
Abstract
Introduction:
The total hip arthroplasty (THA) as part of acute fracture management is used for acetabular fractures in elderly patients. Our objective was to assess the stability of osteosynthesis performed using 2 different techniques in combination with THA in an experimental model.
Materials and Methods:
We conducted 20 experiments using the left-side hemipelves composite bone models. There were 2 testing groups: 1- and 2-stage osteosynthesis. The acetabular fractures of the anterior column and posterior hemitransverse were simulated. The same THA technique was used in both groups. The stability of osteosynthesis was explored and compared between the groups by measuring the fracture displacement of anterior and posterior columns under the standardized test load (1187 N) protocol. Load distance diagrams were generated.
Results:
The 0.680-mm gap (0.518; 1.548) of the posterior column in the 1-stage group (n = 10) was higher than the 0.370-mm gap (0.255; 0.428) in the 2-stage group (n = 10; P = .002). There was no significant difference between the gap of the anterior column in the 1- and 2-stage groups (0.135 [0.078; 0.290] mm vs 0.160 [0.120; 0.210] mm; P = .579).
Conclusion:
The 2-stage osteosynthesis of the anterior and posterior columns in combination with THA provides better stability of posterior column when compared to 1-stage method in composite bone models.
Keywords
Introduction
Acetabular fractures in the elderly individuals are increasing in prevalence. 1,2 The increasing prevalence of osteoporosis in the aging population has contributed to older patients becoming the fastest-growing group presenting with acetabular fractures. 3
Simple mechanical fall from standing height in elderly patients with preexisting osteoporosis is the most common cause of acetabular fracture. Treatment options for acetabular fractures in elderly individuals include conservative methods, percutaneous fixation, open reduction and internal fixation (ORIF), and acute or secondary total hip arthroplasty (THA). Conservative treatment for displaced acetabular fractures in elderly patients is related to the high risk of complications due to the prolonged decubitus position. The ORIF is also not the best option because of osteoporotic bone and lengthy decubitus position. 4 Moreover, although ORIF requires 1 surgery, a secondary THA may be needed in the future because of osteoarthritis. 5
The secondary THA following ORIF is a demanding technique. Due to adhesions and a frequent malposition of the acetabulum, the secondary THA is associated with an increased risk of infection, tendency to develop para-articular ossifications, and a higher risk of early component loosening compared to the acute THA. 6 If there is significant impaction, destruction of articular cartilage, and well-done ORIF is in doubt, acetabular stabilization and primary THA at 1 stage should be considered. 7 Acute primary THA with the use of an antiprotrusion cage and bone grafting for acetabular fractures allows to employ 1 operation for definitive repair. 6,8 It provides primary stability and immediate pain relief, permits graded weight-bearing and early pain-free mobilization, and may also treat hip arthritis, if it exists. 6 Complications, surgical times, and hospitalizations are consistent with ORIF or secondary THA, but a single surgical procedure will avoid the “wait-and-see” approach, which is often used for these patients. 8
Biomechanical studies are conventionally used to evaluate the stability of fixation of acetabular fractures achieved using different techniques. 9,10 However, at the time of designing the present study, we did not find biomechanical study reports on the use of ORIF in combination with THA for the treatment of acetabular fractures.
Our objective was to compare the stability of osteosynthesis for anterior column–posterior hemitransverse acetabular fractures performed using 1- and 2-stage osteosynthesis techniques combined with THA. Our null hypothesis was that there is no difference between the biomechanical performance of these fixation techniques.
Materials and Methods
The study was conducted in 2 groups of experiments, the 1- and 2-stage osteosynthesis technique groups, respectively. The number of stages reflects the number of approaches to the fractures. The 1-stage group implied osteosynthesis using the posterior approach. The 2-stage group implied anterior approach for anterior column osteosynthesis followed by the posterior approach for posterior column osteosynthesis. 11
Specimens
We used 20 synthetic, fourth generation, left-side composite hemipelvises (Saw Bones;, Hemi Pelvis, Fourth Generation; Sawbones Europe AB, Sweden). Ten orthopedic composite bone models were used in each group. Artificial fracture 62B3 with a protrusion of a quadrilateral plate (Letournel classification for acetabular fractures) 12 was performed by making osteotomy along the premarked fracture lines (Figure 1).

The premarked fracture lines for simulation of 62B3 fracture with protrusion of a quadrilateral plate.
Osteosynthesis Techniques
In the 1-stage group, the posterior column was stabilized with a 3.5-mm reconstruction plate (Figure 2). The stabilization of the anterior and posterior columns was achieved using 1 intra-acetabular reconstruction bent plate that was fixed with screws. Once the columns were stabilized, a cemented-type polyethylene acetabular cup was implanted with an aim to simulate THA (Figure 2).
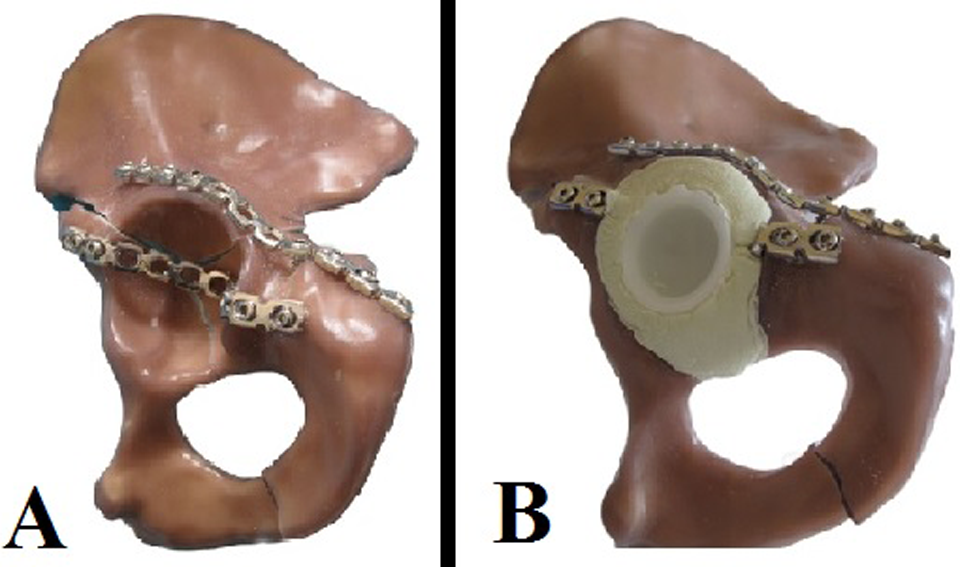
A, One-stage osteosynthesis before total hip arthroplasty (THA). B, One-stage osteosynthesis after the cemented cup implantation.
In the 2-stage group, through anterior approach, the anterior column stabilization with a reconstruction plate was performed (Figure 3). Then, through the posterior approach, the standard internal posterior column osteosynthesis followed by implantation of the cemented acetabular cup was performed using the same technique as it was in 1-stage protocol.

Two-stage osteosynthesis group before the cemented cup implantation. A, Lateral view. B, Anterior view.
In both groups, a standard 3.5-mm pelvic reconstruction plate (11-hole) and 3.5-mm cortical screws were used for osteosyntheses. The same parameter screws put in the same location holes were used in all osteosyntheses. We used the 11- × 135-mm femoral stem, 32-mm-diameter femoral head, 44-mm acetabular polyethylene cup, and 40 g of bone cement for performing the THA.
Biomechanical Testing
The pelvis was positioned at the level of the anterior iliac spine, whereas the pubic bone was located orthogonally in the background. Then the presacral iliac part was attached to the coordinate rotation table imitating rotational accuracy of 5°. This setup simulated a physiological pelvis anteversion of 50° to 60°. The simulation of normal human gait was based on the anatomical studies that found 45° abduction and 15° anteversion of the normal femoral head (Figure 4). 13 After adjustment of the hemipelvises, the calibration of the coordinate system was performed.

Biomechanical workbench. Normal femoral head 45° abduction and 15° anteversion.
Four mechanical distance indicators were used for the measurement of fracture displacement. Two indicators measured the anterior column fracture gap. The other 2 indicators measured the posterior hemitransverse fracture gap. With the measuring accuracy of 0.01 mm, the indicators were pretensed up to 4 mm in order to have a free measurement capacity. The frame of the measuring device was attached with stiffness of more than 500 N/mm to ensure stability of the basis. The reference points were situated in the inner quadrilateral plate. The protrusion was measured as medial dislocation of the marked fragment. This gap was used as baseline. The test load procedures in both protocols included 3 preload tests (15 N) for the pretension of structures and 1 ultimate load test (1187 N). The measurements were done exactly at the fracture site, so the apparent motions of the hemipelvises and the testing setup have not affected the results. The fracture gaps were recorded when the maximum load of 1187 N was applied. Load distance diagrams were generated using the raw data (ASCII format).
Data are presented as median, 25th and 75th percentiles, and a Wilcoxon signed rank test was applied for nonnormally distributed data. The Mann-Whitney U test was used to assess the differences between groups. A statistical analysis was performed using PASW (PASW Statistics 17, SPSS 20.0; IBM Corporation, New York). The significance level was set to α = .05 (2 sided).
Results
The 0.680-mm gap (0.518; 1.548) of the posterior column in the 1-stage group (n = 10) was higher when compared to the 0.370-mm gap (0.255; 0.428) in the 2-stage group (n = 10; P = .002; Figure 5). There was no difference between the gap of the anterior column in the 1- and 2-stage groups (0.135 [0.078; 0.290] mm vs 0.160 [0.120; 0.210] mm; P = .579; Figure 6).

Posterior column fracture gap after loading.
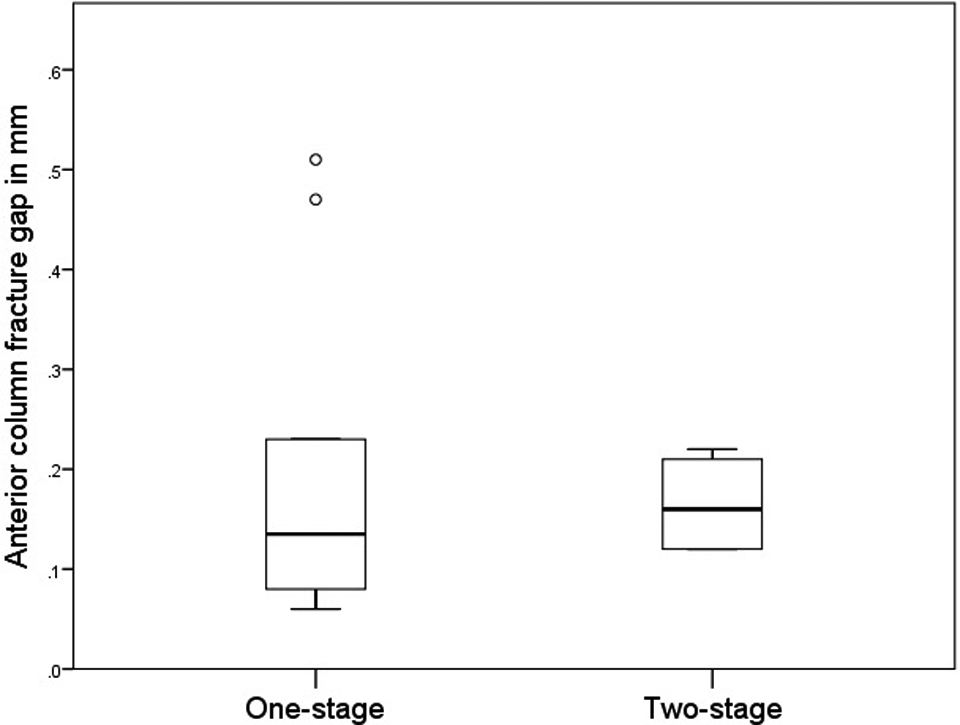
Anterior column fracture gap after loading.
Discussion
The most important finding of the present study was that 2-stage technique provided better stability for anterior column in 62B3 fracture osteosynthesis than the 1-stage technique. Although statistically significant difference was observed, there was only 0.310 mm difference between the posterior column means in the 2 groups, which is in doubt to reflect clinical importance. However, the experiment was conducted using synthetic bones, which represents healthy nonosteoporotic bone. It is possible that there would be a bigger difference in poor quality bone.
Acetabular fractures as a result of low-energy mechanisms (osteporosis-related) in elderly patients can be well treated by nonoperative management, ORIF, or acute THA. However, few data exist regarding the treatment outcomes for geriatric acetabular fractures. It is difficult for clinicians to decide among ORIF, percutaneous fixation, acute THA, and nonoperative strategies of treatment.
The ORIF shows a high 1-year mortality rate of 25% and a 28% rate of conversion to THA after ORIF. 14 It has been reported that bony union of acetabular fracture after ORIF was achieved in 74% of patients younger than 60 years, but in only 44% of patients older than 60 years. 6 A recent systematic review involving a number of databases to identify studies that included outcomes in patients aged >55 years has indicated that the overall mean rate of conversion to THA was 23.1%, rate of nonfatal complications was 39.8%, and the mean mortality rate was 19.1% at a mean of 64 months. 3 In the present study, anterior fixation of the pelvic rim and posterior stabilization of standard posterior column fixation ensured good stability of both columns and provided good conditions for the cemented cup implantation.
In vivo measurements of hip joint stress were previously performed using the instrumented hip endoprostheses in different loading conditions. Our choice of 1187 N maximum loading is relevant to elderly patients after THA who use crutches in order to reduce the lower limb loading. Damm et al 15 found that loading on the operated hip approximated 160% to 180% body weight during a 4-point gait when walking with forearm crutches in early postoperative period. The choice of 1187 N maximum loading in the present study is in accordance with these findings. Our calculation was based on the assumption that the body weight is 70 kg.
Nie et al found that stress in acetabular dome is concentrated in the acetabular rime, the superior part of the lunate surface, and the posterior–superior surface of acetabulum in normal hip joint, while the highest stress is in the posterior hemitransverse fracture area. 16 These findings explain why we have observed a significantly lower displacement of the posterior column fracture gap in the 2-stage protocol compared to the 1-stage. In the 2-stage protocol, the acetabular dome was secured by 2 plates above the dome, and the anterior column fixation has possibly neutralized stress in the posterior hemitransverse fracture zone. Meanwhile, in the 1-stage protocol, the anterior column fixation was under the acetabular dome, and thus bearing in mind the cranial direction of the loading, it did not provide sufficient support to the posterior column fixation.
This study has some limitations. First, it has a small sample size and our findings are inconclusive. Next, in one of the 1-stage protocol tests, we found higher displacement than in other tests of this group. The calculated Z values suggested that it is a relative exception. Since we found significant difference between the 2 study groups when data from this particular test were excluded from the analysis, it suggests that this relative exception did not have an impact on the conclusion. Finally, we used our research group’s designed and custom-made testing rig and we did not find similar study to validate it. Since we did not find biomechanical study reports on the use of ORIF with THA, we could not compare our results with the findings of other researchers.
The recently published 5-year follow-up of functional outcomes in the oldest independent old and very old patients (>80 years old) with previously good functional status has demonstrated that with appropriate surgical and geriatric care, they have few hip dislocations and reoperations, survive postfracture at least as long as their noninjured contemporaries, and continue to function and ambulate as they did prior to their injury. 17 It is noteworthy that when the fracture fixation is followed by acute THA, the perfect reduction of fracture is not required. The resected femoral head may be used for the autograft of bone defects. These advantages are important for the better outcomes of treatment. We believe that our findings will encourage future research in this field.
Conclusion
The 2-stage osteosynthesis of anterior and posterior columns in combination with THA provided better stability of posterior column when compared to 1-stage osteosynthesis in the experimental model. Our findings are inconclusive and require investigation in future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.