
Abstract
Keywords
Introduction
Scoliosis is defined as a lateral curvature of the spine, which influences its alignment in frontal, sagittal, and transverse planes.1,2 Scoliosis is divided into structural and nonstructural scoliosis (postural). 3 Structural scoliosis can be further divided into idiopathic (cause unknown) and nonidiopathic (cause known) scoliosis. The incidence of scoliosis varies between 2% and 13.6%.4,5 Some reasons, such as genetics, growth, hormonal dysfunction, bone mineral density change, abnormalities in body part tissue, abnormal platelet calmodulin levels, biomechanical factors, and central nervous system abnormalities influence the incidence of this disease. 6
Various treatment approaches are used for subjects with scoliosis. The use of various designs of braces, physical therapy, functional electrical stimulation, yoga, and surgery are the common methods for treating scoliosis.3,6 The braces used for idiopathic scoliosis can be divided into soft and rigid braces. Some braces such as Milwaukee, Boston, and Cheneau are classified as rigid braces, and employ three points pressure system to stabilize and correct the scoliosis curves. 6
One of the braces recommended for idiopathic scoliotic subjects is a soft brace. Actually, the use of soft braces to treat scoliosis has been described by Fisher based on the use of elastic straps to correct deformities associated with scoliosis.3,7 These elastic straps mostly apply corrective forces to inhibit curve progression. This was the first report on the use of soft braces for scoliotic subjects. During the 80th and early 90th other types of soft braces such as the St Etienne brace and Olympe were developed in France. 8 However, there was no study that evaluated the effectiveness of these braces. Other types of braces developed based on the physical therapy approach include SpineCor and Spinealite. 8 The main difference between the designs of SpineCor and Spinealite is related to the locations of the straps and the material used. A new type of soft brace was developed based on the previous designs of soft braces with an emphasis on the correction of lumbar lordosis. The new brace was named as Universal Spine orthosis. 8 Although the newly developed brace could be used for different purposes including scoliosis, it was not easy to be adjusted and the patients may experience some problems during daily activities including clothes change and toilet use. 8
Based on the results of various studies, the use of a brace influences the rate of curve progression and controls the severity of scoliosis.3,9 Rigid braces restrict the motions of the spine significantly and the performance of scoliotic subjects especially during sports activities.10–12 Moreover, the use of these braces influences the quality of life of scoliotic subjects. 13 As a result, some of the scoliotic subjects prefer to not use any braces or select other treatment approaches. 13 SpineCor brace is mostly recommended for the subjects who refused to use the rigid braces with a curve not exceeding 30–35°.7,14–16 SpineCor brace consists of corrective elastic bands attached to a pelvic base. These corrective bands apply various corrective forces based on the type and the location of the curve.14,17,18 Actually, it applies dynamic corrective forces to prevent curve progression. 16
Soft braces seem to have less motion restriction than rigid braces and do not influence the quality of life of scoliotic subjects as much as rigid braces.6,19 However, the main questions are how much is the amount of effectiveness of this brace (SpineCor) to prevent scoliotic curve progression in idiopathic scoliotic subjects and also are there any differences between the effectiveness of this brace compared to rigid braces? Therefore, this review aimed to evaluate the effectiveness of the SpineCor brace used for scoliotic curves and other available braces.
Method
Search strategy: A search was done in databases including PubMed, Google Scholar, ISI Web of Knowledge, Ebsco, Embasco and Scopus for a period up to December 2021. Keywords of soft braces, soft orthosis, and SpineCor were used in combination with scoliosis.
Exclusion and inclusion criteria
The first criterion to select the paper was based on titles and abstracts to focus on the use of soft braces for scoliosis. The papers which focus on other spinal deformities like lordosis, and kyphosis were ignored in this stage. The second criterion to select the papers was based on the papers which were published in the English language.
It should be emphasized that the outcome variables were not considered in the selection of the studies. The type of studies, type of participants and type of interventions were the other criteria to select the studies.
Type of studies
It was tried to select mostly randomized control trials however, due to the lack of these studies on this topic other types of studies were also included (case series, and case controls). Abstracts, conference articles, editorial comments, and expert opinions were excluded from the final list.
Type of participants
The studies focused on idiopathic scoliosis were selected in this study.
Type of interventions
The studies on the use of soft braces for idiopathic scoliosis curves were selected in this study.
Main outcomes
The main outcome measures selected in this study include X-ray measures (rib cage angle and Cobb angle), time of use of the brace and quality of life.
Secondary outcome
The need for surgery and other complications were selected as secondary outcomes.
Two researchers independently screened the studies based on the aforementioned criteria. It was done mostly based on titles and abstracts and then the full text of the studies. If there was a source of disagreement, a third reviewer was involved.
Data extraction and management
This review was done based on Population, Intervention, Comparison and Outcome (PICO) style. It means that the data of each study was categorized as PICO.
Quality assessment and determination of the risk of bias
The quality of the studies was evaluated based on Down and Black tool 20 (It was done by one reviewer). It is a reliable tool to evaluate the quality of the studies. It consists of four parts including internal validity, external validity, bias and confounding. Furthermore, it consists of 28 questions which evaluate various aspects of the studies. The trustworthiness and relevance of the published papers were determined based on this scale. A higher score on this scale represents better quality.
Results
Based on the aforementioned keywords 52 studies were achieved. After reviewing the title and abstract of each study, 11 papers were selected for final analysis. Eight studies were on the evaluation of the effectiveness of the SpineCor brace on scoliosis. In these studies, the effect of the SpineCor brace on scoliosis curve correction and its association with the severity of the curve, type of the curve (single or double curves) and gender were evaluated. There were three studies on the comparison of the SpineCor with other available rigid braces. In one of these studies, the effects of SpineCor on the kinematic of the knee joint were evaluated and compared with rigid TLSO. In another study, the effectiveness of SpineCor was compared with the Boston brace. The third study focused on the comparison between SpineCor and underarm rigid brace on spinal curves.
Table 1 shows the quality assessment results of the studies. As can be seen from this table, the quality of the studies scored between 11 and 19 (out of 28), based on the Down and Black scale.
The results of studies on effectiveness of SpineCor brace on scoliotic curve.
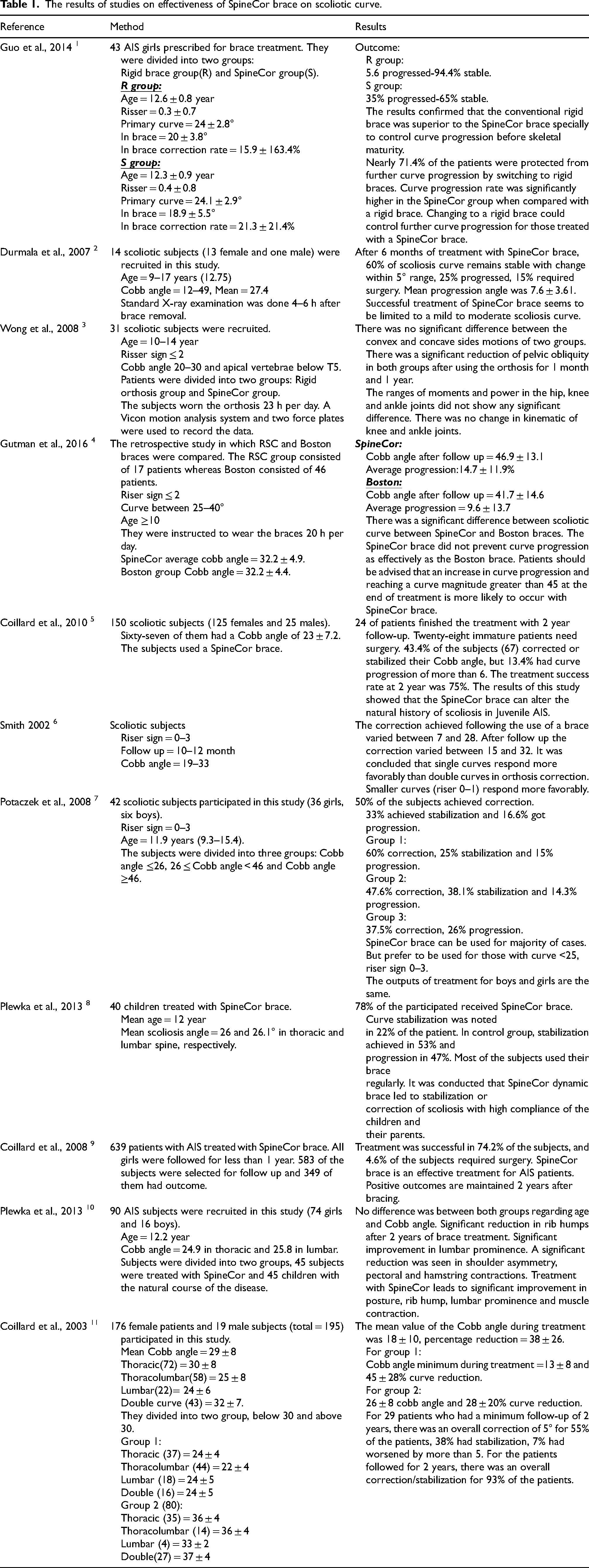
Table 1 show the results of selected studies on the effectiveness of the SpineCor brace. The main outputs of the selected studies include:
Use of SpineCor results in clinical improvement in posture, reduction in the hump, lumbar prominence and muscle contractures in the subjects with scoliosis.
21
The effectiveness of SpineCor for the curve below 30° was more than that with the curve above 30°.
22
Single curves respond more favorably than double curves.
23
Although the outputs of treatment with SpineCor were the same for both girls and boys, it is preferred to be used for the curve < 30° with Riser signs 0–3.
22
It seems that the effectiveness of SpineCor on shoulder asymmetry, pectoral and hamstring contracture is more than that on Cobb angle.
22
Use of SpineCor did not influence the kinematic of knee and ankle joints.
24
It seems that curve of scoliosis progressed more in the subjects who used SpineCor than those who used rigid braces. Therefore, successful treatment seems to be limited to mild to moderate scoliosis curves. Type of the curves and severity of the curves influence the output of treatment with SpineCor. Single curves respond more favorably than double curve to the use of a SpineCor brace. Moreover, the use of this brace influence shoulder asymmetry, muscle contraction and posture, as shown in Table 1.
Discussion
Soft braces (especially SpineCor brace) seem to restrict the performance of the scoliotic subjects less than that of rigid braces (Boston brace). However, the main question posted here is: Are soft braces as effective as rigid braces to control the scoliotic curve progression. Therefore, the aim of this review was to review the available studies to determine the effectiveness of soft braces (Table 2).
The results of quality assessment of studies selected in this review.
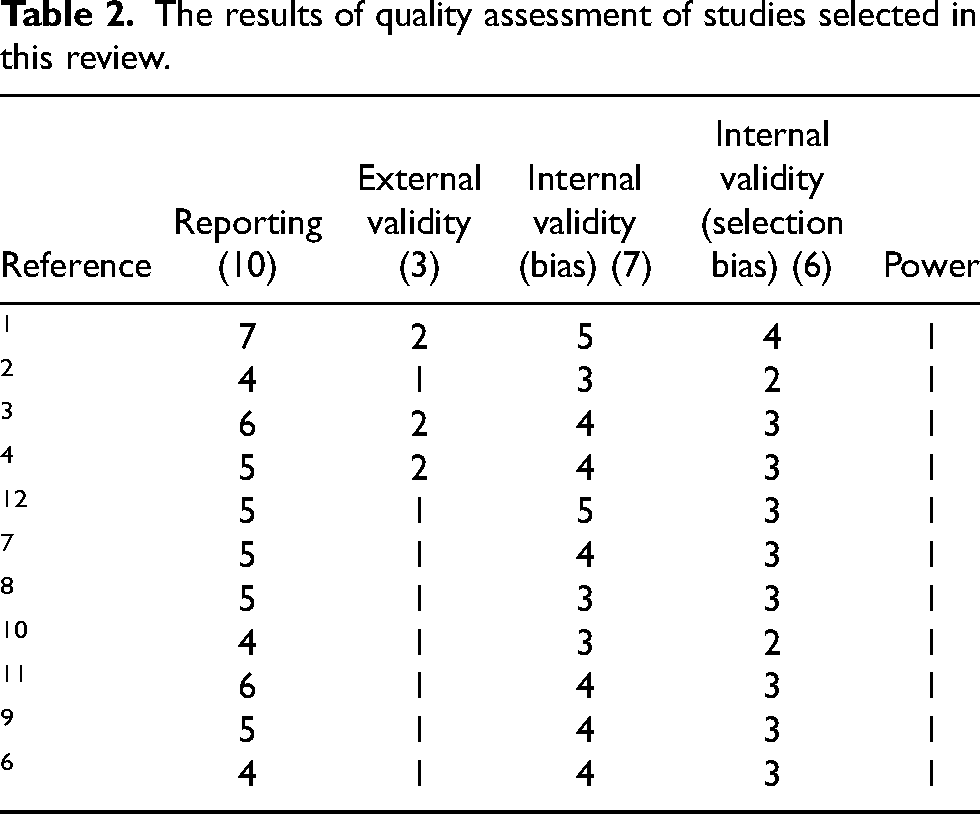
There were 11 studies on this topic of which eight papers focus on the effectiveness of soft braces and three studies on the comparison between soft and rigid braces and only observation. The quality of these studies varied between 11 and 19 (the total score of quality based on this score is 28). The quality of most of these studies was medium (between 11 and 19) due to a low number of participants, short follow-up time, and also no attempt was done to blind the researchers and patients regarding the type of braces. In the research done by Plewka et al. on 90 scoliotic subjects, the progression of the scoliotic curve was followed for 2 years and compared with those who received no treatment (only observation).12,21 The success rate for the scoliotic group was 22% compared to 53% in the observation group (the scoliosis curve was 26° in the SpineCor group). The results of this study also showed that the use of a SpineCor brace influenced posture, shoulder hump, lumbar prominence and muscles contractures. 21 In another study done by Coillard et al. on 39 scoliotic subjects, it was shown that 93% of the subjects got some degrees of scoliotic curve correction and stabilization. 16 The results of other studies on the effectiveness of SpineCor brace confirmed that SpineCor brace can alter the natural history of scoliosis 17 led to stabilization or correction of scoliosis with a high degree of acceptance by children and their parents21,25 and also could influence the asymmetry of shoulder and rib hump in these subjects. It should be emphasized that the number of subjects in these studies was noticeable, and the subjects were followed up for at least 2 years. Therefore, based on the above-mentioned studies and due to the quality of the studies it can be concluded that the SpineCor brace seems to control the progression of the scoliotic curve. However, it should be noted that the effectiveness of the SpineCor brace depends on curve severity, and the type of the curve (double or single). In the research done by Coillard et al., 176 scoliotic subjects, treated with SpineCor, were divided into two groups, those with the curve above 30° and those with the curve below 30°. The results of their research confirmed that the curve correction in those with curve less than 30° were more than those with curve more than 30° (mean Cobb angles were 29 ± 8 and 18 ± 10°, before and after treatment, respectively). 16 In another study done by Smith it was concluded that single curve responded more favorably than double curve, especially for those with Risser signs 0–1. 23 Potaczek et al. also showed that although SpineCor brace can be used for most of the scoliotic subjects, it is preferred to be used for those with curve < 30° and with Riser signs 0–3. 22 Based on the above-mentioned studies and due to the quality of the available studies, it can be concluded that SpineCor brace has better effectiveness for younger scoliotic subjects (riser sign < 3). It is preferred to be used for the curve less than 30°.
The second question posted here is that whether the effectiveness of the SpineCor brace is comparable with other available rigid braces or not. There were three studies on this topic. The quality of these studies varied between 15 and 19. In the study done by Wong et al. on 31 scoliotic subjects (with Cobb angle between 20° and 30° and apical of the curves below T5), the subjects were divided into two groups, those used SpineCor brace and those used rigid braces. 24 The results of their study showed that although both braces reduced pelvic obliquity significantly, they did not influence on power and moments of hip, knee and ankle joints while walking. The effectiveness of Boston brace was compared with SpineCor by Gutman et al. 26 Ninety-seven subjects used the SpineCor brace (Cobb angle was 32.2 ± 4.9°), whereas the Boston brace group consisted of 146 patients (Cobb angle was 32.2 ± 4.4°). Although there was no significant difference between scoliotic curve severities between both groups at the beginning of treatment, the scoliotic curve progressed significantly in the SpineCor group compared to the Boston group. They concluded that the patients should be advised that the risk of progression in the curve more than 45° is more likely to occur with the SpineCor brace. 26 In another study done by Guo et al., the effects of using a rigid brace were compared with the SpineCor brace (the severity of scoliotic curve was 24° in both groups). The scoliotic curve was stable in 94.4% of the subjects treated with a rigid brace, compared to 65% in the SpineCor group. It was concluded that a rigid brace was superior to SpineCor to control the progression of scoliosis before skeletal maturity. Moreover, 71.4% of those who used SpineCor were advised to use a rigid brace to control the curve progression. 27 Based on the above-mentioned studies and due to the quality of the studies, it can be concluded that the effectiveness of the SpineCor brace is not comparable with rigid braces. It should be also noted that the comparison between SpineCor and rigid braces is mostly done based on Boston brace. However, it seems that the effectiveness of other rigid braces such as Cheneau brace, ART brace, is more than that of the Boston brace, especially for the curves more than 40°. Therefore, it is recommended that the effectiveness of soft braces will be compared with new developed rigid brace in future research study.
As can be seen from above-mentioned studies, the main parameter evaluated in most of the studies was the Cobb angle. However, other parameters such as the effects of brace on quality of life, symmetry of pelvis and trunk, motions of other joints and compliance of the children and their parents are important.21–23,25 The effect of SpineCor on the reduction of pelvic obliquity was the same as rigid braces. 23 Although, there was no difference between the effects of SpineCor brace on scoliotic curves between boys and girls, 23 its effectiveness depends on curve severity and age of the subjects. It should be emphasized that significant reduction in shoulder asymmetry, correction of hamstring and pectoralis, improvement in posture and reduction in muscle correction occur following the use of this brace.21,25
Based on the above-reviewed studies and due to their quality, it can be concluded that the SpineCor brace could be used to control the progression of the scoliotic curve for the subjects with curve severity less than 30° and with riser signs 0–3. It should be emphasized that scoliotic subjects should be advised to use rigid braces as the first and most effective choice to control the progression of the scoliotic curve. If the patients refused to use rigid braces due to restriction and their effects on quality of life, the SpineCor brace should be an effective alternative.
There are some limitations which should be acknowledged regarding available studies, which include:
Limited follow-up period for scoliotic subjects used soft braces. Comparison of soft braces was done only with a few rigid braces. Limited number of scoliotic subjects in different studies. Limited number of parameters were evaluated (most of the studies only evaluated the severity of the scoliosis).
Conclusion
Based on the available literature and due to the quality of the studies, it can be concluded that the SpineCor brace can be used to control the progression of scoliosis. However, its effectiveness is limited to the curve with a severity of less than 30° and for the patients with Risser sign 0–3. The effectiveness of SpineCor is not comparable with rigid brace, especially for the curve above 40°.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.