
Abstract
Keywords
Introduction
Hip fractures have been associated with high rates of morbidity, mortality, and financial distress, especially among the elderly population.1–11 With a growing ageing population, the worldwide incidence of hip fractures is projected to significantly increase by 2050.12–14 A less common subtype of hip fractures is an isolated fracture of the greater trochanter (GT).15–18 In contrast to the adolescent avulsion injury, these fractures in the elderly and osteoporotic typically occur as a result of direct trauma.19–22 Although the incidence of isolated GT fractures is lower than conventional hip fractures, evidence still shows comparable mortality rates between the two fractures, underscoring the importance of proper medical and surgical management. 23
Diagnostic and treatment guidelines for GT fractures have not been adequately defined. In contrast to other conventional hip fractures, standard radiographs alone do not reliably display the extent of the GT fracture, particularly extension into the intertrochanteric (IT) region.24–26 Some suggest up to 90% of injuries initially diagnosed as isolated GT fractures on radiographs have occult IT extension on advanced imaging.27–28 While isolated GT fractures in patients may appear mild or even asymptomatic, 21 IT extension is considered a risk factor for fracture displacement, and thus morbidity, mortality, more complex surgery, and prolonged hospital length-of-stay and rehabilitation.29–30
Beyond computed tomography (CT), magnetic resonance imaging (MRI) has been shown to be the most sensitive imaging modality for identifying occult fracture propagation into the IT region.15,22,24–28,31–33 Therefore, some studies have suggested that all patients with isolated GT fractures identified on plain radiographs undergo MRI for assessment of IT extension.15,27 However, even with occult fracture extension on MRI, treatment debates remain. There are reports of successful outcomes with conservative management of isolated GT fractures, 16 while others recommend immediate surgical management for fractures with IT extension found on MRI.22,32–33
Therefore, this study sought to investigate the diagnostic and treatment protocols for isolated GT fractures at our institution—an urban, Level I trauma center. Specifically, we aimed to evaluate adherence to our own protocols for this injury. Additionally, we aimed to evaluate short-term outcomes in patients whose care deviated from protocol. We hypothesized that the majority of patients with isolated GT fractures would have an MRI to look for IT extension, and operative intervention would directly correlate to MRI findings.
Materials and methods
Institutional diagnostic and treatment protocol
Our current protocol for GT fractures is based upon fracture extension into the IT region, as seen on MRI. GT fractures with ≤ 50% IT extension, in the coronal and axial planes, are treated nonoperatively with an initial protected weightbearing and close follow-up with radiographs. For fractures with > 50% extension into the IT region, surgical stabilization with cephalomedullary nail or sliding hip screw is recommended. Patients with IT extension seen on radiographs or CT imaging are considered to have an IT fracture and are treated as such. While these are current treatment protocols, the decision for operative and nonoperative management of every patient is ultimately a balanced decision that weighs risks, benefits, and potential outcomes based on patients’ comorbidities and overall health status.
Patients and imaging
After Institutional Review Board approval, all adult patients (≥18 years old) presenting with a GT fracture over a 7-year period (10/2015–12/2021) were identified via query of our institution's billing database. We searched based on CPT codes 27244 (treatment of IT, peritrochanteric, or subtrochanteric femoral fracture; with plate/screw type implant, with or without cerclage), 27,245 (treatment of IT, peritrochanteric, or subtrochanteric femoral fracture; with intramedullary implant, with or without interlocking screws, and/or cerclage), 27,246 (closed treatment of GT fracture, without manipulation), 27,248 (open treatment of GT fracture, includes internal fixation when performed) as well as ICD-10 diagnosis codes of S72.11 (fracture of GT of femur). Patients were excluded if the injury was periprosthetic, had a ballistic mechanism, or there were any concomitant fractures of the femoral head, neck, or shaft identified on plain radiographs. Patient demographics, medical history, treatment, and outcomes were then tabulated via chart review.
We also evaluated whether each patient received both CT and MR imaging of the affected hip. This imaging was reviewed by an orthopedic surgeon (J.S.). Radiographic imaging and MR imaging variables encompassed time from injury to MRI, MRI characteristics, specifically whether fluid crossed the IT line or the mid-coronal line (Figure 1), and whether a pre-operative CT was performed.
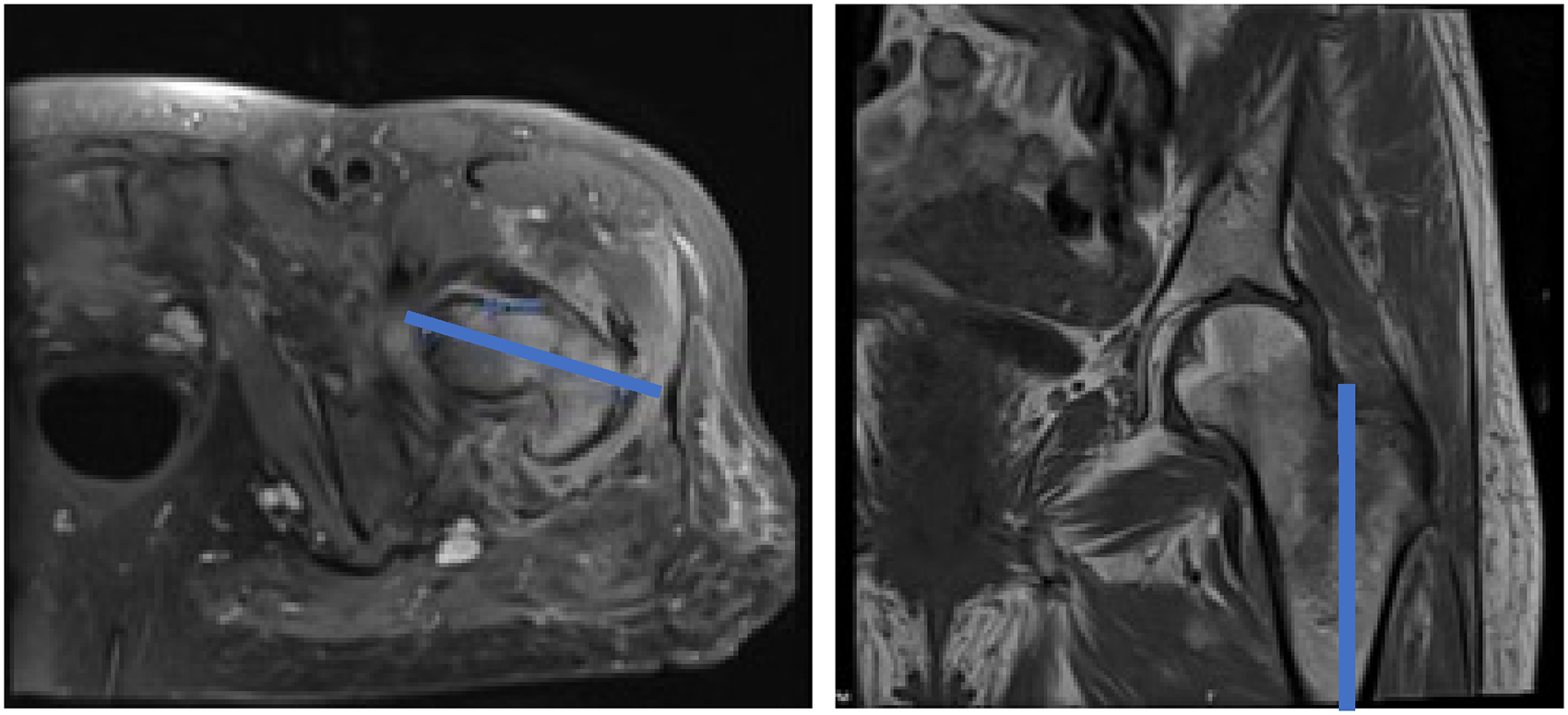
Magnetic resonance imaging of an isolated greater trochanter fracture demonstrating >50% fracture line extension on axial (left) and coronal (right) views.
Patient demographics, including but not limited to age, sex, body mass index (BMI), and Modified Frailty Index (mFI) were recorded. Characteristic data variables included initial presentation, length of stay, and associated injury complex. Injury Severity Score was also obtained from our institution's trauma registry. Treatment-specific information included whether the patient was initially managed conservatively or operatively, type of implant used (intramedullary nail versus sliding hip screw), and treatment outcomes. Clinic follow-up notes and subsequent emergency room visits were used to assess for post-injury adverse outcomes.
Statistical analysis
The data was analyzed to correlate injury presentation, frequency of occult fractures, and outcome of varying treatment options via descriptive statistics. Differences in average mFI scores between patients treated operatively and nonoperatively were analyzed utilizing Student's t-tests. Furthermore, in order to determine differences in average length of stay between patients treated operatively and nonoperatively, generalized linear regression was performed, controlling for age, sex, and mFI. Generalized linear regression was also utilized to determine differences in average length of stay between patients who received an MRI and those who did not, controlling for age, sex, and mFI. Statistical significance was set to p < 0.05. All analyses were performed using SPSS 25 (IBM Corp., Armonk, New York) and RStudio 1.2.133 (PBC, Boston, MA).
Results
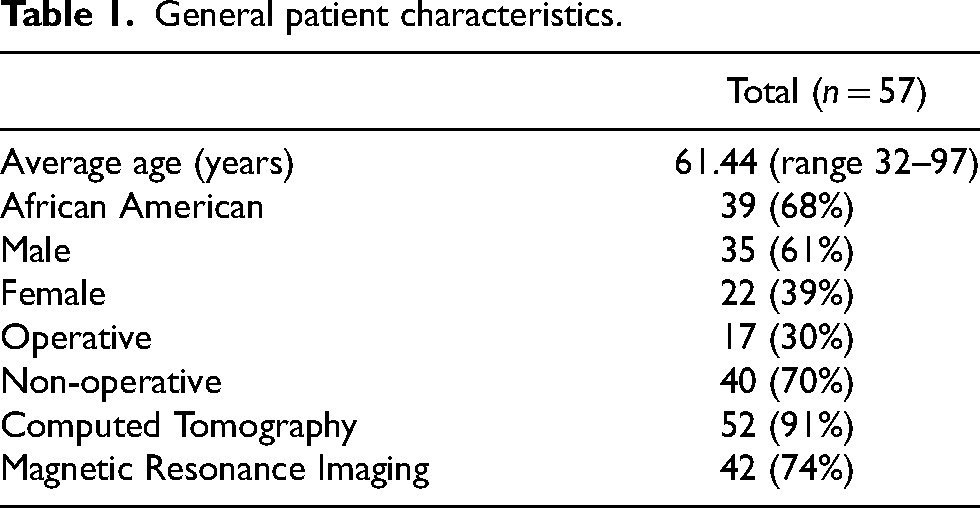
From January 2015 through December 2021, 212 patients were identified by our institutional query. Of those patients, 57 patients met our inclusion criteria with an isolated GT fracture (OTA/AO 31A1.1) (Figure 2). Patients were a majority male (61%), Black/African American (68%), and had an average age of 61 years (±14.7 years) (Table 1). In total, 52 of 57 patients (91%) had initial CT scans, but only 41 patients (72%) had an MRI (Table 1). From chart review of the 11 patients who did not have an MRI completed, no contraindications to MRI were identified. In total, 17 patients (30%) were treated operatively (11 intramedullary nails, 6 sliding hip screws) and 40 patients were managed nonoperatively with assistive devices and protected weightbearing (Figure 3). Patients treated nonoperatively were significantly healthier with a mean mFI of 0.5 versus 1.4 (p = 0.04). On average, those who were treated nonoperatively stayed 3.1 days longer than those treated operatively (11.6 days versus 8.5 days); however, when controlling for age, sex, and mFI, no significant difference was noted (p = 0.54). One intraoperative death was reported in the operative group.

Imaging of patient with right greater trochanteric femur fracture identified in non-operative treatment group. (A) AP pelvis XR identifying right greater trochanteric femur fracture. (B) Coronal view of CT. (C) Axial view of CT. (D) Axial view of MRI demonstrating fracture line extension. (E) Coronal view of MRI demonstrating intertrochanteric extension. GT: greater trochanter; MRI: magnetic resonance imaging; CT: computed tomography; AP, anterioposterior.
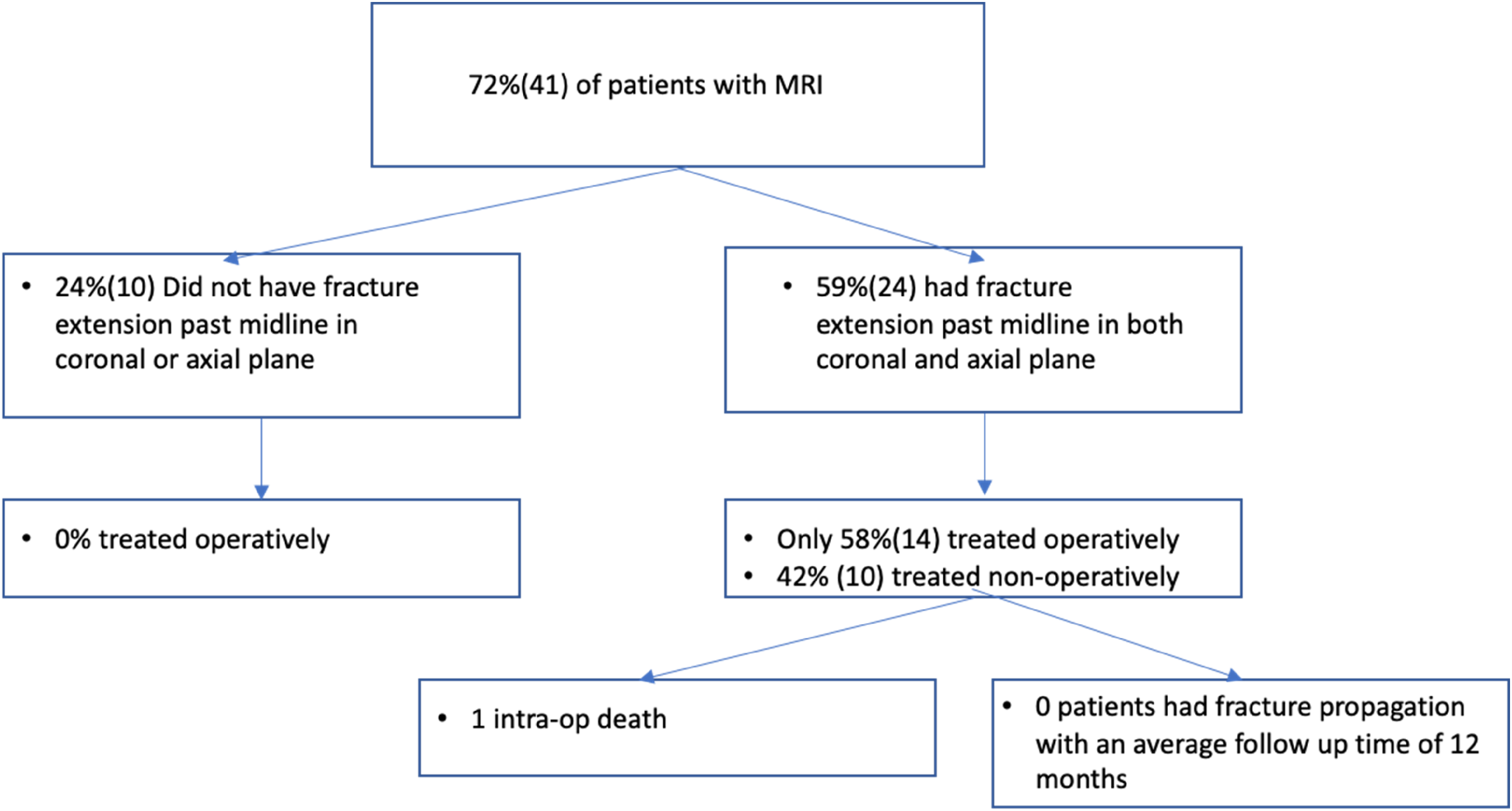
Treatment algorithm and outcomes of patients identified in the study based upon magnetic resonance imaging (MRI) results.
General patient characteristics.
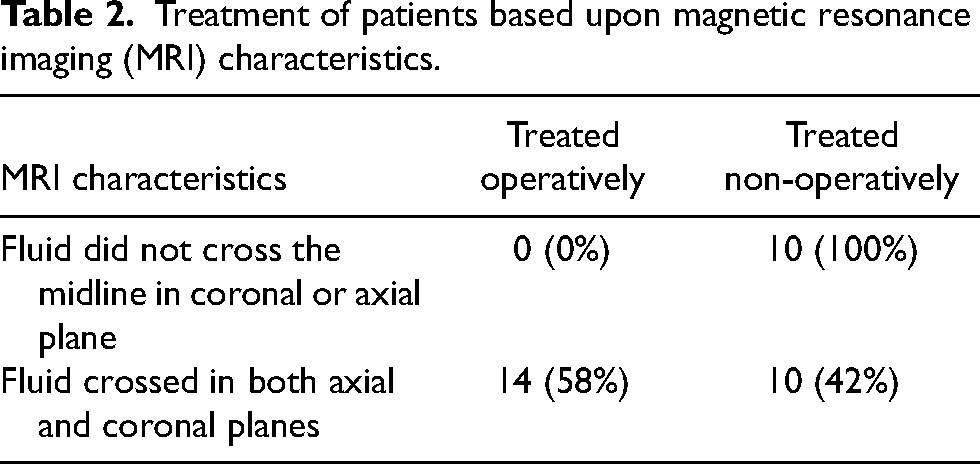
When analyzing patients that obtained MRI's, 10 of the 41 (24%) patients did not show >50% fracture line extension in either coronal or axial plane—all 10 of these patients were treated nonoperatively. In contrast, 24 of 41 (59%) showed >50% fracture line extension in both planes. However, of these 24 patients, only 14 (58%) were treated operatively (Table 2). Patients who received an MRI stayed on average 5.4 days longer compared to patients who did not receive an MRI (12.1 days vs. 6.7 days); however, when controlling for age, sex, and mFI, no significant differences were noted (p = 0.27). On review of outcomes for the 10 nonoperative patients with significant fracture line extension, eight patients had documented follow-up of 2-months or greater. None of these presented with further injury, surgery, or fracture extension (Figure 2).
Treatment of patients based upon magnetic resonance imaging (MRI) characteristics.
Discussion
Debate remains regarding the treatment of isolated fractures of the GT. Despite historical protocols based on the extent of fracture propagation into the IT region, surgeons still deviate from operative criterion when considering other patient and situational factors. The purpose of this study was to review our own institutional experience with isolated GT fractures and evaluate outcomes in patients whose care deviated from standard protocol.
In a retrospective review of patients presenting to our urban, Level I trauma center from 2015 through 2021 with isolated GT fractures, we found that our current protocol for advanced imaging is not consistently followed, with fewer than 3 out of every 4 patients receiving an MRI. Furthermore, the decision for surgical management appears to go beyond the MRI, as almost half of our patients with fracture extension >50% into the IT did not undergo surgery. However, despite deviations from surgical indications, our study also demonstrated that these patients treated nonoperatively had no differences in short-term outcomes—no increased length-of-stay and no increased risk of fracture propagation or subsequent injury.
Currently, our institution's protocols recommend that all patients with a GT fracture receive an MRI to assess for fracture extension into the IT region. Orthopedic literature has repeatedly made similar recommendations due to the ability of MRI to reveal the occult extension of the GT fracture, seen as signal intensification from the bony edema surrounding the occult fracture.22,24–28,31–36 However, Thomas et al. 37 believe the high sensitivity of MRI brings risk of unnecessary surgeries due to overestimation of the fracture line. The risk of surgery was unfortunately displayed in this review with an intra-operative death.
If MRI risks overestimation of injury, CT scans may suffice for the assessment of fracture propagation. In a similar fashion, CT is already widely accepted as a mode of evaluation for occult femoral neck fractures in the setting of femoral shaft fractures. In our patient population, 91% of patients received a CT. Thomas et al. 37 found a sensitivity and specificity of 100% in detecting occult hip fractures from isolated GT fractures utilizing multidetector CT. Dunker et al. 38 found a 95% sensitivity with CT in evaluating occult hip fractures, with no-false positives. Using CT, patients may still have an undetected fracture extension, but this occult injury pattern is likely appropriate for conservative treatment. 16
CT has several advantages over MRI, including decreased waiting time and greater patient compliance.37,39 As a result, a quicker diagnosis and initiation of treatment may lead to a shorter inpatient stay, decreased hospital costs, and lower mortality. 40 Our study demonstrated that patients who received an MRI stayed on average 5.4 days longer in the hospital compared to patients who did not receive an MRI. Although this was not statistically significant when controlling for patient comorbidities and demographics, further studies would be needed to assess relationship between hospital costs and utilization of resources. Another possibility for utilizing CT is in the detection of cortical bone integrity, which may be more critical for assessing fracture stability. Kim et al. 41 demonstrated that multiplanar CT had greater sensitivity in detecting cortical bone integrity compared to MRI. Thus, patients with decreased bone integrity after isolated GT fracture may be better candidates for surgical fixation while those with preserved stability continue with conservative treatment. Future research is needed to consolidate the impact of measuring bone integrity on treatment outcomes.
Even with fracture extension on advanced imaging, variability exists between proposed surgical indications and current practices. Our institutional protocol suggests that patients with a fracture extending >50% into the IT region on MRI should undergo surgical stabilization after careful consideration of patients’ general health and morbidity status. However, others such as Feldman et al. have suggested an even more aggressive strategy—surgical stabilization for any fracture extension beyond the base of the GT. 33 We had 24 patients with fracture extension past the midline on MRI, but only 14 of these patients underwent surgical stabilization. Despite this deviation from protocol, none of the nonoperative patients presented with further injury, surgery, or fracture extension. Additionally, we found no difference in length-of-stay between patients treated operatively and nonoperatively. These results agree in large part with several other studies that have advocated for conservative treatment.26,37,42–43 Our study cannot claim causation, but the results add to the argument that surgical indications likely involve factors additional to IT extension on MRI.
The present study has several limitations. First, the methodology relied on a retrospective chart review, which may introduce the potential for insufficient documentation. There may have been cases that were missed in the initial billing query. Additionally, documented weightbearing and physical therapy information was not available, limiting our ability to discuss mobility differences and outcomes. Furthermore, the present study only included a single urban medical center, which limits the generalizability of the study population to other healthcare settings. Future investigations should utilize a prospective study that considers these limitations to obtain a more comprehensive understanding of the most efficient, cost-effective diagnostic and treatment management for isolated GT fractures.
In conclusion, we reviewed our institutional management of patients with isolated GT fractures, discovering deviations from the institutional protocol. Fewer than 3 out of every 4 patients received an MRI, and even in patients who did receive an MRI, those with traditional operative indications did not all have surgery. However, these nonoperatively managed patients had no increased hospital length-of-stay or elevated risks of fracture propagation. Higher powered work with more robust follow-up is needed, but this retrospective review questions the need for MRI in all isolated GT fractures. Furthermore, there may be patients with fracture extension into the IT on advanced imaging who are still candidates for nonoperative management.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.