
Abstract
Purpose
Acetabular fractures are challenging injuries in the heterogeneous population of elderly patients. In patients able to partially bear weight, open reduction and internal fixation (ORIF) is indicated. In frail patients, ORIF combined with primary total hip arthroplasty (THA) allows early weight-bearing to preserve independence. This article systematically analyses a treatment algorithm that separates fractures into stable fractures treated conservatively and fractures needing surgical stabilization with osteosynthesis or osteosynthesis plus arthroplasty, dependent on patient characteristics but less on the fracture classification or energetic impact of the trauma.
Methods
Data on patients ≥50 years of age treated for acetabular fractures (2009–2019) were retrospectively analyzed. The primary outcome was loss of independence. In-hospital complications, length of stay, re-operations, the need for walking aids, and pain were analyzed as secondary outcomes.
Results
Out of 207 patients, 135 were male, average age was 70 years. Eighty-five patients were treated conservatively, 89 ORIF, and 33 ORIF plus arthroplasty in one operation. The initial morbidity of patients treated with the combined operation was higher than osteosynthesis alone, but the long-term outcome was favorable with less pain and fewer secondary interventions. Age and female gender were associated with the decision to treat the fracture with the combination of osteosynthesis and arthroplasty.
Conclusions
The results suggest that aged and potentially frail patients with acetabular fracture have better long-term outcome after ORIF combined with arthroplasty at the price of an initially higher risk of adverse outcomes. Females were more frequently treated with the combined operation independent of other risk factors
Keywords
Background
Acetabular fractures in elderly patients are a relevant public health concern due to the aging of societies,1–3 an increase in the rate of this injury, 4 as well as an increasing prevalence of high-energy trauma, 5 have been observed. In elderly patients, the treatment aims at early mobilization to preserve mobility and thereby independence. 1 Although joint preservation accordingly is not the primary aim of treatment, for active elderly patients able to partially bear weight, open reduction and internal fixation (ORIF) remains the treatment of choice. In older patients, poor bone quality and other unfavorable prognostic factors such as marginal impaction, relevant displacement, and/or preexisting osteoarthritis are common.5–7 These factors increase the risk for a secondary operation after ORIF7–9 with potentially inferior outcomes.10,11 To facilitate early full weight-bearing and avoid the risk of secondary surgery, ORIF and total hip arthroplasty (THA) in one operation (ORIF + THA) have gained popularity. Given the heterogeneity of the elderly population, treatment approaches are highly individualized. Traditionally, fracture morphology had been in the focus for the decision of the therapeutic strategy. However, in recent years the patient profile and expectations have gained higher relevance. This was the aim of implementing our treatment algorithm that is applied in elderly patients independent of the trauma impact if associated injuries allow (see Figure 1). The algorithm is also independent of age, age is only implicitly taken into account with its potential impact on the patient profile.
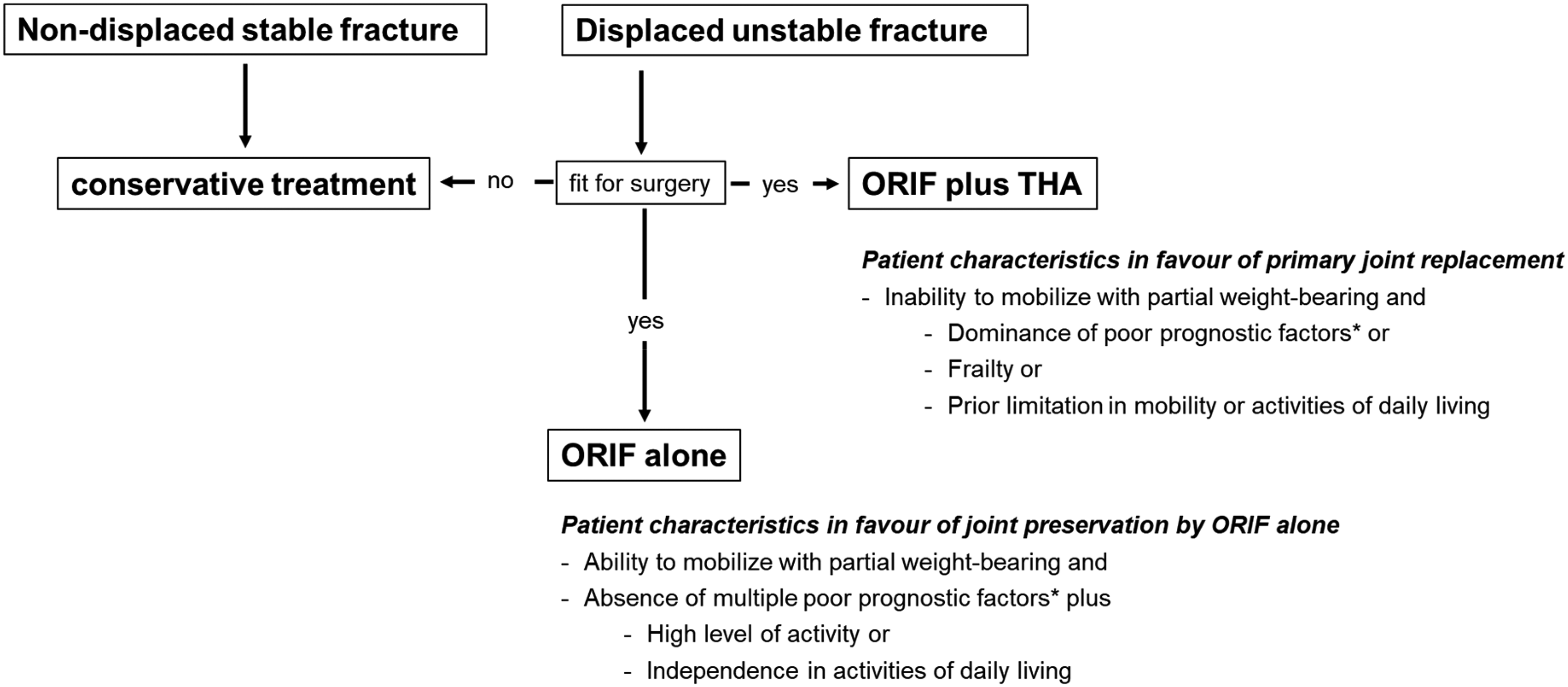
Institutional treatment algorithm for acetabular fractures in elderly patients. The algorithm depicts the different treatment approaches depending on patient characteristics and stability judged based on the criteria described by Tornetta et al. 12 *Negative prognostic factors according to Tannast et al. 7 : age over 40 years (HR 2.4), femoral head damage (HR 2.6), acetabular impaction (HR 1.5), involvement of the posterior wall (HR 1.6), anterior dislocation (5.9), or an initial displacement > 20 mm (HR 1.6).
This article describes the outcomes after the implementation of the algorithm in 2009 13 stratified by certain groups. In particular, we aim to evaluate if, after adjustment for differences in patient characteristics, patients after ORIF + THA have similar or better outcomes than patients after ORIF alone, justifying the additional operative impact.
Methods
Patient population
Patients were identified from the clinical information system including all patients ≥50 years of age treated for an acetabular fracture at our institution between January 2009 and August 2019. The study includes patients ≥50 years of age to increase the homogeneity of the patient group and the range of treatment approaches, given that patients were included after low energy (LE) and high energy (HE) trauma. Patients with periprosthetic acetabular fractures or fractures of the superior pubic ramus with extension into the acetabulum were excluded. Demographic data, comorbidity scores, measures of mobility, and living situation (Supplemental Text 1) were extracted for all patients independent of treatment. Based on the anamnestic information, the traumatic impact was categorized as “low-energy” (fall from standing or sitting height) or “high-energy” (motor vehicle accident, fall on stairs, etc.) trauma. All fractures were assessed using the classification by Judet et al. 14 The type of treatment and duration of surgery were extracted from the records. Data on the place of residence upon admission and follow-up, for example, relocation to a nursing home as well as the date of death, were collected from the Basel–Stadt registration office for patients living in that vicinity. For the remaining patients, the information was assessed as documented in the hospital records.
Primary and secondary outcomes
Loss of independence measured via relocation to a nursing home was evaluated as primary outcome since mobility is one important factor for independent living in older age.15,16 As secondary outcomes, major complications (following ICH GCP criteria for severe adverse events), intensive care unit (ICU) treatment, based on the administrative switch from orthopedics and traumatology to anesthesiology and intensive care medicine, and length of hospital stay (LOS) > 14 days were assessed. In addition, mortality, the rate of re-hospitalization, and re-operation was analyzed. As long-term outcomes, the new use of walking aids, pain at rest, and during mobilization were evaluated from outpatient records at the follow-up visit closest to 12 months.
Analytic strategy
For the surgically treated patients, outcomes were compared between ORIF alone versus ORIF + THA focusing not only on differences in specific variables, but also patterns of differences between the groups. Similar comparisons were performed between the surgically and conservatively treated patients and between patients with a low and a HE trauma.
Statistical analysis
The analysis of the primary outcome “loss of independence” is based on a competing risk approach regarding death at home as a competing risk. The distribution is described by the cumulative incidence function. Differences between patient groups were assessed by the hazard ratio (HR) from a Cox model considering death at home and loss to follow-up as censoring events. The distribution of mortality is described by Kaplan–Meier curves. Differences between patient groups were assessed by the HR from a Cox model. For binary variables, we present absolute and relative frequencies. Differences between patient groups were assessed by the odds ratio (OR) from a logistic regression model using exact logistic regression as an inference method. The distribution of continuous variables is described by mean values and the 10th and 90th percentiles.
As frailty is the major determinant for the choice of the type of surgical treatment, patient groups differ substantially. This implies a different prognosis and invalidates a direct comparison. Consequently, in this article, the conclusions are solely based on adjusted analyses taking into account the differences in patient characteristics. Due to the limited sample size, we adjusted the comparison only for age and gender. The latter was included due to a clear association of gender with the choice of surgical treatment. The same strategy was used for outcome comparisons among other patient groups.
With respect to the choice between treatment options, we considered a prespecified list of binary and continuous patient characteristics described in Supplemental Text 1. The degree of association with the treatment choice is depicted by OR from a logistic regression model.
Results
Patient population
Overall, 207 patients with acetabular fractures were included. A predominance of males was observed after both high- and low-energy trauma. The remaining patient characteristics were distributed as expected, with higher age, a higher frequency of comorbidities and dependence in the group of patients after low-energy trauma (Table 1, Supplemental Text 2, and Supplemental Table 1).
Patient characteristics at baseline.
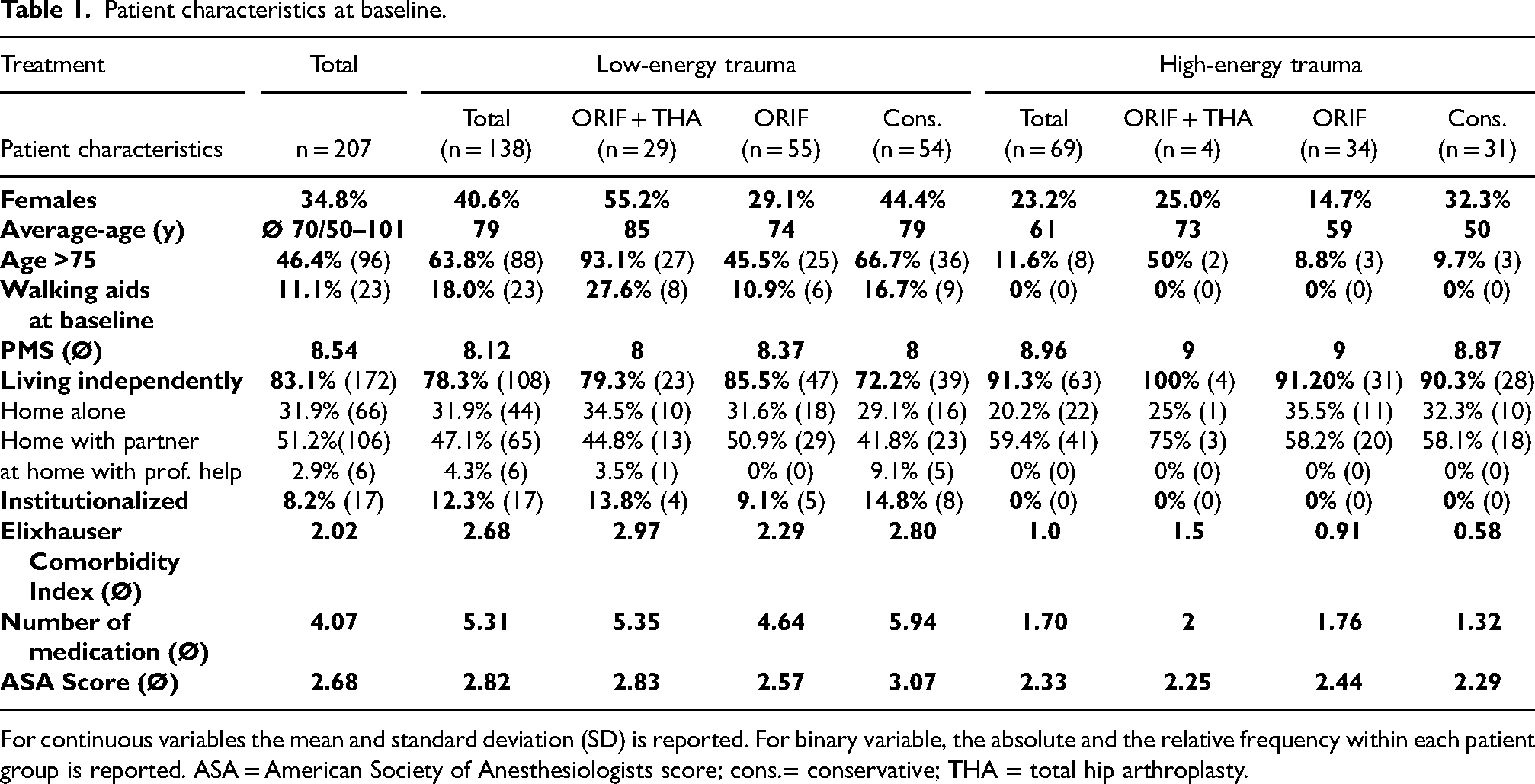
For continuous variables the mean and standard deviation (SD) is reported. For binary variable, the absolute and the relative frequency within each patient group is reported. ASA = American Society of Anesthesiologists score; cons.= conservative; THA = total hip arthroplasty.
Distribution of conservative and surgical treatment
A total of 85 patients were treated conservatively and 122 treated surgically. The distribution of patient characteristics was similar in the two groups (Supplemental Text 3 and Supplemental Table 3). The majority of patients with simple fracture patterns were treated conservatively. In no patient, the indication for conservative treatment was based on their status of health or surgical risk.
Selection of treatment in surgically treated patients
Patients treated surgically were predominantly male with an average age of 76.3 years. Among the 122 surgically treated patients, 33 received ORIF + THA. Age, female gender, and the presence of certain risk factors were associated with the decision for ORIF + THA as treatment choice (Table 2). In the age group between 50 and 65, only 4 patients were treated with ORIF + THA (Supplemental Table 1).
Association between predefined patient characteristics and the choice between ORIF and ORIF + THA.
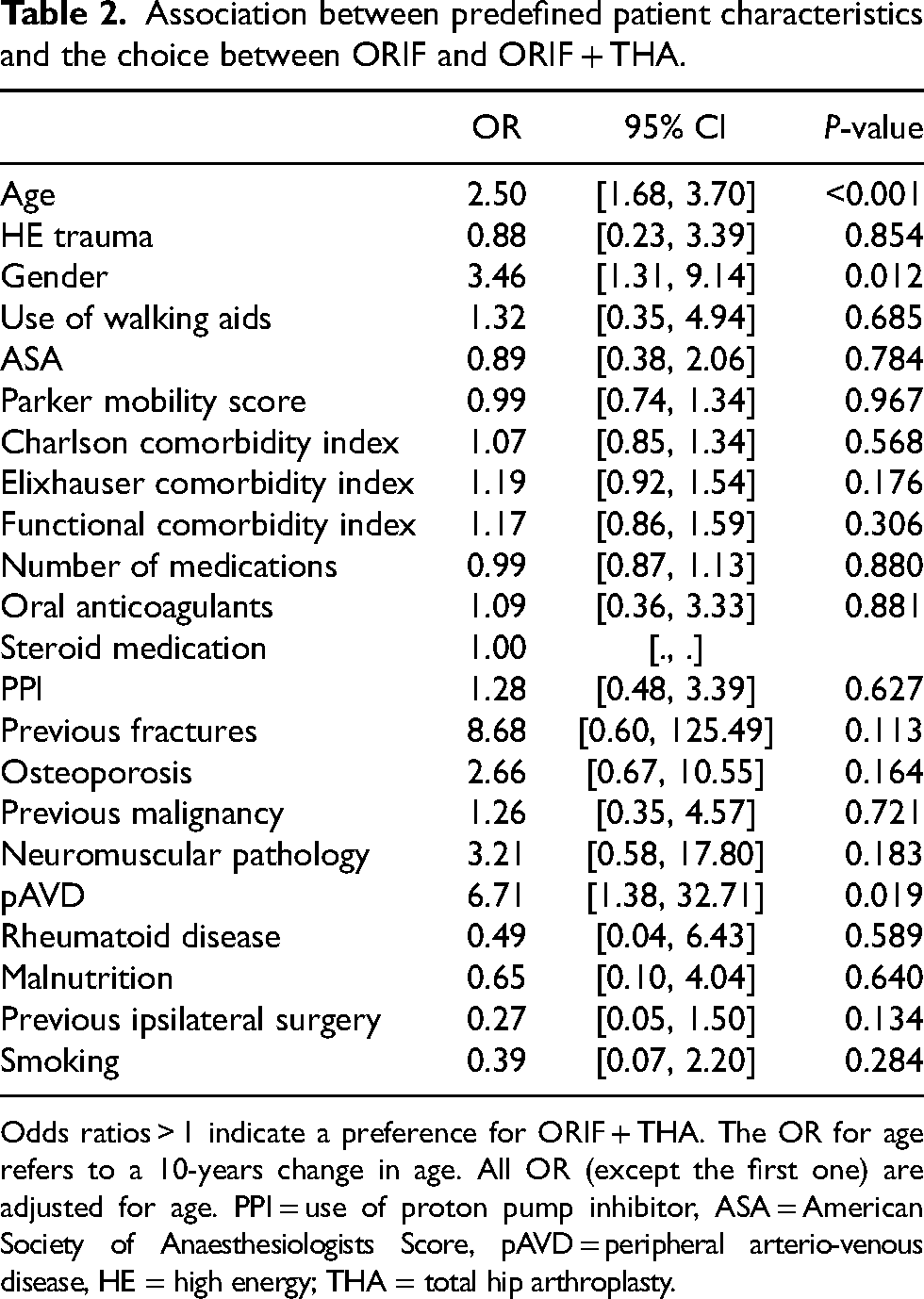
Odds ratios > 1 indicate a preference for ORIF + THA. The OR for age refers to a 10-years change in age. All OR (except the first one) are adjusted for age. PPI = use of proton pump inhibitor, ASA = American Society of Anaesthesiologists Score, pAVD = peripheral arterio-venous disease, HE = high energy; THA = total hip arthroplasty.
Women were on average older with more comorbidities (Supplemental Tables 4 and 5). The association between gender and ORIF + THA could not be explained by a joint association with age or other risk factors (data not shown).
A distinct association between specific fracture patterns and the decision for ORIF + THA could not be observed (Supplemental Table 2). Among patients with simple fracture patterns, 18% were treated with ORIF + THA, and among those with associated fracture patterns, this rate was 36% (P = 0.08).
The duration of surgery was comparable for ORIF + THA after LE and HE trauma. ORIF alone was substantially less time consuming after LE trauma, but similar in duration to ORIF + THA after HE as expected due to the complexity of fracture morphology. Accordingly, time to surgery was longest for ORIF alone after HE trauma. After LE trauma, the Stoppa approach to the anterior pelvic ring was used and a 3.5 mm “reconstruction plate” (Synthes) or a 3.5 mm “suprapectinal plate” (Stryker) was used for the osteosynthesis. In patients receiving concomitant THA combined with an anterior minimally invasive approach using an extension table for the operation. The same strategy was typically used for ORIF + THA after HE trauma. For ORIF alone after HE trauma depending on fracture morphology, the ilio-inguinal, the Stoppa, or the Kocher–Langenbeck approach were used.
Outcome comparisons in surgically treated patients
The 101 patients (82.8%) with at least one documented orthopedic follow-up had a median time until follow-up of 355 days (P10% 79 days, P90% 524 days, P = percentiles). Survival information was available for 117 patients with a median follow-up time of 509 days. Information about the participation in the scheduled follow-up visits is provided in Supplemental Figure 1.
After adjustment for age and gender, there was no statistically significant difference between loss of independence in the ORIF + THA group and ORIF group (Figure 2 and Supplemental Table 6). The secondary outcomes were also without a significant difference between the ORIF + THA and the ORIF group. There was a trend towards a higher initial morbidity after ORIF + THA with a higher rate of complications, a higher rate of ICU treatment and a longer LOS (Figures 2 and 3). In addition, there was a trend toward a better longtime outcome after ORIF + THA with less pain and a lower rate of new use of walking aids. A comparative illustration between adjusted and nonadjusted differences in outcome is shown in Supplemental Figure 2A–C. The impact of age becomes clearly visible in Supplemental Figure 2C where HR and OR are visualized to compare ORIF + THA and ORIF alone without and with age adjustment.
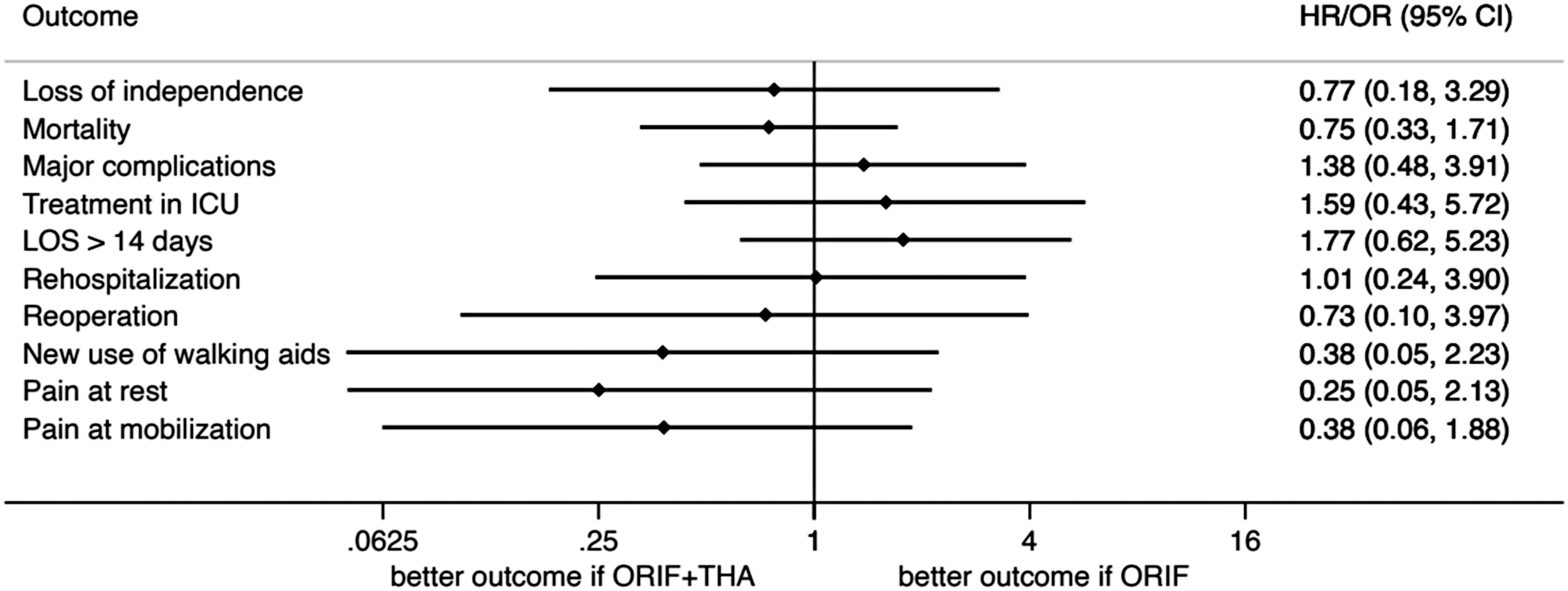
Adjusted HR and OR comparing the two surgical treatments. Adjustment has been performed for age and gender.
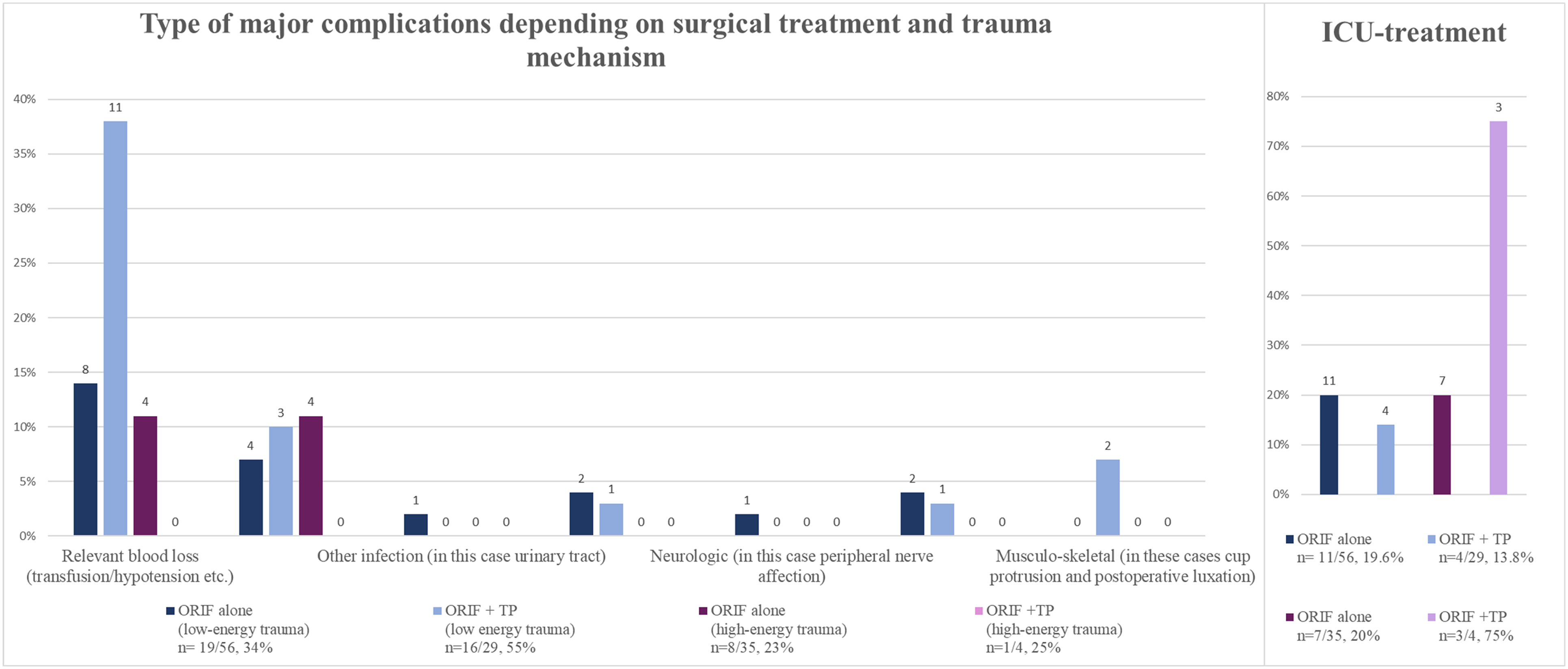
Frequency of major complications and ICU treatment. Frequency of major complications and ICU treatment, numbers on top of the bars indicate the quantity of affected patients.
Further outcome comparisons
There was no statistically significant difference between conservatively and surgically treated patients or between patients with low versus HE fractures with respect to loss of independence, mortality, complications or mobility (Supplemental Texts 4 and 5 and Supplemental Figures 3 and 4). One patient under conservative treatment suffered a cecal volvulus that was successfully operated on without sequelae.
Discussion
In the present study, patients’ performance status, activity level, and signs of frailty were used as support for the decision to employ either ORIF alone or ORIF + THA for the treatment of acetabular fractures in the elderly (Figure 1). Biological age is not specifically taken into account, since it has shown to be only roughly associated with changes related to ageing. 17 The allocation of treatment therefore mainly relies on the fractured stability (as determinant for conservative or surgical treatment) and patient profile. This becomes obvious when looking into the patient profiles of the three patients younger than 70 treated with ORIF + THA as described above. The higher stability of conservatively treated fractures may also explain the overall better outcomes in this patient group.
With this approach, we observed a trend toward a reduced loss of independence in patients treated with ORIF + THA at the cost of more in-hospital complications. Although the results were not statistically significant, all long-term outcomes (loss of independence, mortality, reoperation, new use of walking aids, pain at rest, pain at mobilization) pointed toward better long-time outcome after ORIF + THA after adjustment for age. All parameters concerning in-hospital complications (LOS, need for ICU treatment, and major complications) pointed in the direction of more short-term complications with ORIF + THA (Table 2). The observed higher rate in blood transfusions after ORIF + THA may be attributable to the additional surgical trauma. The arthroplasty-related complications are in the range of those observed after THA for femoral neck fractures. 18 The above evaluations show trends, further studies are requiring to gain more insights into the potential benefit of ORIF + THA versus ORIF in patients with acetabular fractures requiring surgery. The observed trends are in line with the clinical reasoning that in frail patients it may be worth accepting the additional surgical trauma and duration of surgery to allow early full weight bearing mobilization after ORIF + THA. Whether the observed potential long-term advantages outweigh the early risk should be discussed with patients individually in line with the concept of individualized treatment approaches and shared decision making.19,20 Overall, the algorithm though can guide an individualized treatment allocation with good long-term outcomes in both groups.
The endpoint “loss of independence” in this analysis needs to be interpreted in the context of a Swiss urban setting. In Europe, there is a trend toward single person households and most of our patients were indeed living alone or with a partner at home (Supplemental Table 6). At follow up fewer patients were living at home and overall, there is a shift toward increasing levels of support. The observed “loss of independence” may in other settings only be temporary or not perceived as “loss of independence” with alternative living arrangements such as multigenerational living or senior housing complexes with flexible support services. 21
In a randomized trial comparing ORIF with ORIF + THA in 47 patients with acetabular fractures in the elderly, the authors described lower re-operation rates in the ORIF + THA group but otherwise also comparable results. 22 Previous algorithms have focused on aspects such as the stability criteria, 12 patient factors, 14 or negative prognostic criteria. 7 A more expectation centered approach as described in our algorithm though seems similarly valid.
Recently, a register-based study comparing 1139 patients with acetabular fractures treated with ORIF + THA (also including patients treated with THA without additional ORIF) with 1139 propensity score matched patients with acetabular fractures treated with ORIF reported distinctly higher readmission rates in ORIF + THA patients, but lower rates of in-hospital complications when compared to ORIF alone. 23 The ORIF + THA group was older, had higher comorbidity scores and were more often treated in nonteaching hospitals than the ORIF group, which could explain the contrast to our results.
Similarly however to our analysis, Upfill-Brown et al. describe an association between female gender and treatment with THA. 23 It remains unclear why the gender of the individual, independent of age, has influenced treatment decisions in either cohort, especially given that sarcopenia, as a predictive factor, is typically more prevalent in men than women, after the age of 80 years.24–26 Accordingly, a higher frequency of ORIF + THA in the male population compared to the female one could be expected in higher age groups. Female gender has been associated with higher health care utilization,27,28 not necessarily correlating with age or comorbidities. 29 In view of these results, one reason for the observed gender-specific difference in treatment allocation could be a more detailed health status documentation in women. Previous research has also shown that independent of health profiles, the prescription of activity restrictions based on illness behavior was more frequent for female patients. 30 The authors explain this phenomenon by a socialization-based more intense illness behavior in women and potential gender bias from health care providers. Both may have played a relevant role in the above study. Another aspect may be gender disparities in physical activities with potentially the perception of lower expectations in females. 31
There are several limitations to this study. Its retrospective design made it necessary to rely on routine documentation that is not standardized. Especially in this very old population, loss to follow-up due to death, dementia, and preferred follow-up by primary health care providers due to concurring comorbidities was inevitable. The nonrandom treatment allocation made it necessary to adjust for differences in patient characteristics between treatment groups, and the limited number of patients limited the number of adjustable factors. In addition, the aim was to demonstrate the absence of differences between treatment groups, which requires large sample sizes to draw strict conclusions.
Conclusion
The results of this study underline the importance of individualized treatment for acetabular fractures in elderly individuals, suggesting a long-term advantage after ORIF + THA compared to ORIF alone for frail patients. However, this advantage comes at the price of more postoperative complications. In addition, the results point to potential gender bias, that should actively be addressed in clinical practice and research.
Supplemental Material
sj-docx-1-otr-10.1177_22104917241256656 - Supplemental material for Comparative outcome of different treatment options for acetabulum fractures in elderly individuals—a retrospective analysis of 207 patients
Supplemental material, sj-docx-1-otr-10.1177_22104917241256656 for Comparative outcome of different treatment options for acetabulum fractures in elderly individuals—a retrospective analysis of 207 patients by Sebastian Husi, Werner Vach, Dieter Cadosch, Marcel Jakob, Franziska Saxer and Henrik Eckardt in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Author contribution
Sebastian Husi contributed to validation, investigation; Dieter Cadosch contributed to investigation; Werner Vach contributed to methodology, formal analysis, data curation; Marcel Jakob contributed to investigation; Franziska Saxer contributed to conceptualization, methodology, validation, writing-original draft, writing-review editing; Henrik Eckardt contributed to conceptualization, methodology, validation, writing-original draft, writing-review editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the competent ethics committee (Ethikkommission Nordwest und Zentralschweiz, EKNZ, Reference No. 2019-00520). In accordance with Art. 34 of the Swiss Human Research Ordinance all patients were included without individual consent unless a general dissent for the further use of routine health-data had been documented. The study followed good clinical practice (GCP) as well as the tenets of the Declaration of Helsinki and was registered with ClinicalTrials.gov, identifier: NCT03929536. Need for individual consent was waived provided that no dissent had been documented according to applicable Swiss Law Ethics approval and consent to participate.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.