
Abstract
Introduction:
Geriatric-orthopaedic co-management models can improve patient outcomes. However, prior reports have been at large academic centers with “closed” systems and an inpatient geriatric service. Here we describe a Geriatric Fracture Program (GFP) in a mixed practice “pluralistic” environment that includes employed academic faculty, private practice physicians, and multiple private hospitalist groups. We hypothesized GFP enrollment would reduce length of stay (LOS), time to surgery (TTS), and total hospital costs compared to non-GFP patients.
Materials and Methods:
A multidisciplinary team was created around a geriatric Nurse Practitioner (NP) and consulting geriatrician. Standardized geriatric focused training programs and electronic tools were developed based on best practice guidelines. Fracture patients >65 years old were prospectively enrolled from July 2018 – June 2019. A trained biostatistician performed all statistical analyses. A p < 0.05 was considered significant.
Results:
564 operative and nonoperative fractures in patients over 65 were prospectively followed with 153 (27%) enrolled in the GFP and 411 (73%) admitted to other hospitalists or their primary care provider (non-GFP). Patients enrolled in the GFP had a significantly shorter median LOS of 4 days, compared to 5 days in non-GFP patients (P < 0.001). There was a strong trend towards a shorter median TTS in the GFP group (21.5 hours v 25 hours, p = 0.066). Mean total costs were significantly lower in the GFP group ($25,323 v $29085, p = 0.022)
Discussion:
Our data shows that a geriatric-orthopaedic co-management model can be successfully implemented without an inpatient geriatric service, utilizing the pre-existing resources in a complex environment. The program can be expanded to include additional groups to improve care for entire geriatric fracture population with significant anticipated cost savings.
Conclusions:
With close multidisciplinary team work, a successful geriatric-orthopaedic comanagement model for geriatric fractures can be implemented in even a mixed practice environment without an inpatient geriatrics service.
Introduction
The burden of geriatric fractures is expected to increase dramatically over the next several decades, with hip fractures alone reaching an estimated 6.26 million by 2050 world-wide. 1,2 With a rapidly aging population that is at risk for falls, 3 patients with fragility fractures comprise a sizeable portion of orthopaedic practice. It is estimated that nearly half of all women and up to 22% of men will suffer an osteoporotic fracture in their lifetime, often with significant morbidity and mortality. 4 -6 As these patients often have complex medical, surgical, and rehabilitative needs, a multidisciplinary approach is necessary to ensure that these patients have the best possible outcomes.
A combined approach to the care of geriatric fracture patients was first reported in the early 1990s, with a specific emphasis on geriatric and orthopaedic co-management. 7,8 These early studies showed significant improvements in postoperative complications, improved function, and lower discharge rates to nursing homes. 7 Subsequent studies using an “Orthogeriatric” model have also shown shorter time to surgery (TTS), shorter lengths of stay (LOS), lower readmission rates, reduced in-hospital mortality, 9 -11 and lower cost of care. 12,13 However, these reports often come from large academic centers whose physicians are largely employed faculty or who have dedicated geriatric units. 14 -21 In hospitals staffed with multiple private practice groups or individuals, or in those who do not have an inpatient geriatrics program, the implementation of a protocol-driven approach to patient care is challenging because of lack of cohesion, competition, or contrasting care models. Nonetheless, given the scope and breadth of geriatric fracture needs, it is critical that models for geriatric fracture care programs also be developed for these settings.
Our institution is a 900 bed, urban, academic tertiary care medical center and urban level 1 trauma center, with a mixed medical staff model that includes private and employed physicians and ACGME fellowship and residency training programs. While there is no dedicated geriatric unit or inpatient geriatric service, there is robust hospitalist support. We introduced the Geriatric Fracture Program (GFP) as a pilot program in July 2018, seeking to establish a protocol-driven model to provide evidence-based treatment for geriatric fracture patients that could ultimately be extended to all members of the medical staff. We hypothesized that those patients enrolled in the GFP would have quicker TTS, shorter LOS, and reduced total costs compared to those who were not enrolled. Prior to our intervention, there was no organized pathway focused on optimizing care for geriatric fracture patients.
Methods
Program Overview
The mission of GFP is to provide high-value, geriatric-centered care that manages the injury in the context of the patient as a whole and strives to return the patient to a meaningful life in a timely manner. GFP uses a combination of multidisciplinary education, evidence-based clinical protocols, documentation tools and geriatric-centered goals of care. This care model provides an opportunity to close gaps in care, ensure quality and safety, and enhance value and improve outcomes for patients.
Goals for the program include reducing time to surgery of 24 hours or less, achieving inpatient length of stay of 5 days or less, maintaining post-operative delirium rates of less than 20%, and performing post-discharge comprehensive geriatric assessment to address fall risk and osteoporosis management.
Program Development
Vital to successfully implementing a project in a large hospital environment is building a team of champions and strong supporters. The impetus for the development for the program began with the Department of Orthopaedic Surgery and Chief of Geriatrics in March 2018. Leadership from Orthopaedics and Geriatrics then engaged with the Inpatient Specialty Program (ISP), the largest private hospitalist group in the medical center, and hospitalist champions from ISP were identified. Additionally, this group manages a team of nurse practitioners (NP) who ensure smooth care transitions to and the close clinical oversight of patients discharged to 8 local skilled nursing facilities for post-discharge care. 22
Central to GFP was a dedicated Geriatric NP with a background in orthopaedics and geriatrics who was designated program manager and served as a liaison between each group. Department and division champions met for several months to define the goals, identify stakeholders, and develop training programs for physicians and nurses. As the medical center does not have an inpatient geriatrics program, the ISP hospitalists underwent geriatric-specific training by geriatric faculty with a special focus on peri-operative management based on ACS / NSQIP AGS perioperative guidelines. 23 This included training on recognition of and appropriate treatment of geriatric syndromes such as delirium, polypharmacy and pain management. This also included education regarding the domains of comprehensive geriatric assessment and how to utilize templates that incorporated screening and assessment tools for geriatric syndromes. In addition, all nursing staff on the orthopaedic unit underwent training on the importance of how physiologic changes in geriatrics must inform nursing care, including: the recognition and early management of delirium using the Confusion Assessment Method (CAM); 24 polypharmacy; and opioid reduction techniques as well, led by the dedicated Geriatric NP. Additionally, templates for patient intake, delirium assessment, and daily rounding were developed and published in the electronic medical record (EMR) system to assist with standardization of patient care. These templates focused on functional assessment, cognitive assessment, delirium screening, and goals of care.
Geriatric Pain Management
In addition to the geriatric-centered training, a comprehensive pain management program was developed in partnership with the division of regional anesthesia and hospital pharmacy staff. We developed an evidence-based protocol for early non-opioid pain control centered around fascia iliacus (FI) blocks. 25 -33 Orthopaedic residents also received training during their didactic curriculum on delirium, pain management, opioids, and the role of regional anesthesia. Pre- and post-operative pain medication regimens and orders for regional anesthesia were included in the GFP order sets, and orthopaedic residents were instructed to contact the regional team when they were consulted on a hip fracture. Furthermore, the Emergency Department medical director participated in the development of the pain management protocol and provide logistical support for early regional anesthesia in the form of storage of supplies and ultrasound machine use.
Operating Room Availability
A critical factor in reducing morbidity in hip fractures is timely surgery. 34 -38 To achieve this, the Orthopaedic Trauma Service—comprised of fellowship-trained employed faculty—was invited to participate in the program. As the hospital is also a level I trauma center, this created availability for an all-day trauma room during the week. They agreed to provide care for eligible patients, thereby avoiding “add-on” status and unnecessary delays in surgery. All fragility fracture patients were considered urgent and prioritized for surgery as soon as medically appropriateWhile there was no formal dedicated orthopaedic trauma time on the weekend, given the volume of cases and operative needs, a full day orthopaedic room for weekend cases was made available approximately 95% of the time on Saturdays. On weekend days where dedicated time was not available, emphasis was placed on the importance of early operative intervention for patients and the on-call orthopaedic surgeon performed the case as soon as time was available rather than reschedule the case for Monday.
Program Implementation
A challenge to the implementation of this program was the medical center’s pluralistic nature. The medical center has a robust pluralistic clinical environment with a mix of academic and private practices, so interventions needed to blend within this existing culture. Given the multiple private hospitalist groups and other private physicians, it was not possible to enroll every patient over 65 years old who presented with fragility fracture to the GFP-trained hospitalist service. The Medical Director of the Emergency Department helped the GFP team understand how admissions were triaged and time involved in admitting patient and to which service. Furthermore, each internist or primary care provider often had his or her own preferred orthopaedic surgeons to consult for fracture care. As such, it was necessary to clearly define which patients would be considered candidates for GFP enrollment.
When the ISP hospitalist service was involved with a geriatric fracture patient, they were admitted to the GFP hospitalist service (patients would get referred to ISP vs another physician or hospitalist group for a variety of reasons, including certain insurance types or preference of the PCP).
Regardless of GFP enrollment, all patients with a primary diagnosis of fracture were admitted or referred to the orthopaedic surgery unit. If the patient was enrolled in GFP, the ISP hospitalist performed a medical preoperative evaluation within 6 hours of admission and used the electronic GFP documentation template as a guide. Nursing staff administered a CAM survey to screen patients for delirium for all patients in addition to their usual intake process. For hip fractures specifically, the regional anesthesia team was contacted to offer the patient a fascia iliaca (FI) block if they had not already received one in the emergency room.
Multidisciplinary rounds occurred daily Monday – Friday. The multidisciplinary rounds (MDRs) were led by the geriatric NP, and participants included a case manager, an ISP hospitalist, a pharmacist, a physical therapist, orthopaedic surgery trainees and the bedside nurses. The goal of the MDRs was to review the ACS NSQIP and AGS perioperative geriatric checklist 23 , with special focus on delirium recognition, treatment, and transitions of care. For example, nursing staff were educated to repeat the CAM assessment daily on all patients. The CAM result was also included in orthopaedic resident’s and hospitalist’s progress note templates to ensure that presence of delirium was discussed on daily rounds, given both high prevalence and high morbidity associated with delirium in hip fracture patients.
Patients enrolled in the GFP were evaluated by the NP coordinator who also served as a resource and educator for all nursing staff. The NP also educated patients and families about osteoporosis and fall prevention, and patients were scheduled with a geriatrician approximately 6-week post discharge for bone health follow up.
Program Maintenance
A GFP working group with representatives from Orthopaedics, Geriatrics, the ISP hospitalist team, Nursing, Pharmacy, and Physical Therapy met monthly to review issues and make improvements in the program. An additional stakeholder group comprised of clinical leadership also met quarterly to review performance measures and discuss strategic directions. The Geriatric NP was critical to both meetings for following up on action items and overall maintenance of the program’s focus and direction.
Data Collection and Statistical Analysis
Patient enrollment began July 1, 2018 and continued through June 30, 2019. All patients over 65 presenting with a fragility fracture were prospectively followed. Patients fell into 1 of 2 cohorts: GFP and non-GFP (non-GFP patients received standard care). Demographic information, preoperative comorbidities, time of admission, diagnosis, additional cardiac diagnostic procedures performed, time to surgery, type of surgery, length of stay, and 30-day readmission rates were recorded. Total hospital charges were recorded for all patients.
Continuous variables were compared with a one-way analysis of variance. Categorical variables were compared using a chi-square or Fischer’s exact test. For non-parametric data, median values and interquartile (IQR) values were compared using a Kruskal-Wallis test. A p < 0.05 was considered significant. American Society of Anesthesiologists (ASA) score between GFP and non-GFP were compared via Fischer’s exact test.
Results
564 operative and nonoperative fractures in patients over 65 were prospectively followed with 153 (27%) enrolled in GFP, and 411 (73%) admitted to other hospitalists or their primary care provider (non-GFP). There were no demographic differences between cohorts in terms of age (83 v 83, p = 0.35) and sex (73% female v 73% female, p = 0.91). There was no statistically significant difference in the distribution of ASA scores between the GFP and non-GFP cohorts (ASA 3 or 4, 60% v 65%, p = 0.457).
All Patients
There were a total of 285 (51%) hip fractures, 137 (24%) other lower extremity and pelvis fractures, 36 (6%) periprosthetic fractures, and 106 (19%) upper extremity fractures. There was no difference in the distribution of fracture types between cohorts (p = 0.726). Similarly, there were no differences in the median age of the patients between cohorts (83 v 83, p = 0.35). Similar proportions of patients underwent surgery between the GFP and non-GFP cohorts (73% v 73%, p = 1). Mean total costs were significantly lower in the GFP group ($25,323 v $29085, p = 0.022). There were no differences in 30-day readmission rates between groups (2.6% v 1.7%, p = 0.5).
Operative Patients
Patients enrolled in the GFP who underwent surgery had underwent significantly fewer preoperative transthoracic echocardiograms (14% v 25%, p = 0.005) as part of their preoperative risk stratification. Operative GFP patients had a significantly shorter median LOS of 4 days, compared to 5 days in unenrolled patients (P < 0.001). However, there was no statistical difference in TTS in the GFP group (21.5 hours v 25 hours, p = 0.066). There was no difference in the types of fractures or discharge disposition between the GFP and the non-GFP groups (Table 1).
Types of Fractures and Disposition for Operative Fractures.
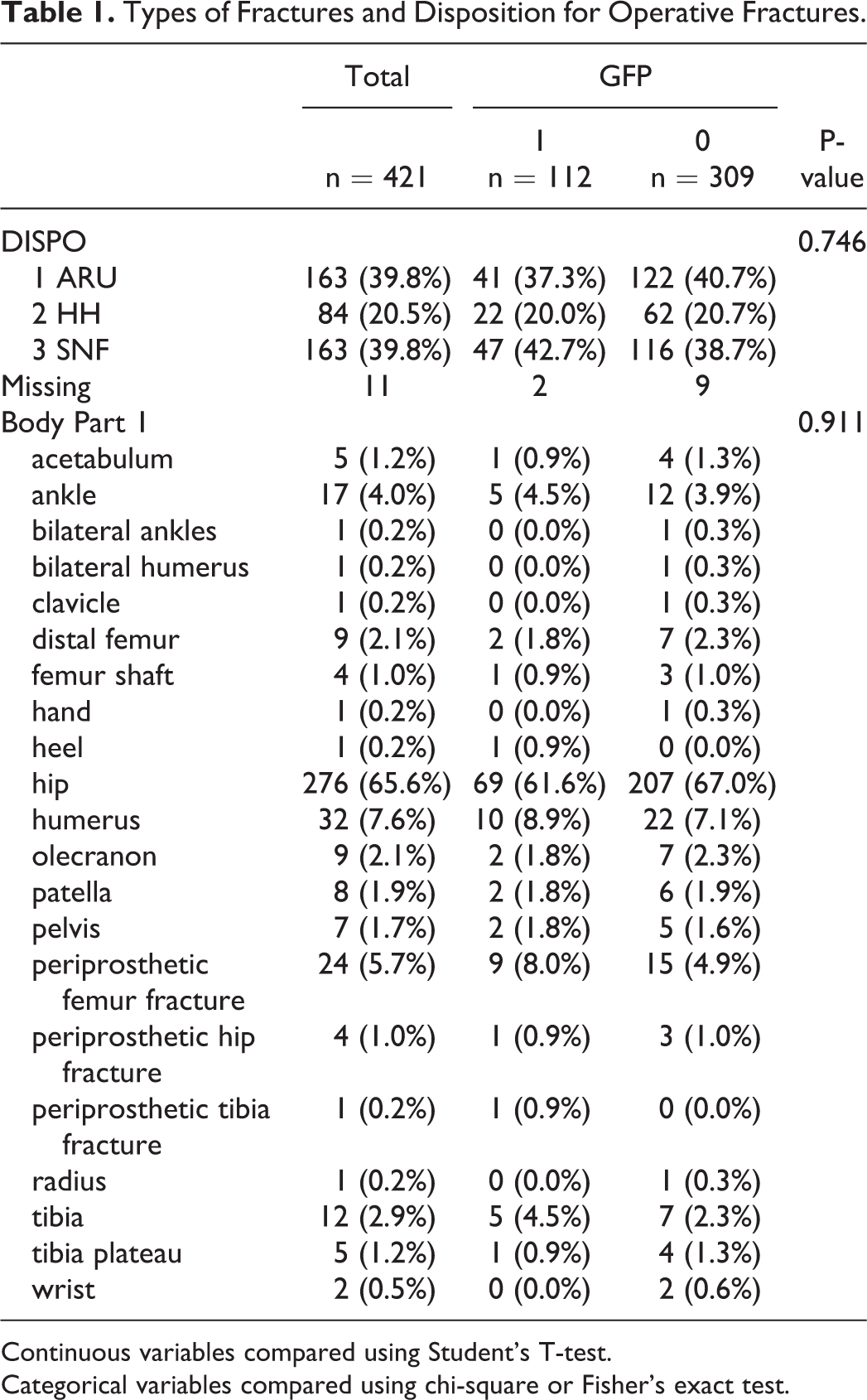
Continuous variables compared using Student’s T-test.
Categorical variables compared using chi-square or Fisher’s exact test.
Nonoperative Patients
In the nonoperatively treated group, the median LOS was significantly lower in the GFP group with a median of 3 days compared to 5 days (p = 0.034) in the non-GFP group. There was no difference in the types of fractures or discharge disposition between the GFP and the non-GFP groups (Table 2).
Types of Fractures and Disposition for Nonoperative Fractures.

Discussion
Geriatric fracture patients continue to present many challenges to our current medical system. Patients often present with a myriad complex medical, functional, and social needs, have significant risk for morbidity and mortality, 21,39 -42 and the number of patients at risk for these fracture continues to grow. 43 In fact, Kates et al predicted that more American women will die from complications associated with hip fractures than from breast, ovarian, and uterine cancer combined. 44 As such, coordinated multidisciplinary care is crucial to ensuring an optimal outcome.
Multiple studies over the last several decades have shown significant benefits of involving a geriatrician. 8,9,15,16,21,45 -47 Grigoryan et al performed a meta-analysis of all Orthogeriatric combined care models. The group divided the existing literature into 3 models: routine geriatric consultation, a dedicated geriatric unit, or orthopaedic and geriatric co-management. They found that geriatrics involvement in the inpatient setting reduced inpatient mortality as well as long-term mortality. 48 However, every trial studied included direct inpatient management by a geriatrician in some form, a service that is not always available in many settings. Given this, a model that relies on the presence of an inpatient geriatric service may not be widely reproducible.
Our study describes one method of implementing a geriatric fracture program without an inpatient geriatric service, but rather with education of existing services by geriatric faculty. Our medical center has a variety of subspecialty services available, but nothing was more valuable than departmental and division leadership who were passionate about establishing the GFP care model and who were willing to devote time, energy, funding, and personnel to ensure its success. In fact, Kates et al noted in their survey evaluating barriers to implementing a geriatric fracture program that lack of physician leadership, along with a lack of a clinical case manager, lack of anesthesia support, lack of operating room time, and difficulties with preoperative cardiac evaluation were among the major barriers in more than 70% of institutions. Lack of medical or geriatric leadership was cited as a “severe barrier” to implementation. Surprisingly, most respondents did not see surgical leadership or hospital administration as a barrier. 49
While our institution does not have an inpatient geriatric service, we do have a Section of Geriatric Medicine within the Department of Medicine. That leadership was heavily involved in designing education programs, outreaching to hospital leadership, and in the recruitment, engagement, and education of the ISP hospitalists. The clinical model for the Section of Geriatric Medicine is an ambulatory care model. The ISP hospitalist team was chosen because of its already well-established care transitions program at nursing homes and the extensive network of outpatient primary and specialty care providers. 22,50 Having these factors already in place significantly reduced the amount of time required to conceptualize and implement the program. The creation of templates and order sets happened in parallel to early program implementation, and early patient enrollment experiences directly fed back to template design. All these factors allowed for rapid program implementation.
There are several limitations to this study. The overall sample size was relatively small; however, despite this we were able to show significant improvements with key metrics, particularly with regards to less preoperative cardiac testing, lower length of stay, and decreased total costs. There was a strong trend towards shorter time to surgery as well. It is worth noting (and encouraging to see) that even though patients in the non-GFP appeared to have longer hospital stays, both cohorts had TTS within or near 24 hours and their LOS was within goals previously established by other programs and the national average. 13 While the patients were sorted into the 2 cohorts, we may have experienced some Hawthorne effect: All patients were admitted to the same orthopedic unit and were cared for by the same nurses, all of whom had undergone geriatric-specific training. In addition, it was not uncommon that patients in the different cohorts were seen by the same surgeon or the same inpatient nurse. Additionally, as the GFP NP was frequently on the unit, she was always available for (and often assisted) unit nurses with questions, assessments, and occasional consultations. Thus, all geriatric fracture patients on the unit benefited from the nursing education efforts and from the availability of the GFP NP. We also recognize that our model allowed for other potentially confounding variables that developed over time, such as the use of FI blocks.
There are several strengths to our program, most notably the close collaboration between the Section of Geriatric Medicine, a private inpatient hospitalist program, the dedicated NP, and the enthusiastic adoption of GFP goals by orthopaedic nursing staff. Additionally, the pluralistic environment of the medical center provided a natural experiment by which we could compare specific interventions related to the GFP versus broader cultural changes within the institution. The crossover between surgeon and nursing care between groups, while considered a limitation from a statistical standpoint, can be considered a major strength in terms of clinical care, as the effort to implement the GFP for a subset of patients required training of health care providers who care for many other patients. Thus, GFP educational efforts could lead to improved outcomes for patients not just on the orthopaedic ward but throughout the hospital.
Another major strength of the GFP model was its financial efficiency. Specifically, very few additional resources (other than the dedicated NP) were needed to implement the program. This means that the program is more easily scalable within our own organization and potentially easier to reproduce in other organizations. Hospitalist and Nursing training will be ongoing, as will the need to monitor adherence to protocols, but program expansion in its current form does not require additional staff. The educational aspects and templates are easily disseminated, so no additional hospital resources are necessary to expand the program to private physicians and other hospitalist groups.
Notably, enthusiasm for the program from hospital administration, patients and nursing has also led to growing interest from the other hospitalist groups, and we have formalized GFP elements as a “package” they can implement to improve patient care consistency while reducing concerns for competition between groups. At this time, institution-wide interest in the program has grown so that 2 additional private hospitalist groups have requested to be involved and are undergoing training.
Our intent is that participation in GFP continues to grow organically, so that additional patients cared for my private practitioners outside of hospitalist groups may also benefit without disrupting the hospital’s current culture. With the increasing inpatient burden of elderly and super-elderly patients, 51 geriatric-specific education and care will likely be needed for every specialty, not just in orthopaedics. Our program outlines one method by which institutions that are not academic medical centers may develop and implement a geriatric-focused program to improve the care of this vulnerable and growing population even without the benefit of a dedicated inpatient geriatric service. In doing so, we hope to provide an additional method by which a variety of institutions may improve the care of this vulnerable and growing population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.