
Abstract
Introduction
Appropriate placement of components in total knee arthroplasty (TKA) is important for long-term postoperative survival.1,2 Bone cuts of the tibia were performed using an intramedullary or an extramedullary guide.3,4 Although some reports suggest that the intramedullary guide has a higher accuracy,5–7 Phillips et al. 8 reported that 76% of surgeons prefer the extramedullary guide. When using an extramedullary technique on the tibial side, the intercondylar eminence,9,10 medial border of the tibial tubercle, 11 extensor hallucis longus,12,13 second metatarsal bone axis, 14 and the line connecting the medial and lateral malleolus of the ankle5,6 have been used as references, but no clear criteria have been established. The usefulness of computer-assisted measurements15,16 and robotic systems17,18 has also been reported, but they are not widely used because of cost issues.
In this study, we investigated whether the anterior border of the tibia is parallel to the tibial axis as determined by palpation, and which position of the anterior border should be used as a landmark of the tibial axis for the intramedullary guide system in TKA.
Materials and methods
This study was approved by the ethics committee of our institution (no. 2020017). Informed consent was obtained from every patient. From October 2014 to October 2018, 91 patients with osteoarthritis (OA) and varus deformity prior to TKA were evaluated for inclusion in this study. We excluded patients with valgus deformity, osteonecrosis, and rheumatoid arthritis.
Preoperatively, electrocardiogram (ECG) electrodes (CLEARODE, FUKUDA DENSHI, Tokyo, Japan) were placed along the anterior border at 5 cm (A), 10 cm (B), and 15 cm (C) distal to the tibial tuberosity, and an anteroposterior X-ray image of the tibia was taken (Figure 1). The angles of the AC, AB, and BC lines on the tibial bone axis line on XP were measured. The proximal side of each line was considered “minus” when it tilted toward the medial side of the tibia (varus) and “plus” when it tilted toward the lateral side of the tibia (valgus) (Figure 2).
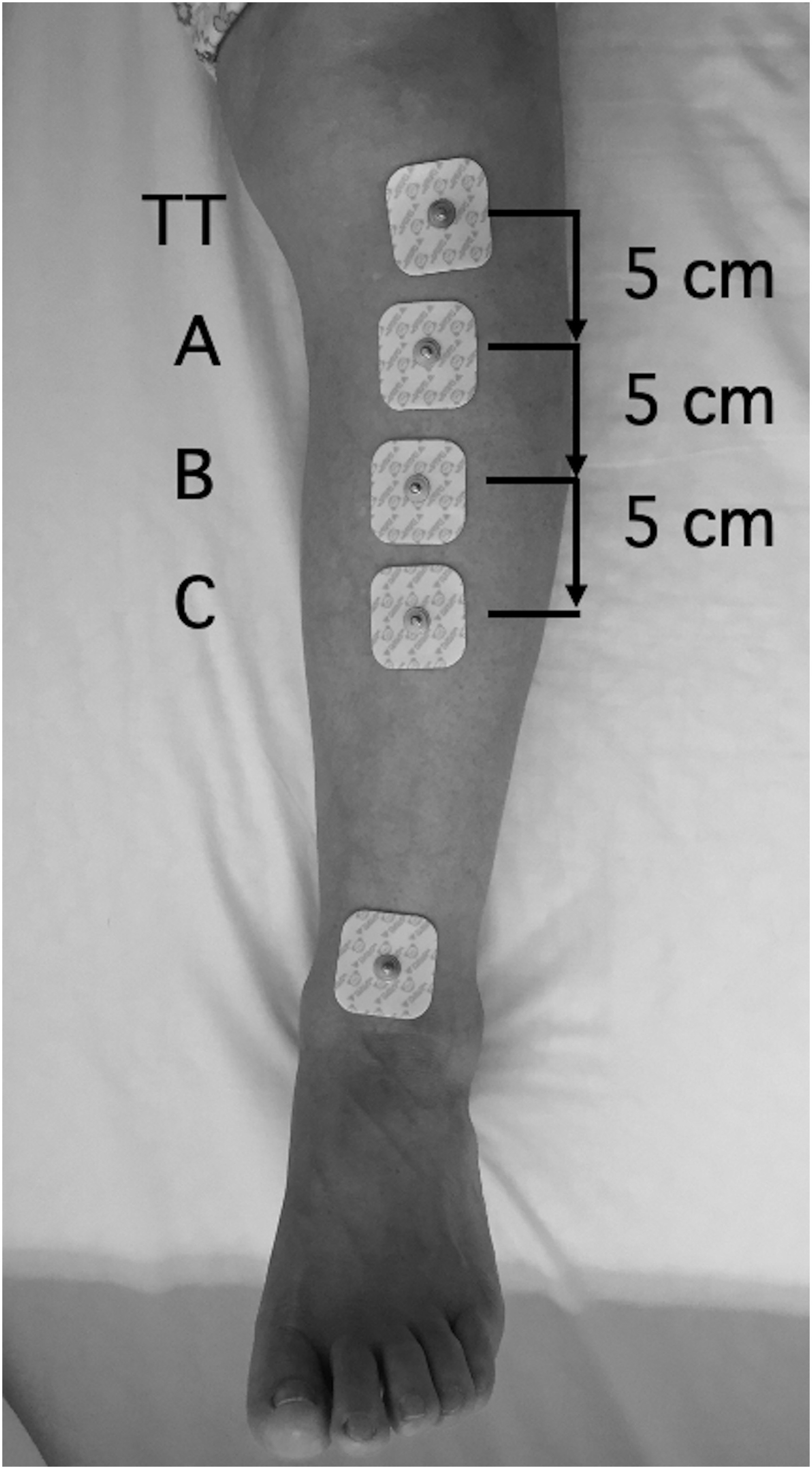
ECG electrodes were placed along the anterior border at 5 cm (a), 10 cm (b), and 15 cm (c) distal to the TT, and an anteroposterior X-ray image of the tibia was taken (an electrode on the ankle was not used in this study).
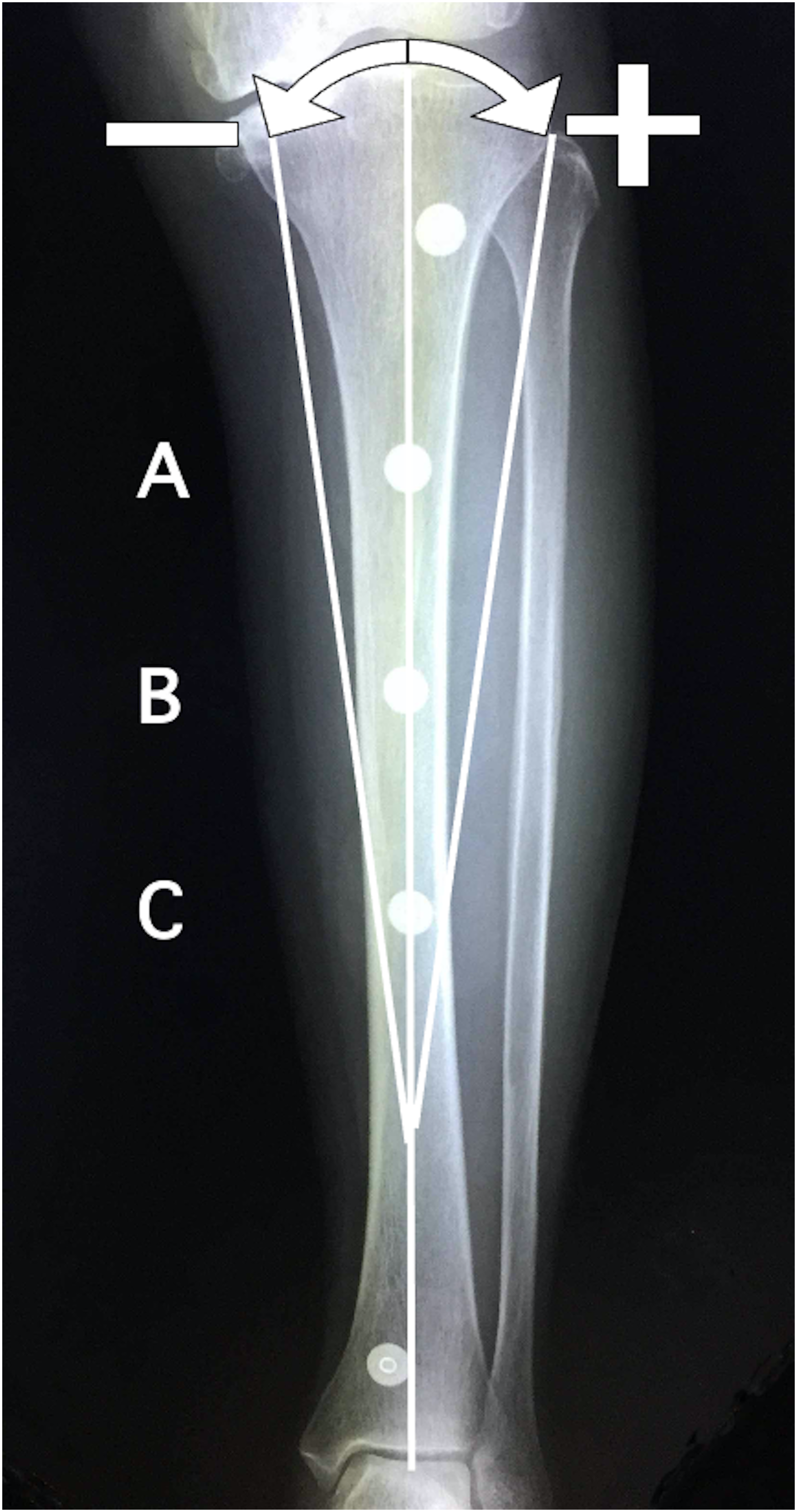
The angles of the AC, AB, and BC lines on the tibial bone axis line on XP were measured. The proximal side of each line was considered “minus” when it tilted toward the medial side of the tibia (varus) and “plus” when it tilted toward the lateral side of the tibia (valgus) (an electrode on the ankle was not used in this study).
To assess intraobserver and interobserver reliabilities, intraclass and interclass correlation coefficients of the angles of the AC lines to the tibial bone axis were calculated using the JMP software (version 16.0.0; SAS Institute NC). The intraclass correlation coefficient was calculated from the data measured by one observer (S-GK). The interclass correlation coefficient was determined from independent measurements of the two observers (S-GK and HA).
Results
The test group of patients comprised 10 men and 81 women, aged 58–89 years (mean, 76.3), with an average height of 151.3 cm, an average weight of 59.1 kg, and an average BMI of 25.8 kg/m2 (range, 15.8–37.6). According to the Kellgren-Lawrence (KL) classification, 20 patients had grade III (moderate) OA and 71 patients had grade IV (severe) OA.
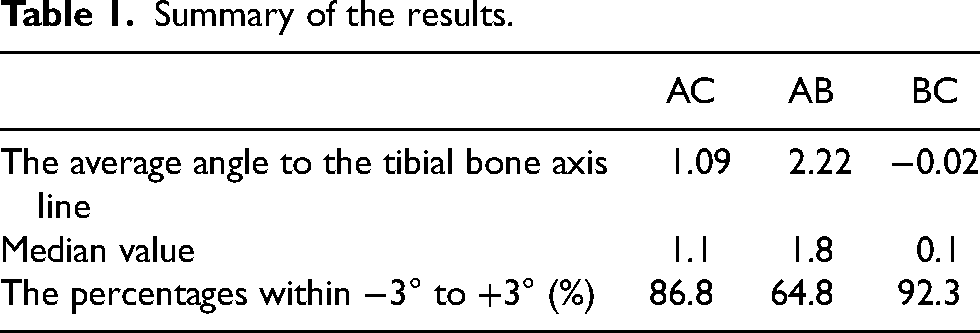
The mean angles of the AC, AB, and BC lines to the tibial bone axis line were, respectively, 1.09 ± 1.75, 2.22 ± 2.64, and −0.02 ± 1.91 (mean ± SD). The median values were 1.1, 1.8, and 0.1, and the percentages within −3° to +3° were 86.8, 64.8, and 92.3, respectively (Figure 3 and Table 1). The mean angles of BC lines to the tibial bone axis line were −0.07 ± 1.99 in KL grade III and 0.00 ± 1.91 in grade IV. The intraclass correlation coefficient was 0.97 and the interclass correlation coefficient was 0.91.
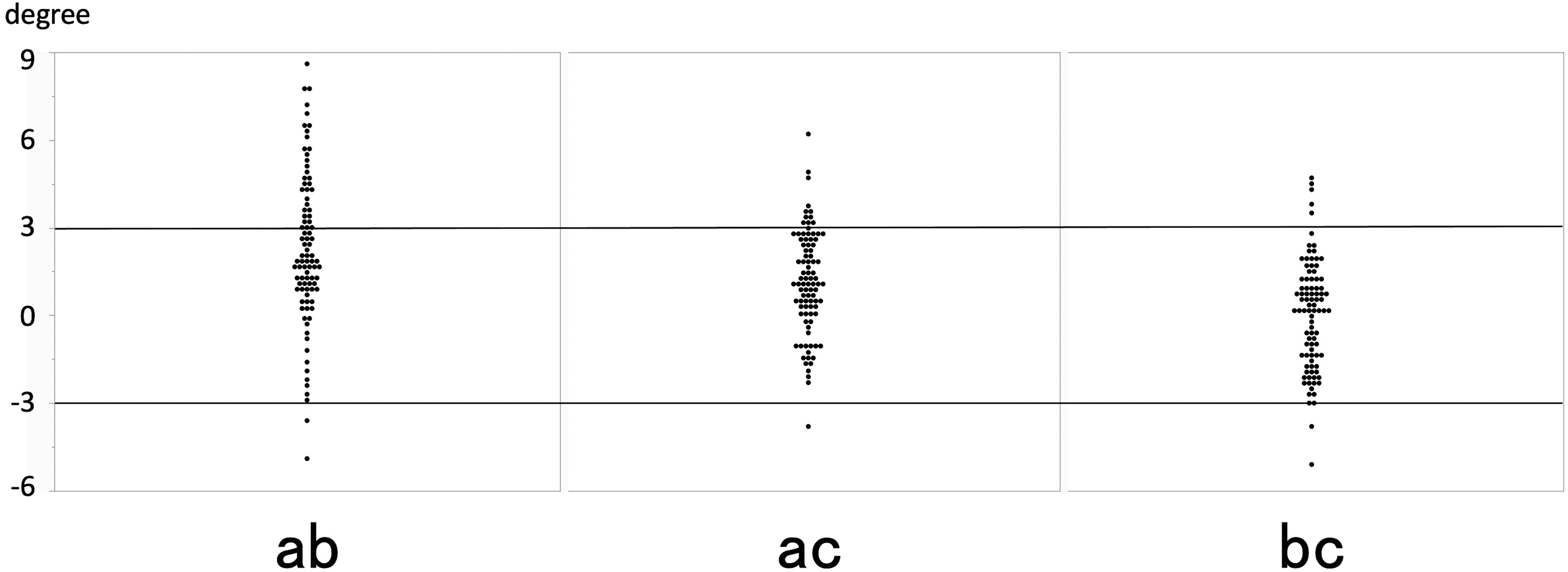
The mean angles of the AC, AB, and BC lines to the tibial bone axis line were 1.09 ± 1.75, 2.22 ± 2.64, and −0.02 ± 1.91 (mean ± SD). The percentages within −3° to +3° were 86.8, 64.8, and 92.3, respectively.
Summary of the results.
Discussion
In TKA, the surgeon aims to place the tibial component perpendicular to the functional axis of the tibia. Although some reports recommend anatomical alignment,19,20 identification of the functional axis during surgery is important because the osteotomy angle is determined based on a line 90° to the functional axis.
For tibial bowing, extramedullary guides are preferred over intramedullary guides. However, the placement of the extramedullary guide is also subject to error because the reference point is subjective and soft tissues may be obstructive. We believe that a simpler and a more accurate reference line can be identified. The tibial anterior border can be easily palpated and can serve as an objective reference point. The anterior border extends from the tuberosity to the anterior margin of the medial malleolus. The line of the anterior border is not parallel to the tibial axis. This study showed that the line connecting the points 10–15 cm distal to the tibial tuberosity averaged −0.02° to the tibial axis and was almost parallel to the functional axis of the tibia. The results were not affected by KL classification. In addition, 92.3% of the points were located within −3° to +3° of the tibial axis, suggesting that they could be used as reference lines for extramedullary guides. The line connecting the points 5–10 cm distal to the tibial tuberosity showed an average eversion of 2.22°, and only about 65% of the points were between −3° and +3°, suggesting that the anterior border within 10 cm of the tibial tuberosity should not be used as a reference line.
Computed tomography (CT)-based studies21,22 have reported that the tibial anterior border is an indicator of the tibial axis. However, in actual surgery, the tibial anterior border cannot be seen directly and must be confirmed by palpation. In this study, we investigated whether the tibial anterior border is parallel to the tibial axis as determined by palpation, and which position of the tibial anterior border should be used as an indicator of the tibial axis. Drawing a line connecting two points, one 10 cm and the other 15 cm distal to the tibial tuberosity on the tibial anterior border is simple, easy, and useful as a reference line for extramedullary guidance.
This study had some acknowledged limitations. First, the tibial tuberosity is not a pinpoint; therefore, there may be a discrepancy in the measurements. Second, in patients with thick subcutaneous fat, the tibial tuberosity and anterior border may be difficult to confirm. Furthermore, if the frontal view of the lower leg is not accurate at the time of radiographic imaging, the line of the anterior tibial border may be skewed. Therefore, because the measurements in this study varied from case to case, and it should only be considered as one indicator. Finally, only Japanese patients with varus OA were included in this study, so it is unknown whether this study is applicable to valgus OA or non-Japanese patients. Further investigation is needed to address these limitations.
Conclusion
A line connecting two points, one 10 cm and the other 15 cm distal to the tibial tuberosity, is approximately parallel to the tibial axis and can serve as a reference line for the extramedullary alignment technique in TKA.
Footnotes
Acknowledgements
We would like to thank Editage (www.editage.com) and WORDVICE (![]() ) for English language editing.
) for English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.