
Abstract
Introduction
A systematic analysis from the Global Burden of Disease Study 2019 that reported the global, regional, and national burden of bone fractures in 204 countries and territories, from 1990 to 2019, stated that fractures in older adults constitute the majority of fractures. 1 Fragility fractures of the pelvis (FFP) occur primarily in older individuals, and the frequency of these injuries is increasing correspondingly with the aging population and improved diagnostic modalities. 2 FFP exhibits different morphological characteristics and occurs as a result of different mechanisms other than high-energy pelvic ring lesions; however, the degree of instability may increase over time. 3 Fragility fractures with no displacement within the posterior part of the pelvic ring are treated conservatively with pain therapy and mobilization as tolerated. 3 Several studies reported that the clinical results of conservative treatment with accurate patient selection were acceptable.3–5 On the contrary, some studies revealed that the outcomes of conservative therapy were poor, with loss of social and physical independence and autonomy, and increased mortality rate.6,7
Rommens and Hofmann developed a novel classification system focusing on FFP 8 ; the classification is based on morphological criteria that correspond with the degree of instability. These criteria are critical for treatment decision-making, including the type and extent of surgery. 8 Based on this classification, many reports recommended surgical treatment for patients with type III and IV FFP.9–11 Furthermore, Yoshida et al. 5 stated that FFP was similar to proximal femoral fracture and causes a significant decrease in activities of daily living (ADLs), and surgical treatment should, therefore, be aggressively performed to regain walking ability. In a patient-based outcome study, participants who received a percutaneous screw fixation for fragility fractures of the posterior pelvic ring reported an overall positive outcome concerning their long-term well-being. 12 In particular, older patients appear to benefit from surgical treatment.
Despite various reports on treatments for FFP, the majority of patients are still treated with bed rest (conservative therapy). Although we believe that conservative treatment is an appropriate choice for patients with FFP, some patients exhibit marked deterioration in walking ability even when bone union is achieved. Nevertheless, the indications for surgical treatment remain unclear. Therefore, the present study aimed to determine the prognostic factors associated with walking ability one year after injury in patients with FFP who were treated conservatively, using multiple logistic regression analysis. Further, we aimed to clarify the limitations of conservative treatment and the indications and timing of surgical treatment.
Patients and methods
Patient demographics
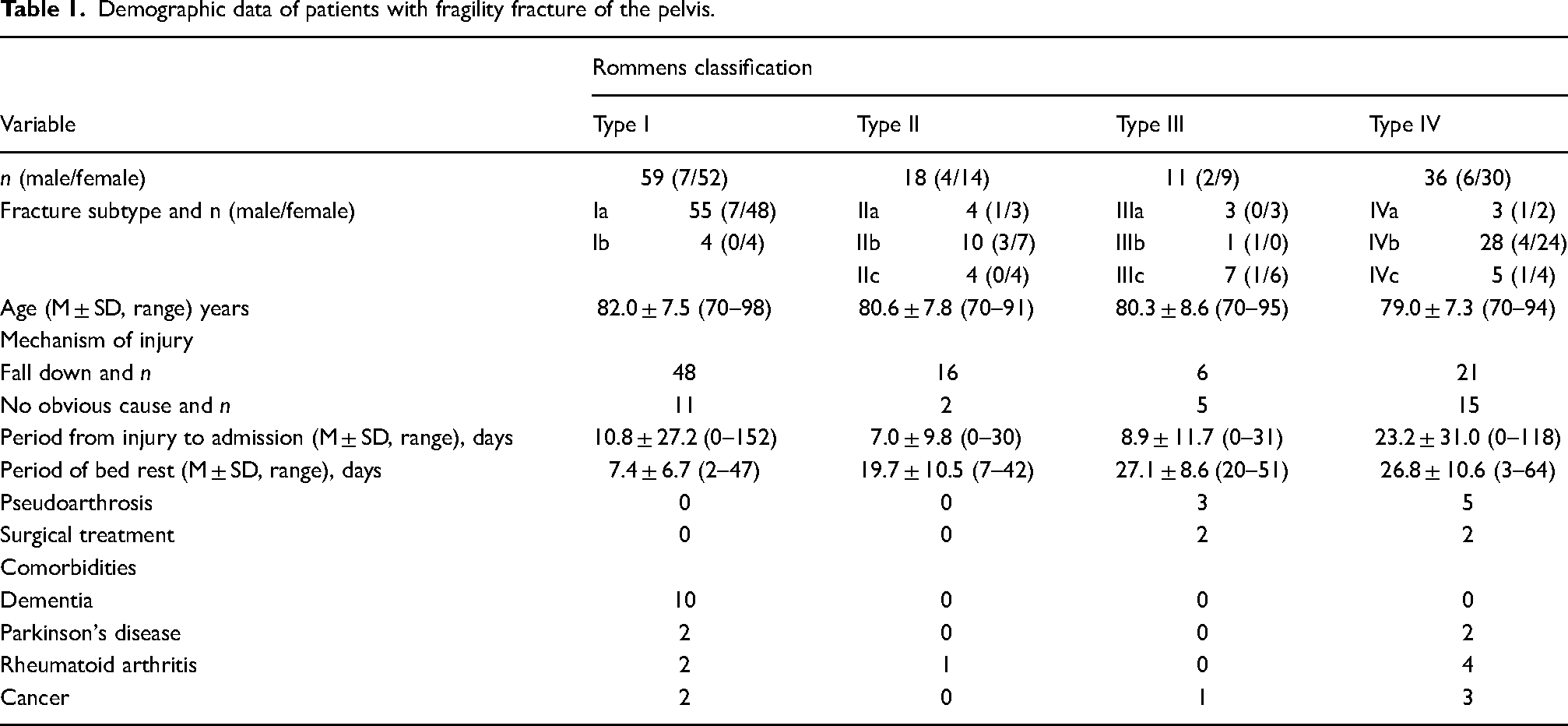
Between 2011 and 2020, 137 patients with FFP ≥ 70 years were admitted to our university hospital. The study included 22 men and 115 women with injuries (mean age, 81 years; range: 70–98 years). In this series, three (2%) patients died from causes unrelated to the fracture before the one-year follow-up visit, and 10 (7%) patients were lost to follow-up before one year. These 13 (9%) patients were excluded from the study. The remaining 124 patients (19 men and 105 women; mean age, 81 years; range, 70–98 years) were included in this study. We defined FFP as a pelvic ring fracture after low-energy trauma, such as falling from a standing height. We excluded high-energy pelvic ring injuries, acetabular fractures, and pathological fractures, such as metastatic tumors. Radiographic examinations included plain pelvic views, multiplanar plain computed tomography (CT), and/or magnetic resonance imaging (MRI) to improve diagnostic accuracy. The type of injury was assessed according to the Rommens classification system 8 ; 55 patients were classified as type Ia, four as type Ib, four as type IIa, 10 as type IIb, four as type IIc, three as type IIIa, one as type IIIb, seven as type IIIc, three as type IVa, 28 as type IVb, and five as type IVc. The cause of injury was falls in 91 patients (73%); however, the cause of injury in 33 patients (27%) was unclear. The comorbidities of the participants are summarized in Table 1.
Demographic data of patients with fragility fracture of the pelvis.
Treatment strategy
All patients were treated conservatively with bed rest and analgesics, such as acetaminophen and/or nonsteroidal antiinflammatory drugs, for pain relief. Only eight (6%) patients were treated with teriparatide (a recombinant human parathyroid hormone). Once pain relief was achieved, sitting and standing were permitted. Muscle strengthening exercises of the lower extremities were performed, depending on pain intensity. In patients classified as types III and IV, ambulation was permitted 4–10 weeks after injury, and the bony union was followed up using serial radiographs. During conservative treatment, patients whose ADLs did not improve due to pain underwent surgery.
Outcome evaluation
All patients, except those who underwent surgery during conservative treatment, were evaluated for clinical outcomes one year after injury. Functional ambulation categories (FAC) 13 were used to assess gait ability and autonomy. This scale includes six levels, ranging from 0 to 5, as follows: FAC 0, unable to walk or needed two assistants to help them walk; FAC 1, able to walk with continuous support of one assistant; FAC 2, able to walk with continuous support of one person for balance; FAC 3, able to walk with one assistant beside them to give them confidence; FAC 4, able to walk independently but need help on stairs or uneven surfaces; and FAC 5, able to walk independently anywhere. A recent study suggested that this tool was feasible to describe walking ability under various circumstances, such as for fragility fractures and postacute rehabilitation, and also at follow-up. 14 Therefore, in keeping with this finding, we used this scale to measure walking ability. Patients with a decrease in FAC of two levels or more were regarded as having poor outcomes. Radiological examinations at follow-up, including plain anteroposterior radiographs of the pelvis, were performed at 1, 2, 3, 6, and 12 months after injury or admission to investigate bone union. CT and/or MRI scans were performed in patients with persistent pain and those who did not achieve bone union as observed on plain radiographs.
The protocol for investigating the clinical outcomes and radiological findings was approved by the institutional review board of the authors’ affiliated institutions, and informed consent was obtained from all participants before inclusion.
Statistical analysis
All statistical analyses were performed using the EZR software Version 4.0.2. 15 The Kruskal–Wallis test was used to compare continuous variables across the four Rommens classification categories, such as the bed rest period. Univariate comparisons were performed using the Mann–Whitney U test for continuous variables, such as age and bed rest period, and the Fisher's exact test for other categorical data. Parameters with p < .15 in univariate analyses were included in the logistic regression analysis. Continuous variables were converted into binary variables based on cut-off values. The optimal cut-off values were calculated using receiver operating characteristic (ROC) analysis as the point closest to the upper left of the graph. Logistic regression analysis was performed using these binary variables in the forward stepwise method to determine the independent predictors of a two-level decrease in FAC. p < .05 was considered statistically significant.
Results
The average bed rest period was 6.7, 18.4, 27.1, and 26.8 days for patients with types I, II, III, and IV fractures, respectively. Patients with type I fractures had a significantly shorter bed rest period than those with types II, III, and IV (p < .001), but no other between-group differences were observed. Eight of the 124 patients presented with delayed union, which continued to heal within three months of follow-up. The fracture subtypes of these eight patients were as follows: IIIa (n = 2), IIIb (n = 1), IVa (n = 3), and IVb (n = 2). Four patients (type IIIa: n = 1, IIIb: n = 1, IVa: n = 2) underwent surgery during conservative treatment, at an average of 10 weeks after their hospital visit, due to delayed union of the posterior ilium and persistent intense pain. Thereafter, these patients continued bed rest and rehabilitation and were able to achieve bone union within one year. Teriparatide was used in one of the four patients. Bone union was obtained during follow-up in all patients, excluding those with delayed union.
Walking ability was assessed in 120 patients, excluding the four patients who underwent surgery. The recovery rate of walking ability, as indicated by FAC, to the preinjury state at one year after injury was 80%, 100%, 44%, and 53% for types I, II, III, and IV, respectively. Table 2 summarizes the univariate factors associated with poor ambulatory outcomes with a two-level decrease in FAC. Fourteen (12%) patients exhibited markedly impaired walking ability with a two-level decrease in FAC at one year after admission. In the univariate analysis, five parameters (p < .15) were included in the multivariate logistic regression analysis: sex, Rommens classification, period from injury to admission, bed rest period, and presence of cancer. ROC analysis was performed to define the optimal cut-off values of continuous variables of the parameters, such as the period from injury to admission and the period of bed rest. The area under the curve for the period from injury to admission and the period of bed rest were 0.63 and 0.77, respectively. These two parameters possess the low-to-moderate diagnostic ability, and their cut-off values were as follows: the period from injury to admission, seven days; and the period of bed rest, 28 days (Figure 1). These variables were converted into binary variables based on the cut-off values obtained by the ROC analysis; continuous variables were converted into points 1 or 0 depending on whether they exceeded or were less than the cut-off values.
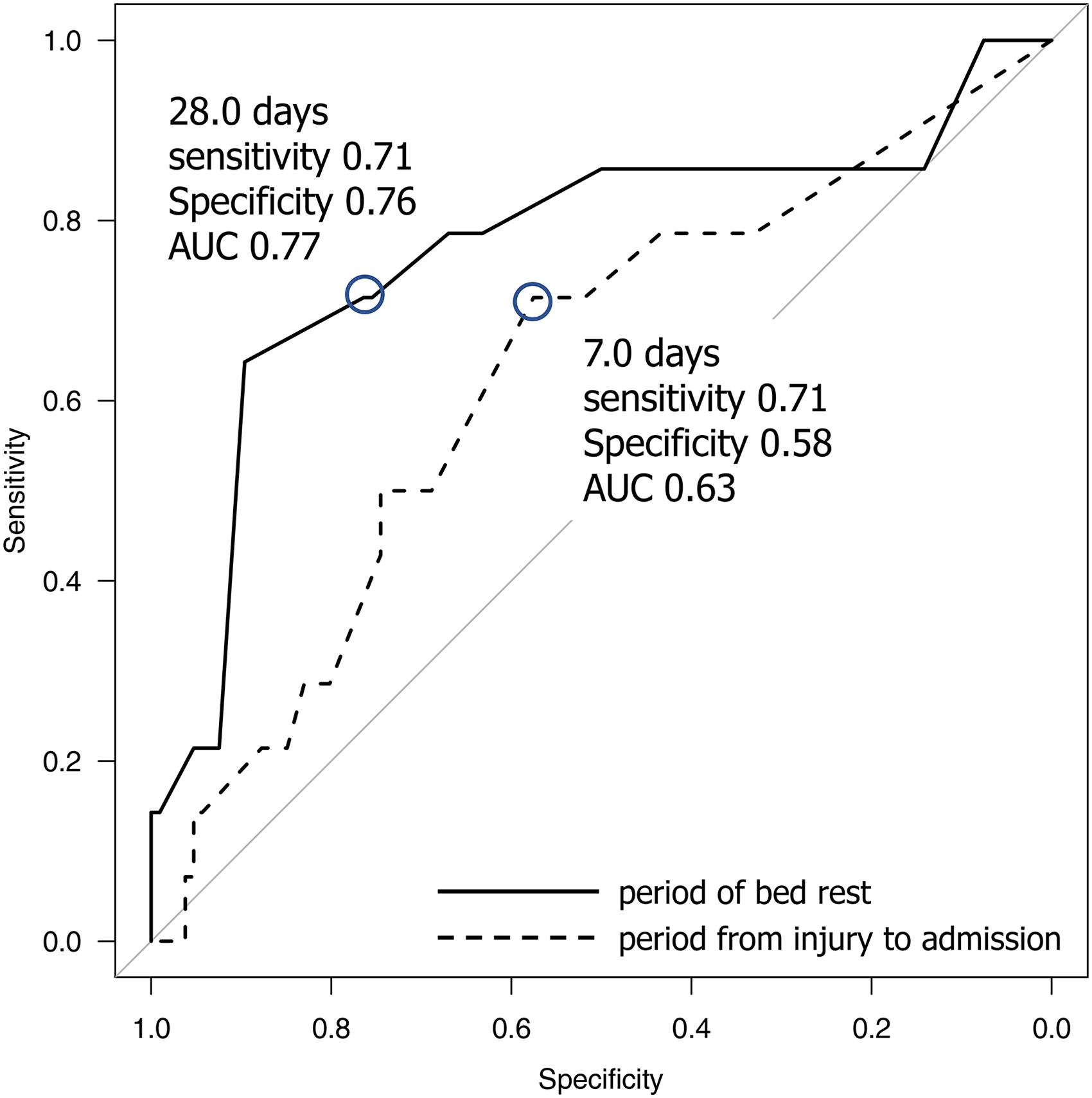
Receiver operating characteristic curves for the period from injury to admission (AUC: 0.63, cut-off value: 7.0 days) and period of bed rest (AUC: 0.77, cut-off value 28.0 days). AUC, area under the curve.
Results of the univariate analysis of 120 cases for factors associated with gait status one year after injury, excluding four surgical cases.
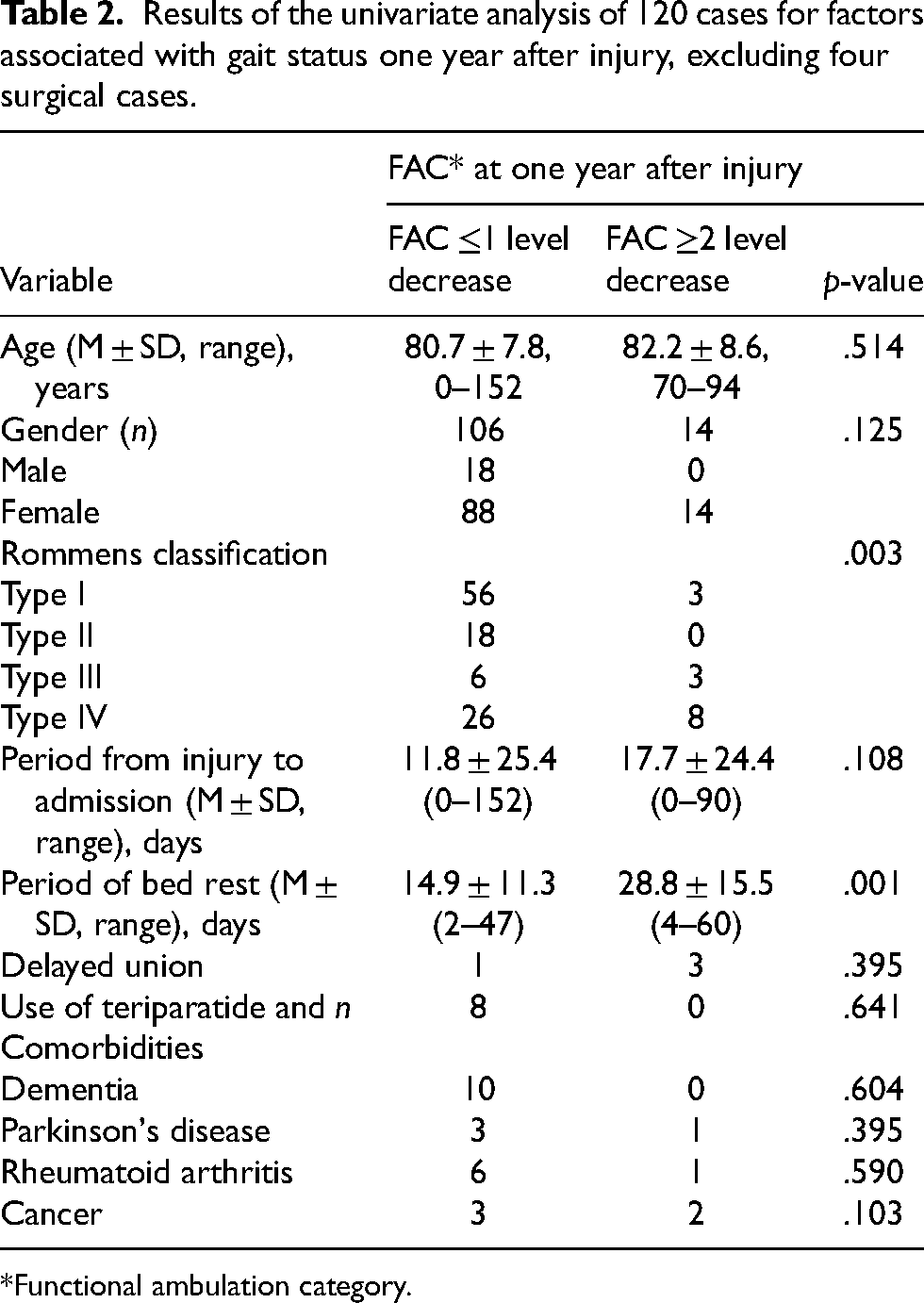
*Functional ambulation category.
Multiple logistic regression identified the following risk factors for significant deterioration of walking ability after one year: ≥ 4-week bed rest (odds ratio [OR] 10.300; 95% confidence interval 95% CI: [2.630–40.300]) and the presence of cancer (OR 11.700; 95% CI: [1.290–107.000]) (Table 3).
Results of multiple logistic regression analysis for prognostic factors associated with walking ability.
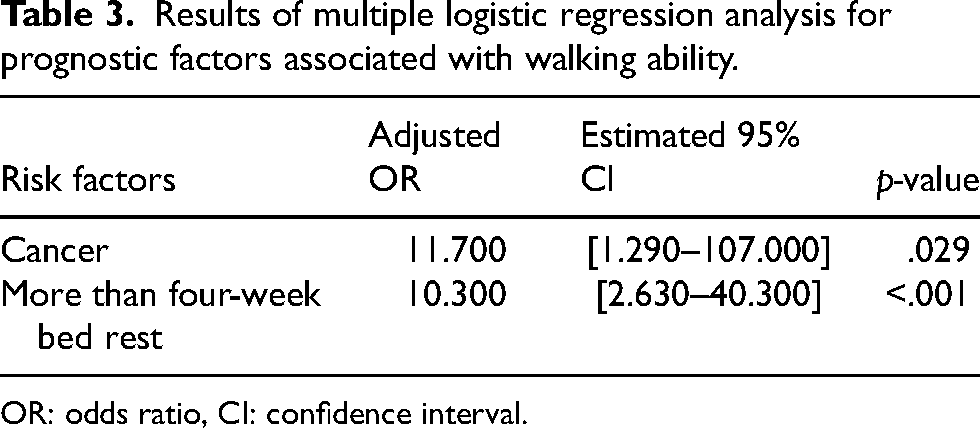
OR: odds ratio, CI: confidence interval.
Discussion
Our results revealed that the presence of cancer and more than four-week bed rest, with a two-level decrease in FAC, were risk factors for a significant decrease in walking ability.
There was a significant difference in walking ability after one year between the Rommens classification types in the univariate analysis; however, fracture type was not identified as predictive of poor ambulatory outcomes. We speculate the reason for this result was that there were few cases of long-term bed rest; other reasons were cases including cancer, among the type I or II fractures; there were few cases with minimal pain in types III or IV fractures where conservative treatment was successful. Among the various complications, cancer was the only risk factor for significant deterioration in walking ability one year after injury. In this regard, several studies reported that approximately half of older patients with cancer exhibited prefrailty or frailty and experienced difficulty or required assistance to perform basic and instrumental ADLs. These patients were at an increased risk of chemotherapy intolerance, postoperative complications, and mortality.16,17 Moreover, another study reported that higher levels of physical activity were associated with reduced risk and improved survival in several cancers, 18 or taking more steps per day was associated with a progressively lower risk for all-cause mortality, to a level that varied according to age. 19 Several studies suggested that rehabilitation of patients with cancer was crucial to improve prognosis. Neo et al. 17 emphasized the substantial need for rehabilitation services that focus on maintaining functional independence and underscored the important role of professionals skilled in occupational assessment and therapy. We agree with this approach, which should not be limited to patients with cancer, but we recommend that patients with FFP with or without cancer, require early active exercise therapy.
It is established that muscle atrophy and decline in muscle strength occur rapidly with prolonged disuse or mechanical unloading after acute hospitalization or experimental bed rest. A study that analyzed data after 5–120 days of bed rest in 318 healthy adults demonstrated that the highest rate of muscle strength decline and atrophy occurred during the earliest stages of bed rest, during the first two weeks of bed rest. 20 In addition, the study highlighted that 79% of muscle strength loss could be attributed to muscle atrophy, while the remaining was most likely due to alterations in single fiber mechanical properties, excitation–contraction coupling, fiber architecture, tendon stiffness, muscle denervation, neuromuscular junction damage, and supraspinal changes. 20 Previous studies analyzed the gait of patients with pelvic and acetabular fractures and concluded that the gait pattern suggested prolonged weakness of hip abductor muscles.21,22 Conversely, we found that early initiation of hip abductor muscle exercise after surgery led to improvement in hip abductor muscle strength. 22 Therefore, we strongly emphasize that early rehabilitation, including hip abductor muscle exercise, is crucial for patients with FFP.
Early physical therapy is important; however, some patients with FFP experience difficulty in initiating rehabilitation due to severe pain. In the present study, some patients required extended periods of bed rest due to pain, and most patients with types IIIa, IIIb, and IVa developed delayed union and eventually required surgical treatment. Ueda et al. 10 demonstrated that prolonged pain was associated with fracture progression, and the presence of prolonged pain could potentially help identify fracture progression. Several studies reported that when fracture progression was identified, surgical treatment might be required if FFP progresses to type III or IV fracture.10,23 Rommens et al. 24 recommended surgical treatment for FFP types III and IV and that surgical treatment should be considered in patients with FFP type II when the patient could not be mobilized within 1 week or when complaints worsened. Furthermore, Rommens et al. 23 suggested that the duration of complete bed rest should be shortened as much as possible because prolonged bed rest has been associated with muscle weakness and postural hypotension in older patients and is associated with a high risk of complications such as decubitus, ulcers, deep vein thrombosis, pulmonary embolism, and urinary tract infection. In the current study, more than four-week bed rest was a risk factor for a significant decrease in walking ability one year after injury. We believe that surgical treatment should be performed no later than three weeks after injury, considering the postoperative rest period. As such, patients with severe pain, with the inability to sit up or transfer to a wheelchair that continues for two to three weeks after injury, despite pain control, should be treated surgically, and rehabilitation should be initiated soon after the surgery. Although FFP usually has less ligamentous component breakdown, type IIIa or IVa FFP cannot be expected to be stabilized by ligaments; therefore, we recommend that surgical treatment should be performed early after admission.
Teriparatide (recombinant human parathyroid hormone) is a bone-forming medication that preferentially stimulates osteoblasts to produce new bone tissue, thereby increasing bone mass and strength. Several studies revealed that teriparatide prevented secondary vertebral and/or nonvertebral fractures and contributed to pain relief over the long term.25,26 Peichl et al. 27 reported data from a randomized controlled trial (RCT) that evaluated teriparatide therapy for its combined effect on osteoporosis and fracture healing in older patients with FFP and observed a significantly shorter time to fracture healing and improved functional outcome in the therapy arm. However, teriparatide therapy requires daily subcutaneous administration and regular laboratory checks. In this regard, Shum et al. 28 reported that patients’ acceptance of teriparatide therapy was inferior to that achieved in an RCT study setting and could not be reproduced in routine clinical practice regarding implementation rate, frequency of side effects, and pathological findings in laboratory controls, as reported in a previous RCT involving patients with FFP. Åkesson et al. 29 highlighted the need for postfracture care, which includes fracture liaison services programs, geriatric/orthogeriatric services, and osteoporosis liaison service programs. These are systematic, coordinated care programs that identify, evaluate, and manage patients who sustained fragility fractures, with the goal of preventing further fractures, because fragility fractures are associated with high rates of disability, loss of independence, and reduced quality of life for patients and their caregivers. A multidisciplinary approach is required to improve the general condition of patients and treat the underlying metabolic abnormalities. 3
This study has some limitations. First, the reported time of injury depended on the memory of the patient; therefore, the time of injury was unclear for a number of patients. Second, the fracture type was classified not only at the time of admission but also at the final diagnosis. Third, the number of patients with types II and III fractures was small.
As indicated by FAC, the recovery rate of walking ability to the pre-injury state at 1 year after injury was 80% for Rommens classification type I, 100% for type II, 44% for type III, and 53% for type IV. Most cases of types IIIa, IIIb, and IVa presented with delayed union. The presence of cancer and more than four-week bed rest, with a two-level decrease in FAC, were risk factors for a significant decrease in walking ability.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The protocol for investigating the clinical outcomes and radiological findings was approved by the Ethics Review Committee of the University of Fukui (20140046), and informed consent was obtained from all patients.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.