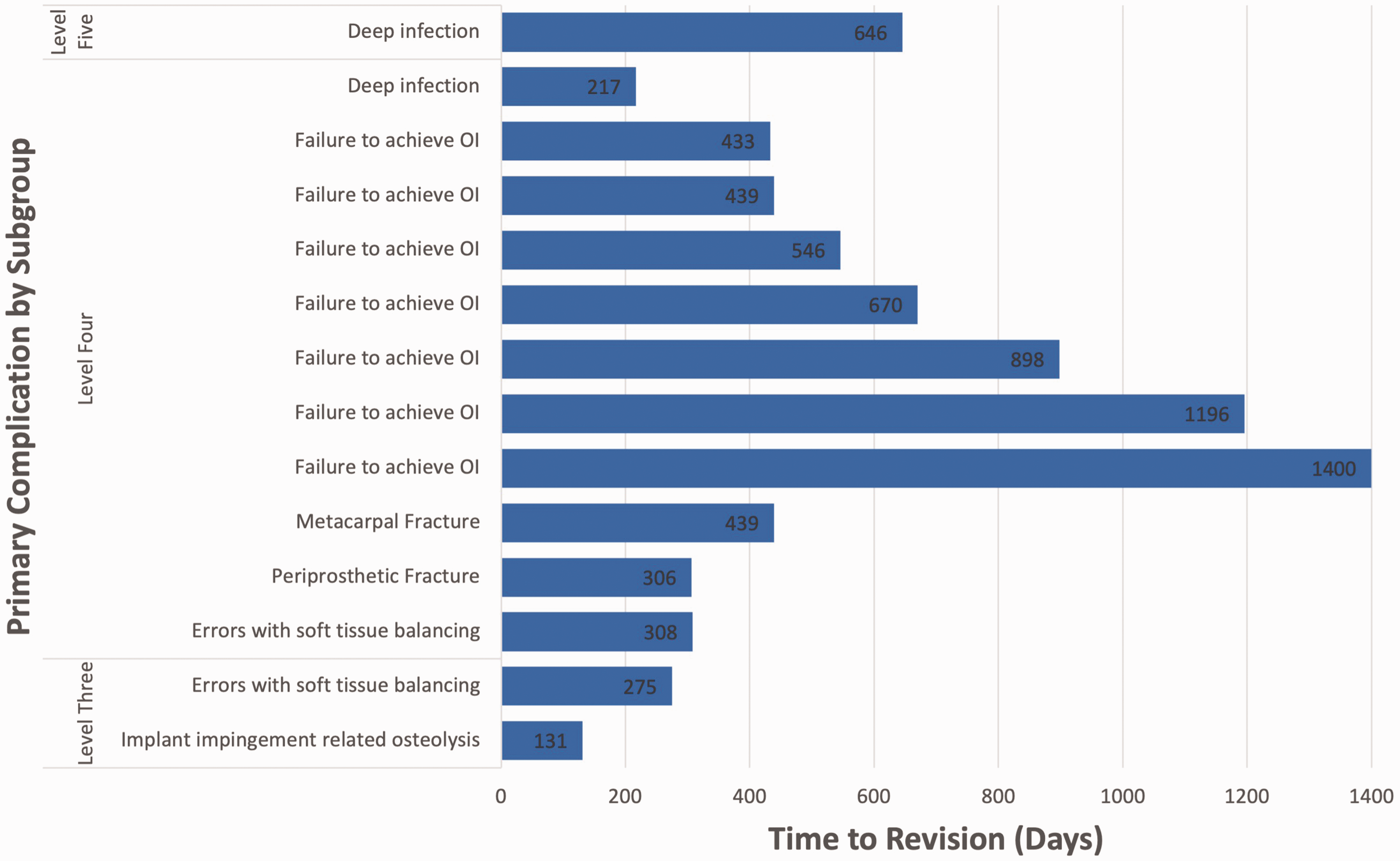
Bar chart displaying time from original surgery to revision by reason for revision and complication level, for each case of revision. OI: osseointegration.
There was no discernible difference when comparing the two types of articulations: 22 (19%) complications occurred in the MoM group compared to 11 (19%) in the MoP group (p = 1.00); and 9 (8.0%) revisions in the MoM group compared with 5 (8.6%) in the MoP group (p = 1.00).
In terms of whether the complications were avoidable, the consensus was that 6 of 33 (18%) of the complications are ‘definitely preventable’ and a further 20 of 33 (61%) are ‘potentially preventable’, and only 7 (21%) of the complications and two of the revisions are considered truly unpreventable.
Discussion
In this study, we analysed prospectively collected complication data of patients treated with the Motec TWA, from six surgeons in five centres. Our reported complication rate of 19% compares favourably with a large single surgeon study by Reigstad and Rokkum (2018), with a reported 32% complication rate (35 in 110 Motec TWA). Our rates also compare well with a more recent randomized controlled trial comparing Motec TWA with another implant that had complication rates of 35% and revision rates of 15% for the Motec group (Holm-Glad et al., 2022). A systematic review of TWA complications found a 31% complication rate in arthroplasty cases over a range of generations and devices, though this complication rate dropped to 13% in later fourth-generation models (Berber et al., 2018). The complication rates found in this study also compare well with those from total wrist fusion. Hazewinkel et al. (2020) found a 33% complication rate in 215 patients, with 19% of patients requiring a second operation. In a systematic review, Berber et al. (2018) found an overall complication rate of 28% for arthrodesis. Interestingly, Adey et al. (2005) found that although 15 of 22 patients (68%) were satisfied by the results of their fusion, 14 of 22 (64%) had significant ongoing wrist pain and 20 of 22 (91%) would undergo a further procedure that could make their wrist move again if one was available.
Our study did not see any difference in complication or revision rates with different articulations and, as such, our data do not support the statement by Holm-Glad et al. (2022) that recommended ‘discontinuing the use of MoM in TWA’ in favour of MoP; a statement which was based upon three cases of unclassified osteolysis, presumed but not proved to be the fault of the articulation in a series of 40 MoM implants.
In our study, certain complications are listed across multiple arthroplasty complication levels, dictated by the requirement for, and invasiveness of, surgical intervention required. For example, a patient with implant impingement osteolysis who presented with no major symptoms could be treated conservatively and be considered a level one complication. However, if this led to unacceptable pain, an articular component revision would be a level three complication, and if it caused significant osteolysis, a level four revision of a screw may be required.
Failure to achieve osseointegration of the metacarpal screw is the commonest complication and cause of revision in this series (seven patients). It is characterized by progressive lucency around the distal component with distal migration of the metacarpal implant (Figure 3a and b), usually associated with pain. If untreated it can lead to the implant cutting out of the metacarpal (Figure 3c). All patients who developed this complication required revision of the metacarpal screw. Primary stability is caused by the screws engaging with the bone, but for long-term stability bone must grow into the surface of the titanium, which is facilitated by the calcium phosphate coating. Failure to achieve osseointegration has been attributed to issues such as poor patient biology (severe rheumatoid arthritis, diabetes, osteoporosis, smoking and advancing age) and medications (such as steroids, bisphosphonates and anti-inflammatories) (Gaston and Simpson, 2007). In this study, however, our opinion is that poor primary fixation and reduced bone–screw interface caused by inadequate screw length and/or width remains the most likely cause of this issue as has been seen with other implants (Apostu et al., 2018).
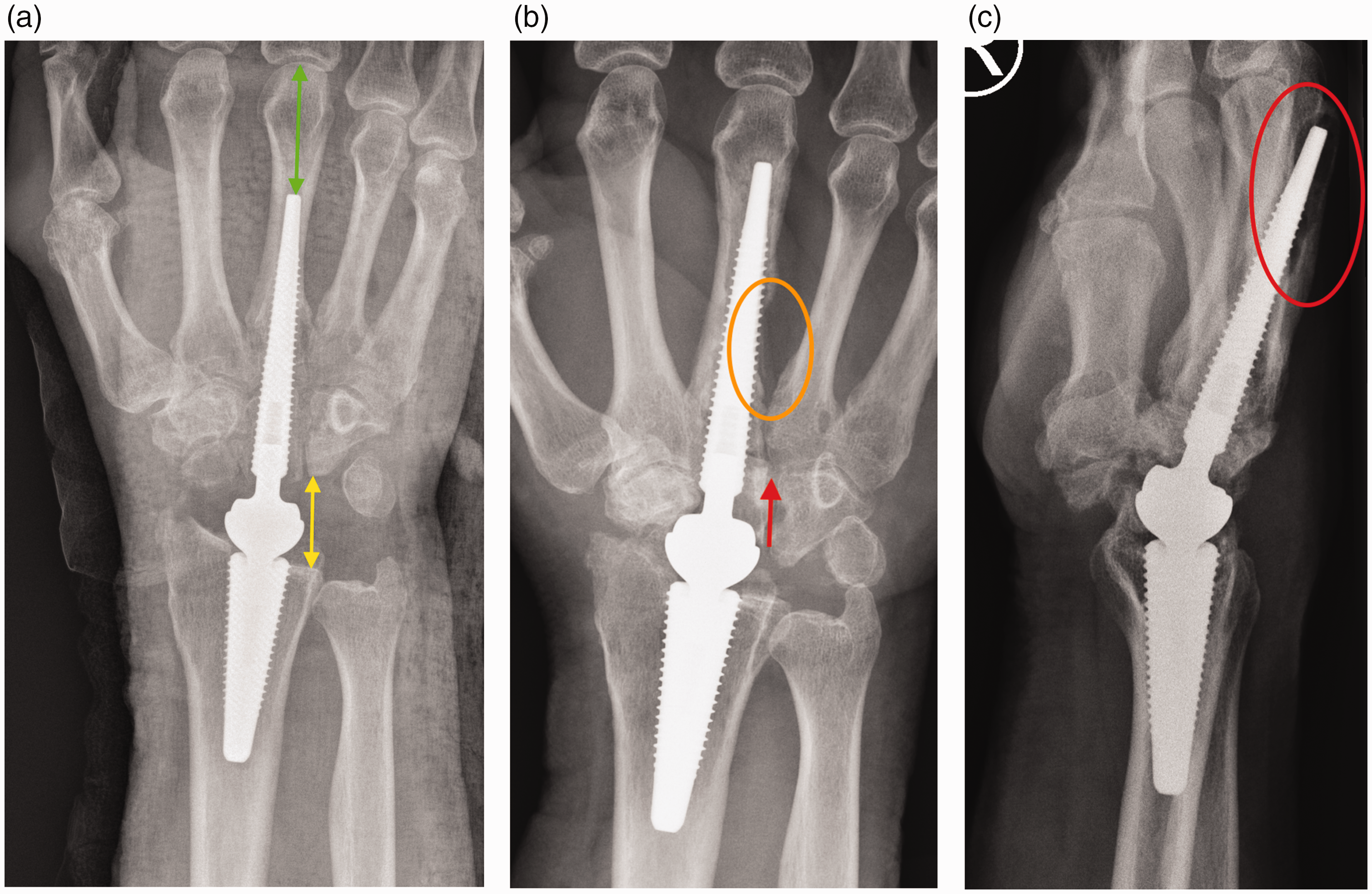
Images of failure of osseointegration. (a) Initial position (note distance from screw tip to metacarpophalangeal joint – green double-headed arrow and joint space – yellow double-headed arrow); (b) distal migration of screw (note change of position of screw in capitate – red arrow) and lysis and (c) implant penetration of dorsal cortex– red oval.
Patients requiring revision of the metacarpal screw generally had a screw that did not pass the isthmus or were too narrow to engage the cortex (Figure 3a) just proximal to the isthmus, and as a result, lacked sufficient stability for osseointegration to occur. The manufacturer’s surgical technique suggests performing a 15° closing wedge osteotomy of the third carpometacarpal joint (CMCJ) to bring the long axis of the capitate into alignment with that of the third metacarpal, which facilitates the placement of a longer screw. This technique has been adopted by four of the six surgeons in this series. As the size and position of the screw are under the direct control of the surgeon, we feel this complication is potentially preventable. Interestingly, there were no failures of the radial screw component in this cohort (although the authors have seen it in other patients). This may be due better bone stock than in the metacarpal region, or possibly due to the fact it is easier to correctly position and size this screw.
Another potentially preventable complication was errors of soft tissue balancing. This group of complications included ‘overstuffing’ of the prosthesis, soft tissue imbalance leading to resting deformity or instability, and incorrect positioning of the centre of rotation of the implant. ‘Overstuffing’ (implanting too large a prosthesis for the space available) leads to over-tensioning of the surrounding soft tissues, leading to pain and reduced ROM and has been seen in most other forms of arthroplasty (Geervliet et al., 2019). This can be prevented by proper countersinking of the prostheses into the radial and capitate/metacarpal segments, and by sufficient joint capsule release. By adjusting the length of the neck, final adjustments can be made once the implants are seated. This is considered as a potentially preventable cause of failure.
Soft tissue imbalance is most commonly seen in patients with inflammatory arthropathies and often occurs when there is pre-existing radial deviation of the wrist and/or ulna deviation at the MCP joints. This deformity may be exaggerated postoperatively with the Motec prosthesis due to its unconstrained (ball and socket) nature. It can be to some extent avoided by soft tissue releases, tendon transfers (extensor carpi radialis longus to extensor carpi ulnaris) and concurrent MCP joint replacements and/or realignment.
The ideal position of the centre of rotation for this prosthesis has not yet been identified. It is anticipated that this will lie somewhere between the original radiocarpal and midcarpal joints and more errors occur by placing this too proximally. It is anticipated that ongoing research on this issue and the possible use of 3D templating tools will eventually help surgeons in this regard.
A third preventable complication is impingement related osteolysis. This has been an issue with this prosthesis and is due to wear debris caused by impingement between the edges of the articular components at the extremes of movement (>67°) (Julian et al., 2023; Reigstad and Rokkum, 2018). This only seems to occur with the short-necked prosthesis when the harder CoCrMo cup edge causes damage to softer titanium metacarpal screw leading to localised metallosis, or when the titanium edge of the distal titanium screw causes damage to the edge of the PEEK cup producing polymer debris, an inflammatory reaction, and loosening (Karjalainen et al., 2018). By avoiding the short neck this complication is preventable. We have not seen osteolysis that cannot be explained by this mechanism.
A fourth preventable complication is bony impingement, largely due to the earlier operative technique not recommending removing the entire proximal carpal row, where removal of the triquetrum and distal scaphoid were considered optional. However, issues with impingement between the distal scaphoid and the radial styloid and the triquetrum on the edge of the cup have led to modifications of the Motec TWA technique with full proximal row carpectomy now mandated and radial styloidectomy performed in addition as required. In our opinion, this complication is therefore preventable.
Symptomatic distal radioulnar joint osteoarthritis (DRUJ OA) developed in two patients postoperatively within our cohort and was treated with an ulnar head replacement (hemiarthroplasty) or excision (Darrach’s procedure). Though technically an unpreventable complication, and one not related to the Motec TWA, it is advisable to assess the DRUJ preoperatively to ensure that this condition is not concurrent with the wrist arthritis as, if present, both can be surgically treated at the same time.
There were two metacarpal fractures in the series, one intraoperative and one postoperative. Although periprosthetic fractures can occur with any implant, it is thought that cortical damage (‘notching’) of the dorsal metacarpal shaft at the time of reaming may make this more likely and is therefore potentially preventable. A closing wedge osteotomy to align the long axes of the capitate and third CMCJ prevents this ’notching’.
Tendon ruptures were caused by overly dorsal placement of implants in the radius or from damage during the reaming process. All patients required surgery to repair the tendon injury; however, only one required revision of the implant. With careful protection of the soft tissues during the surgery, and by attentive placement of implants, this should be preventable.
Stiffness, with or without ongoing pain, was a relatively common complication, though this did not lead to further surgery in our series. This is an unpreventable complication and is seen in all arthroplasty surgery and is thought to be due to scarring or fibrosis, a reaction to one of the metallic elements of the implant or unrecognized ‘overstuffing’. This was successfully treated with rehabilitation and physiotherapy in our patients. One case of carpal tunnel syndrome occurred in the context of a postoperative haematoma in the days after surgery and required carpal tunnel release. A further patient complained of carpal tunnel symptoms; however, these resolved with conservative management. Ulnar nerve compression was also encountered in two cases. In one, this was caused by ‘overstuffing’ of the prosthesis and required revision, whereas bony impingement with soft tissue imbalance caused the other.
Infection, though rare, is devastating in TWA as with all arthroplasty surgery (Berber et al., 2018). In this study, one case underwent a two-stage revision and the other explantation and wrist fusion. These were considered unpreventable complications, though with careful aseptic technique, MRSA clearance and preoperative antibiotic prophylaxis the risk can be minimized (Alamanda and Springer, 2019). Interestingly, there were no documented issues of dislocation in this series, although there are two reported cases in the literature (Giwa et al., 2018; Reigstad and Rokkum, 2018).
As detailed above, 18% of these complications are ‘definitely preventable’ and a further 61% are ‘potentially preventable’, and with knowledge of their causes and ways to avoid them, it is hoped that the rates of these early complications will be reduced. Indeed, in this series, only two of the revisions are considered truly unpreventable. These complications are not unique to our study and are almost certainly the reason why Motec Kaplan–Meier survival curves show an approximately 10% revision rate in the first 2 years after implantation (Reigstad et al., 2012), after which the survival curve flattens out, suggesting that once the implant is fixed and functioning well it is likely to survive into the long term. It is for that reason we have only looked at the short- to medium-term complications, i.e. those occurring within the first 5 years after implantation, using the criteria set out in a systematic review of the reporting of arthroplasty outcomes (Ahmad et al., 2021). Further, the complications listed in this study may not be the cause of the eventual, ‘late’, failure of a well-fixed and well-performing implant.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DB, SF, MS and TT are consultants for Swemac Innovation AB (Linkoping, Sweden).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.