
Abstract
Anterior hip dislocation is a rare orthopedic emergency, usually following high-energy trauma. This injury is occasionally associated with acetabular fractures, femoral head fractures, or diaphyseal femoral fractures. However, the combination between the anterior hip dislocation and the ipsilateral ischial tuberosity and greater trochanter fractures is extremely rare, and very sparsely reported in the literature. This paper reports a case of an obturator type of anterior hip dislocation associated with a concomitant ipsilateral ischial tuberosity and greater trochanter fracture. The hip dislocation was reduced by closed means under general anesthesia, and the greater trochanter fracture was reduced and internally fixed with tension band in a second stage. Radiological and functional evaluation at 12 months after surgery, using the Harris Hip Score (HHS), was good.
Keywords
Introduction
Traumatic anterior dislocation of the hip is a relatively uncommon injury encountered in the emergency department. Early diagnosis and prompt reduction are crucial, as prolonged dislocation increases the risk of developing avascular necrosis of the femoral head, even in the absence of associated fractures. 1 Anterior acetabular rim and the adjacent wall, and fractures of the femoral head are relatively uncommon associated injuries 2 ;furthermore, associated ischial tuberosity and greater trochanter fractures are extremely rare.
Case report
A 50-year-old male presented to our emergency department following a high-velocity road traffic accident due to the collision of his motorcycle with a car. The patient was conscious, with Glasgow Coma Scale 15, hemodynamically stable, with severe pain in his left hip, the left limb was positioned in abduction, and external rotation and the femoral head could be palpated in the groin. There was no associated distal neurovascular deficit.
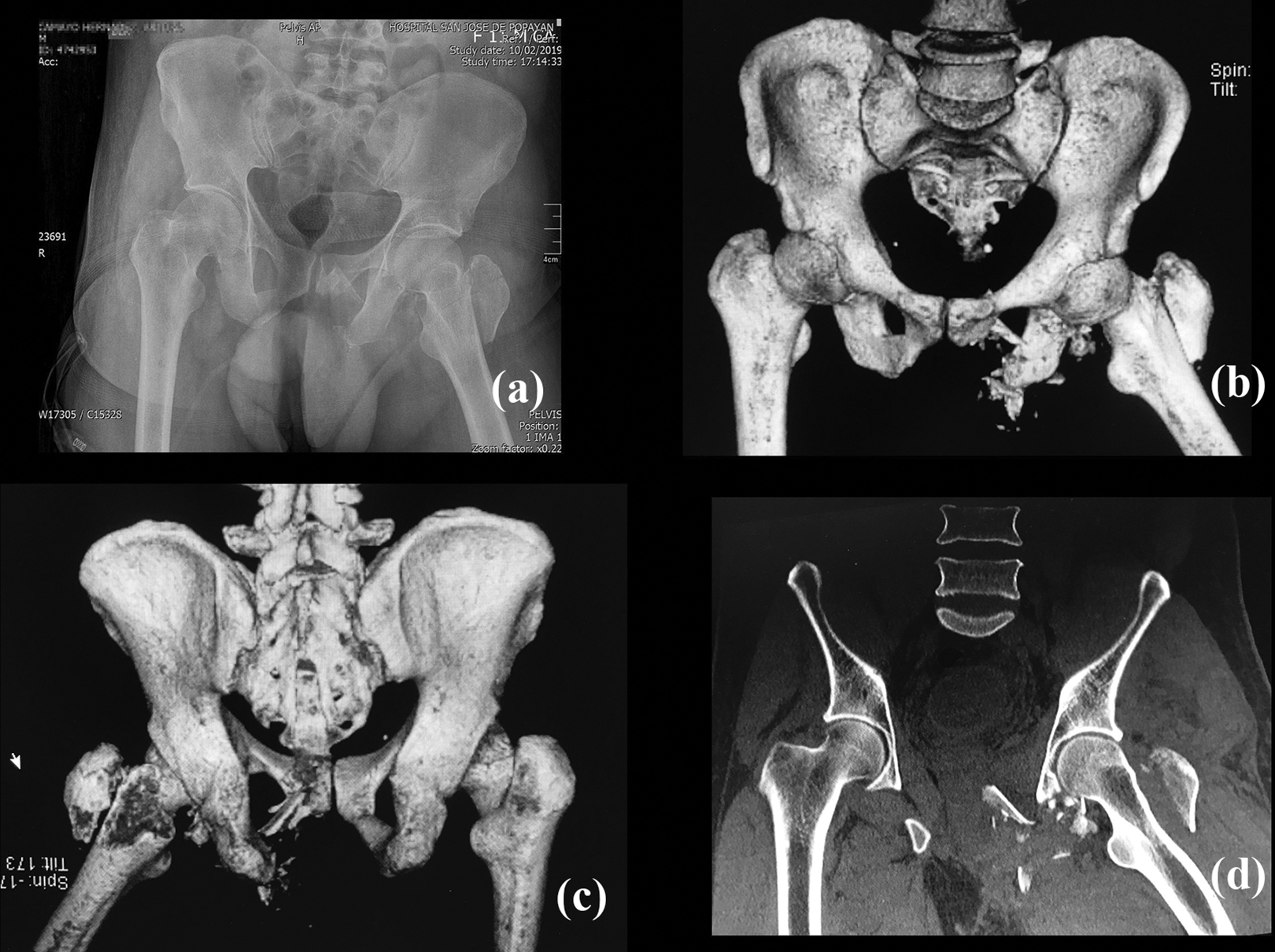
Initial radiographs showed an anterior obturator-type dislocation of the left hip associated with ipsilateral fracture of the ischial tuberosity and greater trochanter (Figure 1).

Initial presentation (a) and injury film (b–c).
Under general anesthesia, a closed reduction of the dislocation was performed within 2 hours of the accident using strong longitudinal traction along the femur with the hip in hyperextension, followed by flexion and internal rotation. Once closed reduction of the dislocation was achieved, the post-reduction imaging studies; pelvic X-Rays and a CT scan showed a congruent reduction of the hip joint along with a displaced fracture of the greater trochanter (Figures 2 and 3). Therefore, to maintain the adequate function of the abductor’s muscles open reduction and internal fixation were planned for the greater trochanter fracture in the elective theater. This mainly helps in reducing the incidence of abductor weakness and abductor limp postoperatively. The patient returned to the operating room a week later; using a lateral approach, the repositioned greater trochanter was then held by applying patellar clamps and stabilized by passing two 2.0 mm K wires from the greater trochanter into the anteromedial cortex of the distal femur and a 1.8 mm wire cerclage (Figure 4), the fracture of the ischial tuberosity was not fixed due to its comminution and because it did not cause instability of the pelvic ring.
Post-reduction imaging studies; pelvic X-Rays (a) and CT scan (b–d).
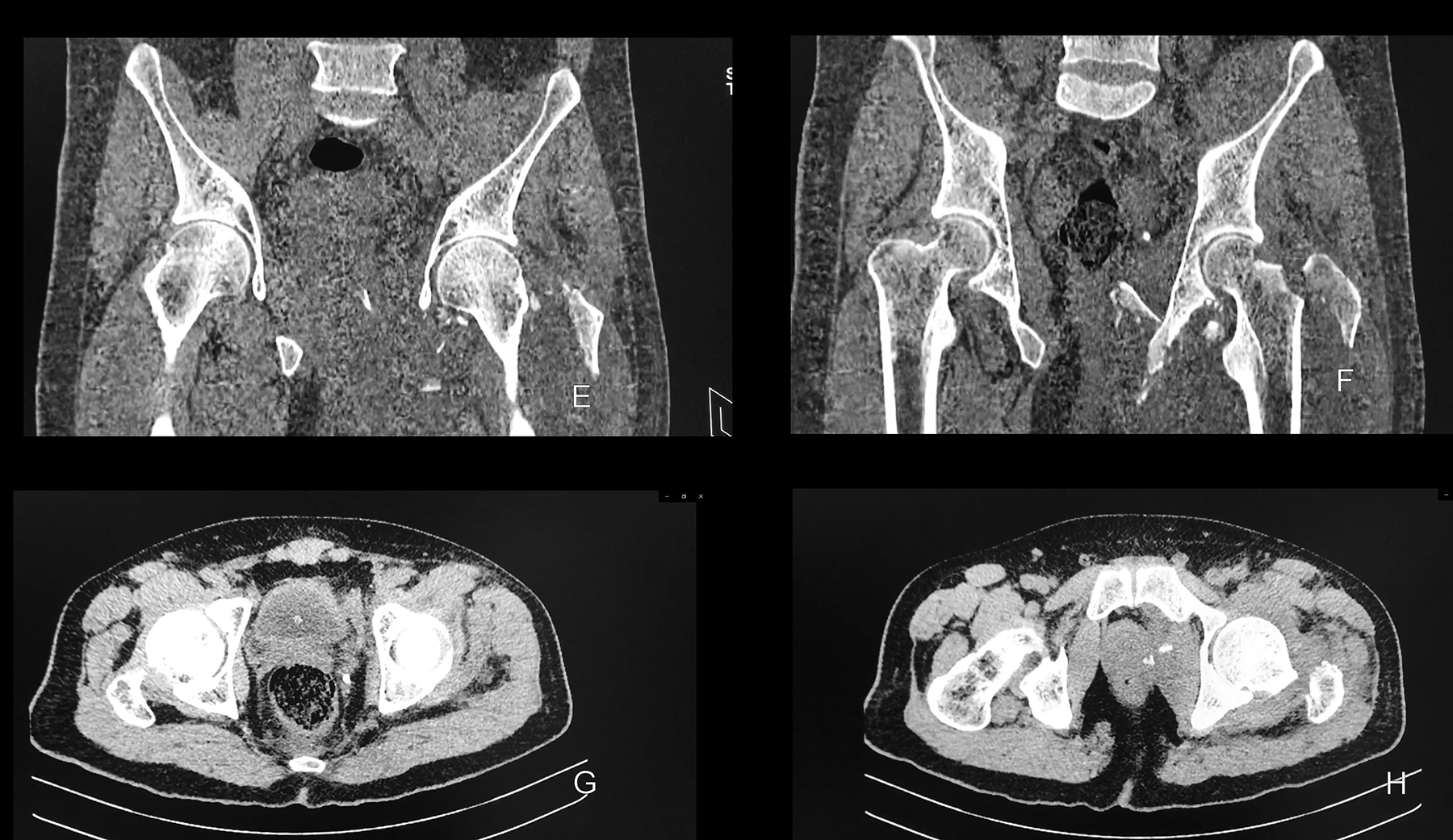
CT scan axial and coronal images.
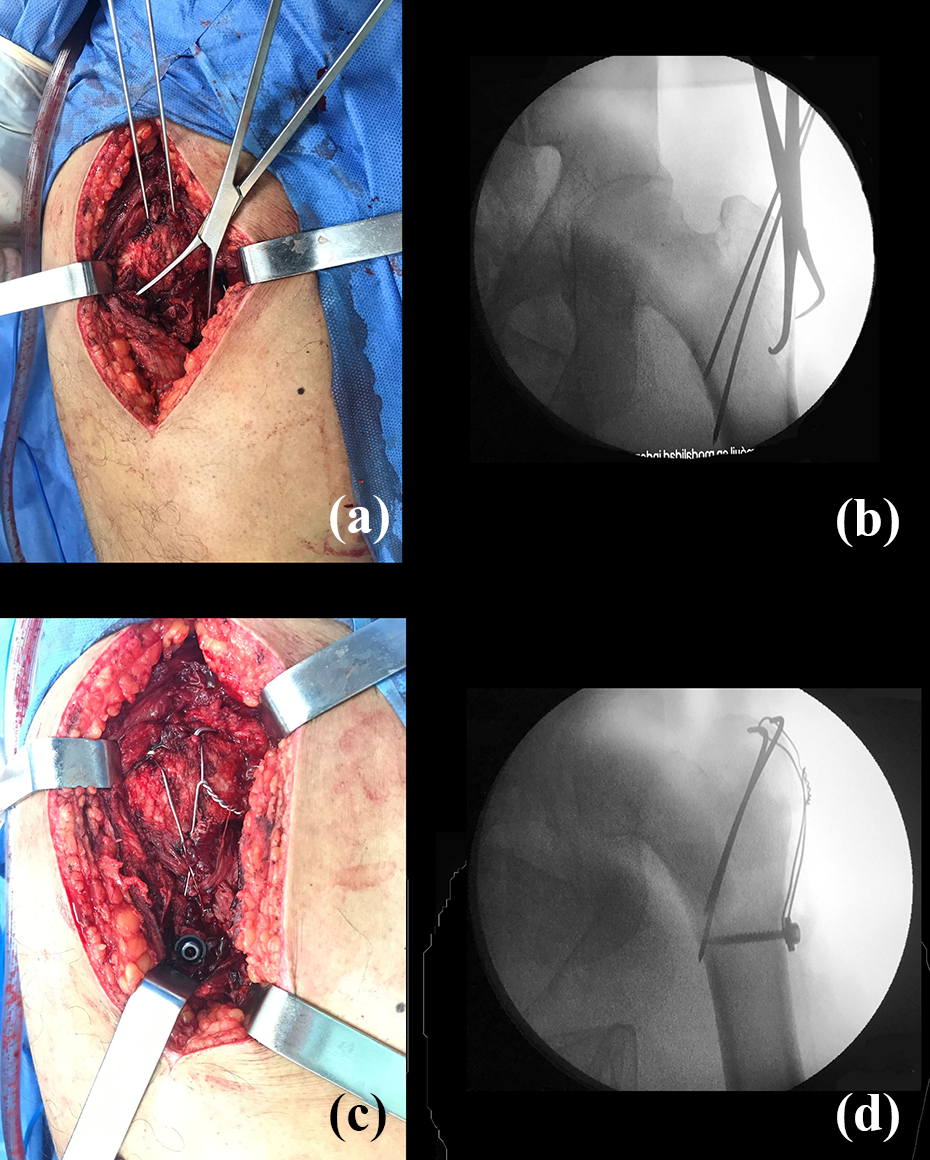
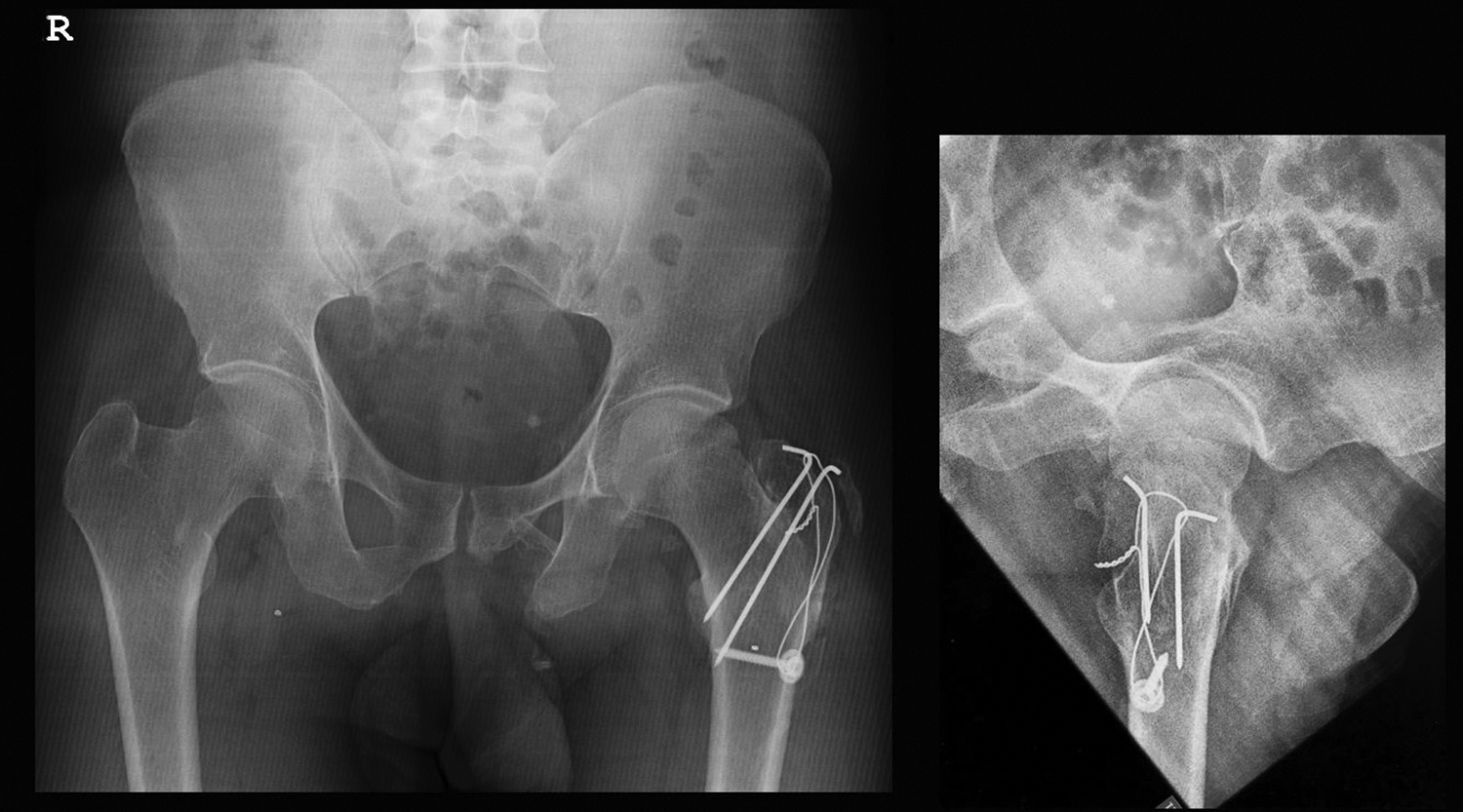
Open reduction and internal fixation of the greater trochanter using a tension band.
Physical therapy is started immediately after surgery by active hip joint mobilization exercises and walking without weight-bearing on the left lower limb is begun. Follow-up was carried out every 2 months, progressive weight-bearing of the injured limb was allowed at 2 months after surgery. By 6 months, radiographs showed signs of union of the great trochanter fracture (Figure 5); at this time, the patient was full weight-bearing with slight pain on long-distance walking with moderate limitation in range of motion: Flexion 0–95°, abduction 0–25°, adduction 0–20°, extension 0–10°, internal rotation 0–25°, external rotation 0–20°. There was a mild limp due to abductor’s muscles weakness. At the end of 1 year, the patient was asymptomatic and was able to sit cross-legged, squat, with a small loss of active and passive of the last degrees of internal rotation and hip abduction motion. X-Rays taken at 1-year revealed a complete union without signs of avascular necrosis of the femoral head (Figure 6).
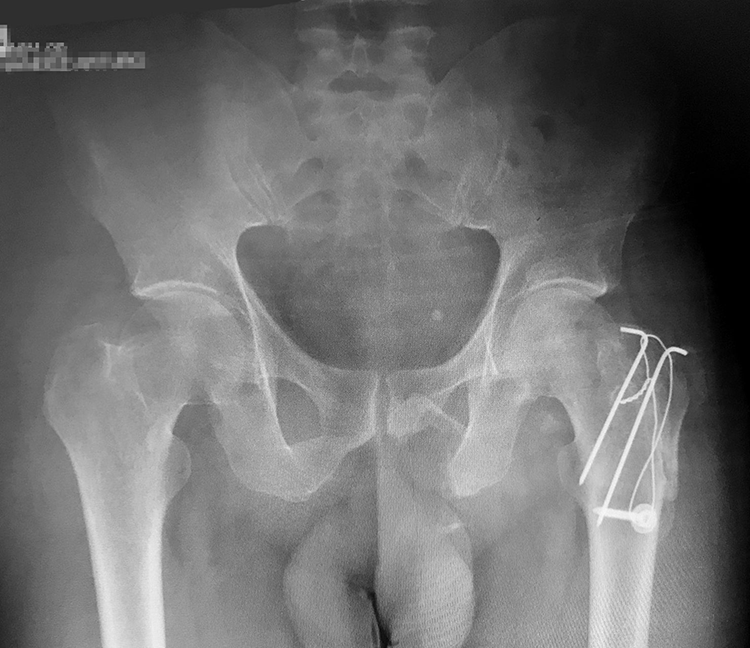
Radiograph at 6 months, showing complete healing of the greater trochanter fracture.
Radiograph at 12 months, without signs of avascular necrosis of the femoral head or post-traumatic osteoarthritis.
The functional evaluation was carried out using the Harris Hip Score 3,4 :37 points at 2 months and improved to 81.8 points at 6 months, and 1 year after surgery the score was 89.0 which means a good result. After 1 year of follow-up, the patient is asymptomatic, functional, there were not avascular necrosis, or arthrosis evidence at the X-Rays, and the Harris score was 89.0 (Figures 7 and 8).
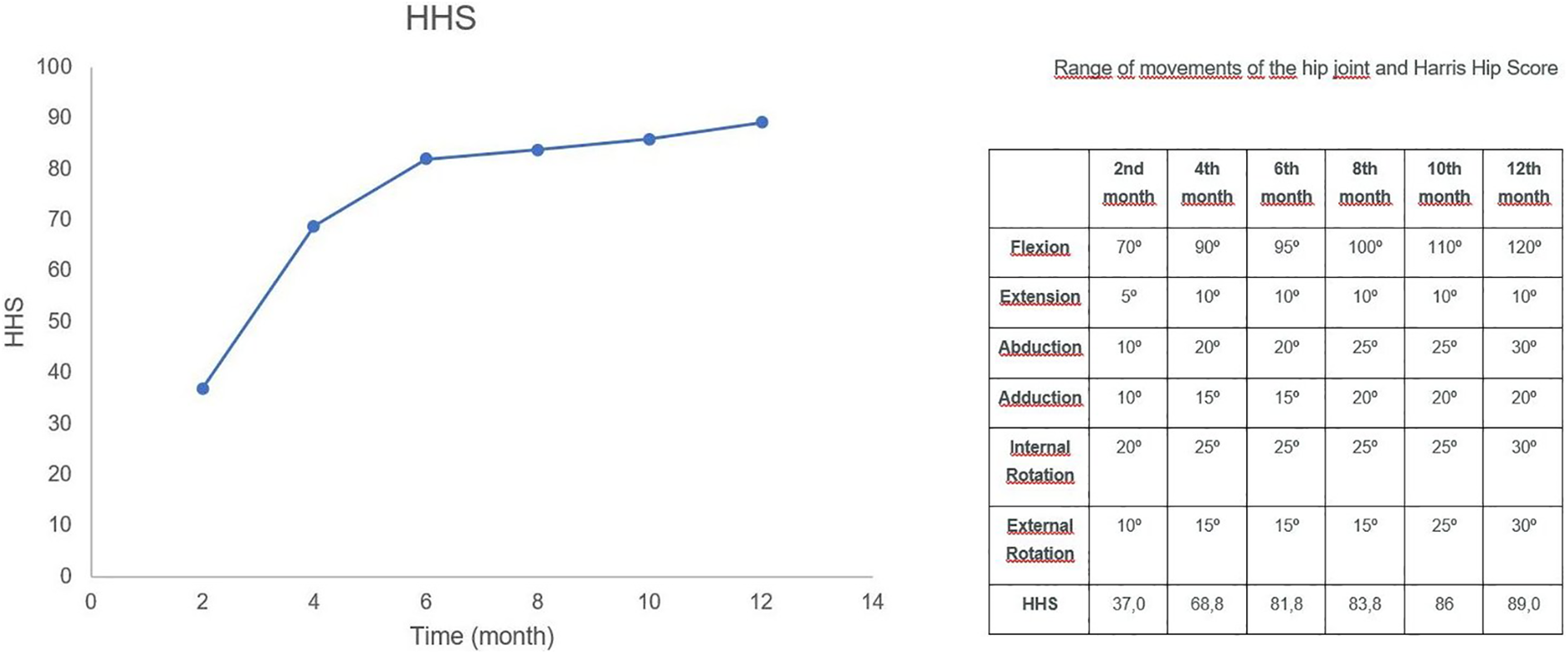
Harris Hip Score and hip range of motion over time.

Active range of motion at 12-month follow-up.
Discussion
Anterior hip dislocations usually result after a high-energy trauma, accounting for approximately 10% of hip dislocations, 5 the obturator type of hip dislocation results from forceful abduction and external rotation with the hip in flexion 6 ;in our case the trauma mechanism could have resulted from a forceful abduction and external rotation with the hip in flexion. The trochanter while abducting impinges upon the acetabulum rim, levering the femur head through the anterior capsule. We believe that this trochanteric impingement against the posterior acetabular wall may lead to the greater trochanter fracture; the residual impact finally might have caused an ischium fracture.
Maruoka et al. in 1993 7 reported a case of pubic-type dislocation of the hip combined with fracture of the ipsilateral greater trochanter managed with closed reduction and a hip spica cast for 6 weeks, and according to their cadaveric study there are two different patterns of impingement between femur and pelvis responsible for the greater trochanter fracture, the first consisted of impingement between the greater trochanter and the iliac bone, and the second of impingement between the femoral neck and the rim of the acetabulum.
Associated fractures to anterior hip dislocations are not common, combination between the anterior hip dislocation and ipsilateral intertrochanteric fracture was reported by Radulescu et al., 8 Chadha et al. 9 described a traumatic anterior dislocation of the hip joint with posterior acetabular wall fracture, El Masry 10 treated a 28-year-old male patient with a combined fracture neck femur with anterior dislocation of the head of the femur by open reduction and internal fixation.
Among the fractures associated with anterior dislocation of the hip, ipsilateral fractures of greater trochanter and the ischial tuberosity are even more rarely seen, and to our knowledge, there are no cases described in the literature. Reduction of the hip dislocation should be considered as an emergency due to the avascular necrosis risk. The healing of the greater trochanter fracture requires absolute stability, alternative of fixation includes cannulated screws and anatomical plates, we consider that a tension band is a biomechanically appropriate solution since it converts tensile forces to compression forces.
In 2018, Selvanayagam et al. 11 documented another case of traumatic pubic dislocation with greater trochanter fracture treated with a closed reduction of the dislocation and open reduction and fixation of the trochanter with two 6.5 mm partially threaded cannulated cancellous screws with an excellent outcome.
In 2019, Khalifa et al. 12 reported a case of a 13-year-old boy who had an open anterior dislocation of the hip with ipsilateral avulsion fracture of the greater trochanter, their treatment consisted of a complete debridement and hip reduction, but osteonecrosis was present at 3 years postoperative. A replacement hip prosthesis was placed when the patient was 18 years old.
Avascular necrosis of the femoral head is the most feared late complication of hip dislocation and reduction within 6 hours is recommended to minimize the risk, 13 there is a paucity of literature involving the long-term results in these patients and the incidences of avascular necrosis, Kellam et al. 14 reported for anterior dislocations, the event rate for avascular necrosis ranged from 0.087 to 0.333, whereas the event rate for post-traumatic osteoarthritis ranged from 0.125 to 0.700. In our case, there were no signs of avascular necrosis or post-traumatic osteoarthritis after 1 year of follow-up, however, more time is needed to establish definitive sequels.
Conclusions
This report presents a rare case of the obturator type of anterior dislocation of the hip with a fracture of the ischial tuberosity and the greater trochanter, describes the treatment and follow-up based on the X-Rays and the Harris Hip Score, tries to explain the mechanism of the injury and remarks the importance of an early reduction among the fixation of the greater trochanter fracture.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.