
Abstract
Purpose
The purpose of this meta-analysis was to compare the efficacy and imaging parameters of kinematic alignment (KA) and mechanical alignment (MA) in total knee arthroplasty (TKA) and to evaluate whether patients undergoing KA-TKA benefited more than those undergoing MA-TKA.
Methods
Studies comparing the efficacy of KA-TKA and MA-TKA were included after searching and screening in the database, including PubMed, Embase, Web of Science and Cochrane Database Library. A total of 1420 patients were enrolled in the study, with 736 MA-TKA and 738 KA-TKA. The primary outcomes were postoperative knee function scores including KSS series, WOMAC, KOOS and OKS. Secondary outcomes included the operative time, the length of hospital stay, knee extension/flexion angle, and some imaging parameters. The risk of bias for included studies was assessed using the Cochrane Collaborative risk-of-bias assessment tool or the Newcastle-Ottawa Scale(NOS).
Results
Sixteen studies were included in this meta-analysis (11 randomized controlled studies and 5 cohort studies). Primary outcomes: Knee Society score (KSS, MD = 8.36, 95% Cl: 0.83–15.90) and combined KSS (MD = 15.24, 95% CI: 5.41–25.07) were higher in KA-TKA than in MA-TKA, and other functional scores were not statistically significant in KA-TKA and MA-TKA, including knee injury and osteoarthritis outcome score (KOOS), Oxford knee score (OKS), Knee Function score (KFS) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Secondary outcomes: KA-TKA resulted in smaller medial proximal tibial angle (MPTA) and lateral distal femoral angle (LDFA) compared to MA-TKA. For other outcome measures, KA-TKA showed similar results compared to MA-TKA, including hip-knee-ankle (HKA) angle, extension/flexion angle, tibial component slope angle, joint line orientation angle (JLOA), the operation time, the length of hospital stay and ligament release rate.
Conclusions
In our analysis results, patients undergoing KA-TKA benefit as much as patients undergoing MA-TKA. KA may be a viable reference in total knee replacement.
Introduction
Accurate alignment at implantation is important in total knee arthroplasty (TKA). The classical mechanical alignment (MA) technique is designed to create the neutral axis of the hip - knee - ankle on a two-dimensional plane, and has been used for more than 30 years. 1 The main points of MA-TKA are as follows: (1) Make the femur and tibia components perpendicular to their respective mechanical axes; (2) Adjust the internal and external rotation angle of the femoral and tibial components to create a parallel extension-flexion gap to place the knee prosthesis; (3) When necessary, release the medial or lateral collateral ligaments to restore the medial and lateral tension balance of the knee. 2 Theoretically, this approach can balance the internal and external forces of the knee compartment, reduce the wear of the prosthesis and improve the survival rate of the prosthesis. And many studies have shown that the survival rate of knee prostheses can exceed 90% after 15 years. 3 The chief complaint of patients was usually stiffness and tightness of the knee after surgery. 4 The possible reason is that the normal motion pattern or the kinetic characteristics of the pre-arthritic state of the knee were not recreated well. 5 Bellemans et al. showed that the alignment of the lower limb in most people was not neutral, but a slight varus. 6 MA-TKA only simulates the motion pattern of the knee joint from a two-dimensional plane, without restoring the physiological characteristics of the knee.
With the development of knee biomechanics, the concept of kinematic alignment (KA) in total knee arthroplasty was proposed to reconstruct the three axes of knee motion, thereby restoring physiological kinematic of the knee. One is the transverse axis of the femur around which the tibia flexes and extends, one is the longitudinal axis of the rotation of the tibia, and the last one is the transverse axis of the patella that is the extension and flexion axis of the patella.5,7 Some studies have shown that KA-TKA may be better than MA-TKA in improving the early postoperative knee function, range of knee motion and patient satisfaction.8,9 while other studies reported that KA-TKA did not show superiority compared with MA-TKA in postoperative efficacy. and more outliers with poor results were found in KA-TKA group.10–12 In response to this controversy, several recently published meta-analysis have yet to reach a unified conclusion, and most of them aim to compare the short-term efficacy of two alignment approaches.13,14 Therefore, it remains unclear which technique has more advantages.
The aim of this study was to perform an up-to-date meta-analysis comparing the efficacy of KA-TKA versus MA-TKA in knee function score and imaging parameters after operation.
Materials and methods
A total of 1420 patients were enrolled in the study, with 736 MA-TKA and 738 KA-TKA. The meta-analysis was conducted according to Cochrane Collaboration standard. Ethical approval was not required for this study as it did not involve the possibility of potential harm to participants.
Search strategy
The initial literature search was conducted independently by two researchers using data including PubMed, Embase, Web of Science and Cochrane Database Library. The search terms utilized in the title, abstract, and MeSH were listed as follows: (kinematic OR kinematical OR kinematically) AND (mechanic OR mechanical OR mechanically) AND (total knee replacement OR total knee arthroplasty OR TKA OR TKR). mechanical OR mechanically) AND (alignment OR aligned). Literature was retrieved with publication dates up to 1 March 2021, but without restricting the region and language. Initially, literature screening is carried out by reading the title or abstract. For studies that were unsure whether they meet the inclusion criteria, the entire article will be carefully read. When there was a disagreement, a third researcher would join in the discussion.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) All randomized controlled trials and cohort studies comparing the efficacy of KA and MA in TKA. (2) Postoperative follow-up in these studies was longer than 12 months. (3) Outcome measures during follow-up included but were not limited to postoperative knee functional scores or imaging parameters. Criteria for exclusion: (1) patients with previous history of knee surgery or trauma. (2) Case reports, basic research, and cadaver studies. (3) Outcome measures cannot be analyzed uniformly with other studies or studies with incomplete data.
Data extraction
The task of data extraction was performed independently by two authors when the study was identified for inclusion. The information extracted from each study included the year of publication, time of follow-up, study design, sample size, mean age, sex ratio, type of prosthesis, operative method, and outcome measures. After that, these data will be summarized in a table. If a dispute occurred during this process, the third author would participate in the resolution of the issue. In our study, the primary outcome measures included KSS series, WOMAC, KOOS and OKS, and the secondary outcome measures included operative time, knee extension and flexion angle, and some imaging parameters.
We would extract the most recent data if an institution republishes the study by increasing the length of follow-up. If some outcome measures were only reported in previous studies, we would include them in our statistical analysis.
Methodological assessment
Two of us independently evaluated the methodological quality of the included randomized controlled studies and cohort studies using the Cochrane Collaborative risk-of-bias assessment tool and the Newcastle-Ottawa Scale(NOS), respectively. The Cochrane Collaboration risk-of-bias assessment criteria include: Is the random allocation sequence correct? Is the allocation plan hiding and blinding perfect? Is the result data complete? Is there a prompt for non-selective report results? Are there other risks of bias? The NOS evaluation criteria include the risk assessment of bias in three items: selection of study subjects, comparability between groups, and outcome measurement. The total score is 9, with 0–4 rated as low quality research and 5–9 rated as high quality research.
Statistical analysis
The collected literature data was analyzed using RevMan 5.3 software provided by the Cochrane Collaboration. The mean difference (MD) and relative risk (RR), with 95% confidence intervals (CIS) were used as combined statistics for continuous and dichotomous variables, respectively, for statistical evaluation. When I2 is less than or equal to 50%, heterogeneity is acceptable, and the fixed effect model is used for data analysis. When I2 is greater than 50%, it indicates greater heterogeneity, and sensitivity analysis random effects model are performed. p < .05 indicated a statistically significant difference.
Results
Literature search results
After the literature screening was completed according to our inclusion and exclusion criteria, 16 studies were finally included in our research, including 11 randomized controlled studies and 5 cohort studies. The retrieval process is shown in Figure 1. All the basic information extracted from the included studies are aggregated in Table 1. One of the studies was republished by increasing the length of follow-up. We included all of them in our study because some outcome measures had only been reported in previous studies. Flow chart of eligibility selection. Main characteristics of included studies. PRCT: prospective randomized controlled trial; PCS: prospective cohort study; RCS: retrospective cohort study; KA: kinematic alignment; MA: mechanical alignment; NR: not reported; PSI: Patient-specific instrumentation; CI: conventional instruments; CR: cruciate retaining; PS: posterior stabilize; RA: Robotic-assisted, ①WOMAC,②KSS/KFS/CKSS,③OKS,④KOOS,⑤HKA angle,⑥LDFA⑦MPTA,⑧complication,⑨Ligament release,⑩Extension range, ⑪Operative time, ⑫Flexion range, ⑬Length of hospital stay, ⑭Tibial component slope angle.

Quality assessment and publication bias assessment
The 11 included randomized controlled studies that had a low risk of bias according to the entries listed in Figure 2. According to the NOS scale, all the 5 cohort studies had a score greater than or equal to 5, which was considered to be of high quality. The funnel plot in Figure 3 indicated a low publication bias. Risk-of Bias summary of 11 studies. The funnel plot indicated a low publication bias.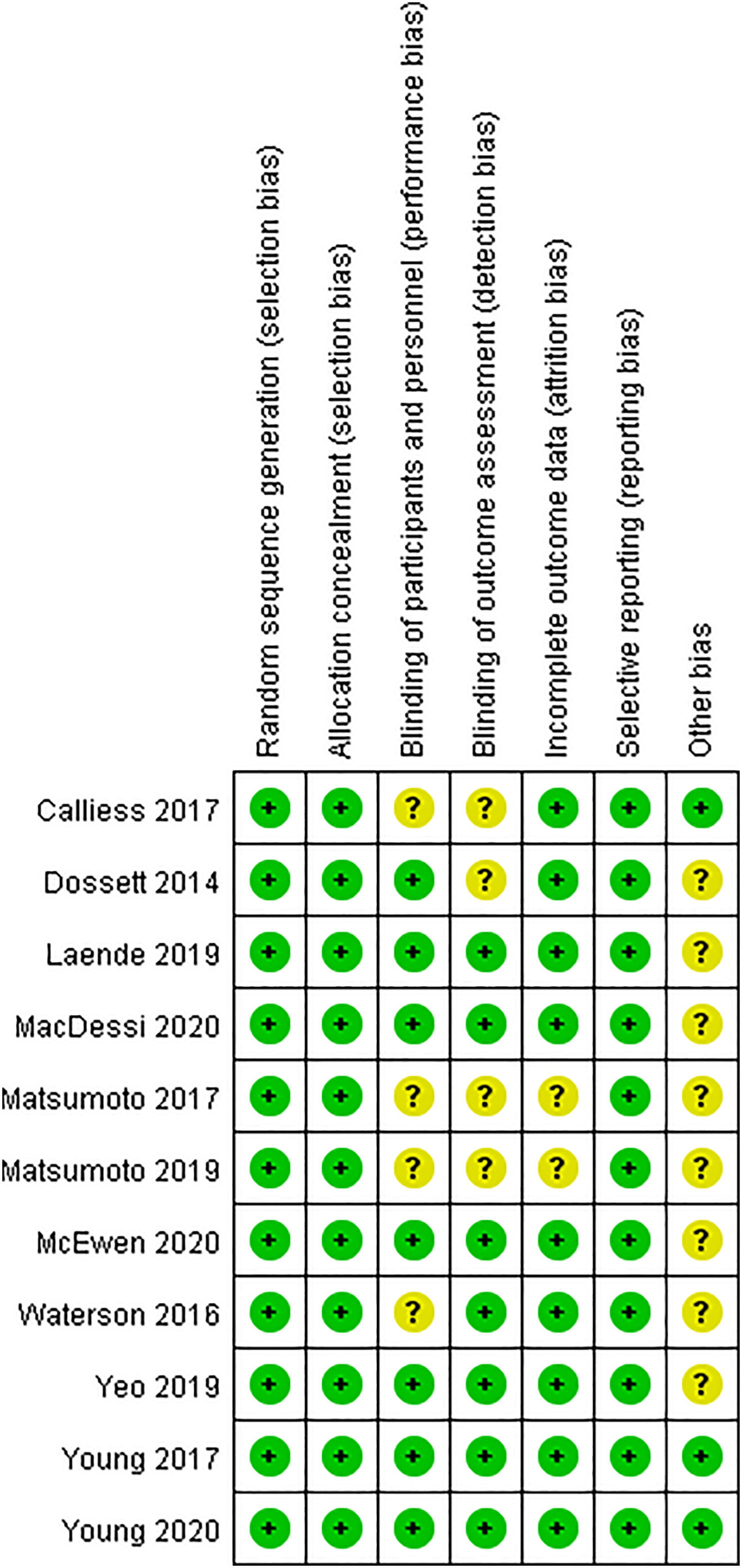

Subjective assessment of symptoms and functional outcomes
Four studies compared WOMAC of KA-TKA and MA-TKA, with a total of 447 patients (223 patients undergoing KA-TKA and 224 patients undergoing MA-TKA). Heterogeneity test result showed that there was significant heterogeneity among the studies (I2 = 92%). We noted that one of the studies had shorter follow-up times than the others,
12
and heterogeneity was significantly reduced after the exclusion of this study (I2 = 58%). The random effects model was applied in the statistical analysis. The result of meta-analysis showed that WOMAC had no statistical difference between KA-TKA and MA-TKA (MD = −3.22, 95% CI:-7.76 to 1.31, p = .16, Figure 4). The forest plot assessing western ontario and mcmaster universities osteoarthritis index between two alignment techniques.
Data on combined KSS were available in two studies, with 144 patients in KA-TKA and 144 patients in MA-TKA. The pooled MD was 15.24 (95% CI: 5.41 to 25.07, p < .1, I2 = 49%), indicating a better combined KSS in KA-TKA than in the MA -TKA. Similarly, two trials with a total of 159 patients reported complete data on KSS and the result showed the KSS in KA-TKA is better than that in MA-TKA (MD = 8.36, 95% Cl: 0.83 to 15.90, p = .03, I2 = 38%, Figure 5). For KFS, seven studies reported detailed data (MD = 2.02, 95% Cl: −2.83 to 6.87, p = .41, I2 = 71%, Figure 5), which were analyzed in two subgroups based on the length of follow-up. One group included 5 studies with 436 patients followed up for 12°months or less, and the other group included 2 studies with 155 patients followed up for 24°months or more. The pooled MD of the two subgroups were 4.94 (95% Cl: −1.17 to 11.05, p=0.11, I2 = 69%, Figure 5) and −3.82 (95% Cl: −7.89 to 0.25, p = .07, I2 = 0%, Figure 5), indicating that MA-TKA group and KA-TKA group had similar results. Since the heterogeneity of some sub-outcome indicators was greater than 50%, the random effects model was used in the above analysis. The forest plot for KSS series. The difference of KSS and combined KSS was significant in favor of kinematic alignment-total knee arthroplasty. KSS = knee Society score.
Four studies with 327 patients provided detailed data on KOOS, and the analysis showed that the score was not statistically significant between the KM-TKA and MA-TKA (MD: 2.81, 95%CI: −0.67 to 6.30, p = .11, I2 = 13%, Figure 6). Two of the studies reported the subgroup score of KOOS. Meta-analysis results showed that there was no significant difference between the two alignments, and the corresponding result of each subgroup was shown as follows: KOOS pain (MD = 1.34, 95%CI: −2.66 to 5.35); KOOS symptoms (MD = 1.58, 95%CI: −1.97 to 5.12); KOOS ADL (MD = .52, 95%CI: −2.38 to 3.43); KOOS sports (MD = 2.71, 95%CI: −4.45 to 9.87); KOOS QoL (MD = 1.91, 95%CI: −2.76–6.58). The heterogeneity between the above studies was small, so the fixed-effect model was used in the analysis. The forest plot assessing knee injury and osteoarthritis outcome score between kinematic alignment-total knee arthroplasty and mechanical alignment-total knee arthroplasty.
A total of 578 patients were evaluated by OKS in six studies, including 290 patients who underwent KA-TKA and 288 patients who underwent MA-TKA. The meta-analysis result showed that no significant difference was demonstrated by the pooled data between the two alignments(MD = 1.35, 95%CI: −0.04 to 2.74, p = .06), and showed a slightly higher degree of heterogeneity between the studies (I2 = 52%, Figure 7), hence the random-effects model used. The forest plot assessing oxford knee score between kinematic alignment-total knee arthroplasty and mechanical alignment-total knee arthroplasty.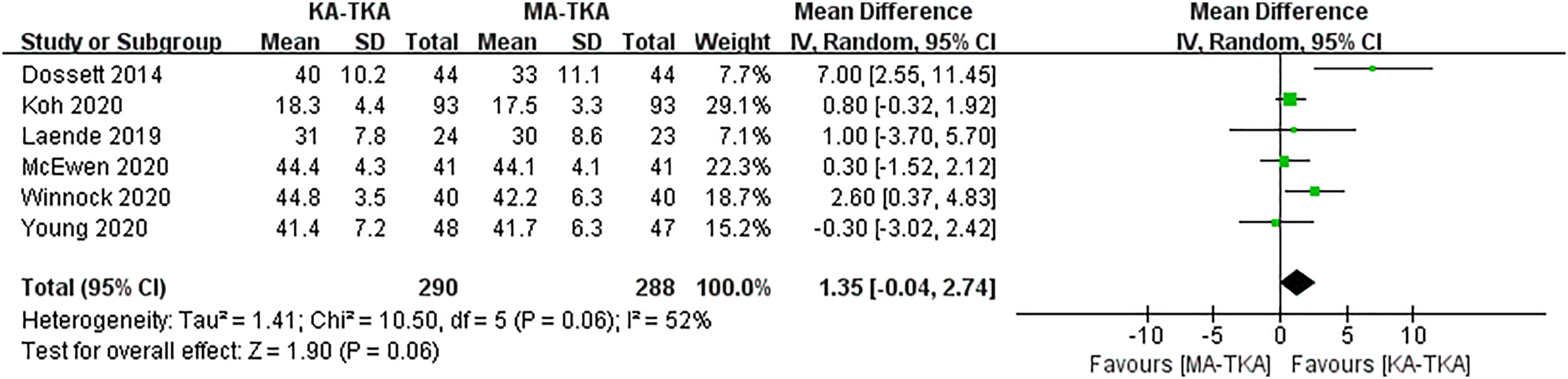
Imaging parameters
Imaging parameters included HKA angle, LDFA, MPTA and Tibial component slope angle. 8 studies reported HKA angle and MPTA, 4 studies reported JLOA and Tibial component slope angle, and 7 studies reported LDFA. For LDFA and MPTA, the pooled MD was −1.62 (95%CI:-1.93 to −1.30, p < 0.01, I2 = 9%, Figure 8) and −2.13 (95%CI:-2.55 to −1.71, p < 0.01, I2 = 56%, Figure 8), respectively, indicating that these two parameters in KA-TKA were significantly smaller than those in MA-TKA. For the other three outcome measures, there were no statistical differences between the two alignments.The results of the meta-analysis were as follows: HKA Angle (MD = −0.56, 95%CI: −1.43 to 0.32, p = 0.21, I2 = 85%, Figure 8), JLOA (MD = 0.56, 95%CI: −1.34 to 2.45, p = 0.56, I2=93%, Figure 8) and Tibial component slope angle (MD = 0.49, 95%CI: −1.02 to 2.00, p = 0.52, I2 = 90%, Figure 8). The forest plot for hip-knee-ankle angle, lateral distal femoral angle, medial proximal tibial angle and tibial component slope angle.
Flexion angle and extension angle
There were 8 studies with 656 patients comparing the flexion angle of the knee in KA-TKA and MA-TKA. The meta-analysis results showed that knee flexion angle in KA-TKA was similar to that in MA-TKA (MD = 0.89, 95%CI: −0.93 to 2.72, p = .34, I2 = 16%, Figure 9). Five studies evaluated knee extension angle with 476 patients, and the pooled MD was −0.01 (95%CI: 0.95 to 0.94, p = .99, I2=58%, Figure 9), indicating an identical result with the above. The forest plot assessing flexion angle and extension angle between the two alignment techniques.
Operation time and length of hospital stay
Detailed data on the length of hospital stay and the operation time were provided in two studies. Meta-analysis results showed that there was no statistical difference in the length of hospital stay between KA-TKA and MA-TKA (MD = 1, 95%CI: −0.16 to 2.16, p = 0.09, I2 = 0%, Figure 10). And the operative time in KA-TKA and MA-TKA were similar (MD = −2.61, 95%CI: −12.02 to 6.80, p = .59, I2 = 59%, Figure 10). The forest plot for operation time and length of hospital stay.
Ligament release
The number of ligament release was recorded in 366 patients in four studies.
Meta-analysis result showed that the ligament release rate in KA-TKA was similar to that in the MA-TKA (MD = 0.48, 95%CI: 0.16 to 1.39, p = 0.18, I2=66% Figure 11). The forest plot assessing ligament release rate between kinematic alignment-total knee arthroplasty and kinematic alignment-total knee arthroplasty.
Discussion
The main findings of this study were that the CKSS and KSS in KA-TKA was higher than that in MA-TKA, the MPTA and LDFA in KA-TKA group were smaller than that in MA-TKA, and other outcome measures were similar in the two alignment techniques, including WOMAC, KSS, KFS, KOOS (Symptoms, Pain, Daily Living, Sport, Quality of Life), OKS, HKA, JLOA, extension/flexion angle, tibial component slope angle, operation time and hospital stay.
In terms of postoperative knee function scores, except for CKSS and KSS, there was no statistical difference between KA-TKA and MA-TKA. Since only 2 studies provided data on CKSS and KSS, and the sample size was small, combined with the results of the comparison of multiple functional scores, we believe that the postoperative function obtained by the two alignment techniques may be similar. The results were consistent with those of previously published studies.14,15 A meta-analysis 14 of 9 studies showed that the KOOS, KSS and Euroqol 5-dimension questionnaires of KA-TKA group were similar to those of MA-TKA group. Another study 15 that included 229 KA patients and 229 MA patients also reported similar WOMAC and KSS between the two alignments.
In our Meta-analysis results, MPTA and TPLA of KA-TKA were significantly smaller than those of MA-TKA, which is consistent with the previous results of Young et al. 16 The reason may be the different concepts of the two alignment techniques in guiding knee arthroplasty. KA technique is designed to restore the state of the knee before the injury, and it has been reported that the lower limb alignment of most healthy people is not neutral at 0°, but slightly varus.5,6 The MA technique aims to reconstruct the neutral position on the two-dimensional plane, which can theoretically balance the internal and external pressure of the knee joint compartment, reduce the wear of the prosthesis, and help to prolong the service life of the knee prosthesis. However, Howell et al. followed 214 patients for an average of 6.3 years and found that the survival rate of the knee prosthesis in KA-TKA was comparable to that in MA-TKA. 17
KA-TKA is designed to restore the axis of motion of the knee to the original axis of motion, thereby avoiding the step of releasing the ligaments around the knee and shortening the operative time. 18 However, the results of our meta-analysis showed that the operation time and the rate of ligament release in KA-TKA was similar to that in MA-TKA, which was not consistent with the above theoretical analysis results. Therefore, the speculation by some experts that excessive loosening of the ligaments around the knee was the cause of low patient satisfaction after MA-TKA may not be reliable. 19 We believed that whether the ligaments around the knee need to be released was related to the degree of knee deformity and the surgeon’s habit. And KA-TKA was not suitable for all patients. If the patient had a severe physiological varus or valgus, the wear and survivorship of implants after KA-TKA shoud be a concern.
KA-TKA is designed to accurately restore the surface morphology of the distal femoral condyle and the posterior femoral condyle, but it is difficult to take into account the patellofemoral joint. Whether KA-TKA can lead to patellofemoral joint complications has been a controversial hotspot. Nagai et al. 19 reported that the patellar shift at 30° flexion was significantly greater in KA-TKA than in MA-TKA and Ishikawa et al. 20 indicated that the knee motion after KA-TKA is close to normal knee, but the contact stress of patellofemoral joint and tibiofemoral joint is significantly increased, which may increase the risk of prosthesis wear. However, recent studies21,22 have shown that KA-TKA with a conventional prosthesis does not result in patellofemoral alignment abnormalities and can make the patellofemoral alignment closer to normal.
Our study still had the following shortcomings: (1) The analysis results of some outcome indicators showed high heterogeneity, which may be related to the difference in the operation of the operator or the choice of implants. Due to the limitation of the number of literatures, we did not conduct in-depth analysis. (2) Although the follow-up time was limited to at least 1 year, we still could not draw a conclusion on the long-term results of the two alignment TKAs. (3) Part of the studies were cohort studies, which may reduce the reliability of this study. (4) Due to the lack of data in the literature, we did not analyze the survivorship of implants and the parameters related to patellofemoral joint. (5) With respect to ligament release, only the rate of ligament release was compared, not the degree of ligament release, and the results should be interpreted with caution.
Due to the uneven quality of the included literature and different follow-up time, the significance of our study is limited, which plays a certain reference role for clinical work. In the future, higher quality studies are needed to make up for the shortcomings of our study.
Conclusions
Meta-analysis showed that the postoperative knee function score obtained by KA-TKA was comparable to that obtained by MA-TKA. KA may be a viable reference in total knee replacement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.