
Abstract
Background
This study aimed to compare the impact of mechanical alignment (MA), anatomic alignment (AA), kinematic alignment (KA), and restrictive KA (rKA) on native coronal alignment in Asian osteoarthritic knees undergoing total knee arthroplasty (TKA). It also assessed the proportion of KA patients requiring rKA adjustment and compared early postoperative function between the two.
Methods
A retrospective analysis of 700 knees involved measuring lateral distal femoral and medial proximal tibial angles on long-leg radiographs. Coronal plane alignment of the knee (CPAK) classification was determined using the arithmetic hip-knee-ankle angle and joint line obliquity (JLO). Simulations of MA, AA, KA, and rKA were performed to observe changes. The proportion of patients requiring adjustment to the rKA safe range was recorded. Postoperative functional scores at 1 year were compared between KA and rKA groups.
Results
KA preserved native coronal alignment entirely. MA and AA altered constitutional alignment in 71.1% and 71.7% of cases, respectively, versus 8.9% for rKA. CPAK classification changed in 91.7% (MA), 80.0% (AA), and 31.7% (rKA) of cases. Only 31.9% of patients fell within the rKA safe range without adjustment; 68.2% required corrective osteotomy. No significant difference in 1-year functional scores was found between KA and rKA groups.
Conclusions
KA preserves native alignment, while rKA causes the least alteration among alternative techniques. Early functional outcomes are similar, though most patients require adjustment to meet rKA’s safe coronal alignment boundaries.
Introduction
Total knee arthroplasty (TKA) is an effective treatment for end-stage osteoarthritis. For a long time, neutral mechanical alignment (MA) of the lower limbs has been considered the gold standard for TKA alignment.1,2 Under this principle, surgeons place the femoral and tibial components perpendicular to the mechanical axis to achieve a level joint line and neutral mechanical axis, which is believed to provide the optimal mechanical environment for the prosthesis, thereby increasing its longevity. 3 Owing to ongoing improvements in prosthetic design and advancements in technology, surgical precision has gradually increased 4 ; however, there remains a high rate of dissatisfaction after TKA.5–10
An increasing number of studies have revealed a diverse distribution of lower limb alignment in the population. Although MA has good reproducibility, it significantly alters the original anatomical structure. Moreover, excessive laxity of the soft tissue after MA is a major contributor to postoperative dissatisfaction.5,11–13 Bellemans et al. reported the presence of constitutional varus caused by varus alignment since skeletal maturity. For these patients, the restoration of neutral alignment is not normal. 14 The coronal plane alignment of the knee (CPAK) classification was introduced by MacDessi et al. and is a simple yet comprehensive system for describing knee alignment by considering both constitutional alignment and joint line obliquity (JLO). 15 This classification has been increasingly accepted by scholars in various countries.16,17 In addition, an increasing number of studies indicate that preserving the CPAK classification during lower limb surgeries can lead to better functional outcomes, improved intraoperative balance, and greater postoperative satisfaction.18–20 On this basis, several personalized alignment strategies for TKA have been developed to minimize changes to the native coronal alignment to achieve better functional outcomes. 21 However, there is still a lack of sufficient research on the impact of various alignment techniques on alignment in the Asian population. 22
In KA, preserving the patient’s original alignment and occasional active soft tissue release results in more natural knee movement23,24 and soft tissue balance postoperatively,25,26 as evidenced by clinical outcomes that are superior to those of MA.27,28 However, some extreme alignment situations after KA may affect the long-term survival rate of the prosthesis. To address this issue, restrictive kinematic alignment proposed by Blakeney and Vendittoli et al. avoids extreme postoperative alignments by setting a safe range. 29 rKA avoids extensive alterations to the patient’s lower limb anatomy 30 and somewhat ameliorates prosthesis malpositioning that may result from KA, leading to a postoperative gait pattern that approximates the gait pattern at the time of nonoperative surgery 31 ; thus, it may be considered an ideal compromise for KA. Although Almaawi et al. 13 reported that 51% of patients were in the acceptable range for rKA, lower limb alignment varies considerably across ethnic and regional groups, with structural entropion being particularly prevalent in Asian populations.32,33 There are no investigations of the percentage of Asian patients with osteoarthritis of the knee that require adjustment of the alignment to within the safe range or comparisons of functional outcomes after KA versus rKA.
The purpose of this study was to analyze the changes in native coronal alignment among Asian osteoarthritis patients who underwent TKA on the basis of different alignment objectives and to evaluate the proportion of patients who require adjustment of the revised rKA to a safe range. Moreover, the early postoperative functional outcomes of KA and rKA were also compared. We hypothesized that rKA would minimize changes in native coronal alignment more effectively than KA would, which preserved native coronal alignment, and that there would be no difference in early postoperative functional outcomes between the two alignment techniques.
Methods
Participants
Data were retrospectively collected from patients who underwent primary total knee arthroplasty due to knee osteoarthritis at our institution between January 2018 and December 2023 after approval was obtained from the ethics committee. The exclusion criteria included traumatic arthritis, previous lower extremity internal fixation surgery, combined severe bone defects (Ahlback ≥ grade 3), non-OA side knees, substandard or poor quality full-length films of the lower extremity, and no full-length radiographs of the lower extremity in the standing position. A total of 390 patients with 700 knees were included in this study. The inclusion and exclusion process was completed by two orthopedic residents, who reviewed the medical records and imaging data individually.
Radiological measurements
Lower extremity alignment parameters were measured by an orthopedic surgeon with extensive clinical experience in the picture archiving and communication system. The center of the femoral head is determined using the best-fit circle method, and the center of the ankle joint is defined as the midpoint of the talus. The mechanical femoral axis is defined as the line between the center of the femoral head and the apex of the intercondylar notch of the femur. The mechanical tibial axis is defined as the line between the center of the ankle joint and the midpoint of the intercondylar eminence of the tibia. The lateral distal femoral angle (LDFA) is defined as the angle formed between the tangential line of the bottoms of both femoral condyles (the femoral joint line) and the mechanical femoral axis. The medial proximal tibial angle (MPTA) is defined as the angle formed between the tangential line of the surfaces of both the tibial plateaus (the tibial joint line) and the mechanical tibial axis. aHKA is calculated using the following formula: aHKA = MPTA - LDFA. The JLO is calculated using the following formula: JLO = MPTA + LDFA.
An aHKA less than 2° is defined as constitutional varus alignment, a value greater than 2° is defined as constitutional valgus alignment, and a neutral aHKA is 0 ± 2°. Neutral JLO is defined as 180 ± 3°, and the apex distal JLO was less than 177°, whereas the apex proximal JLO was greater than 183°. The CPAK classification is ascertained based on the aHKA and JLO. The CPAK classification is ascertained based on two independent variables: aHKA (with subgroups of varus, neutral, and valgus) and JLO (with subgroups of distal, neutral, and proximal). The three subgroups of aHKA and the three subgroups of JLO form nine distinct knee joint phenotypes in a matrix. After the measurements were completed, 100 knee joints were randomly selected and measured by another orthopedic attending physician to assess interobserver consistency.
Simulation protocols for different alignment techniques
Four different TKA alignment techniques were simulated. In MA, the target alignment is perpendicular to the mechanical axes of the femur and tibia, keeping the LDFA and MPTA at 90°, thereby restoring a neutral aHKA. In AA, the femoral lateral alignment is set to a fixed position of 3° valgus relative to the mechanical axis of the limb, whereas the tibial lateral alignment is set to a fixed position of 3° varus relative to the mechanical axis of the limb, resulting in a neutral overall lower limb alignment. 34 In KA, the goal is to restore the coronal plane alignment and joint line inclination of the lower limb to the patient’s prearthritic condition, so the target alignment is consistent with the patient’s native coronal alignment. 29 rKA is planned in accordance with the method established by Laforest et al. 35 ; the coronal alignment of the femoral and tibial sides is maintained within 90 ± 5°, whereas the safety range for overall lower limb alignment is within 0 ± 3°. When adjustments are needed for the femoral and tibial alignment to keep the overall lower limb alignment within the safe range, adjustments to the tibial side should be prioritized. All plans were completed by an orthopedic attending physician with several years of experience and were verified by another orthopedic chief physician. The team records and compares the degree and proportion of changes in the LDFA, MPTA, constitutional alignment, JLO, and CPAK classification before and after the four alignment techniques.
Clinical results
From February 2023 to July 2024, 60 patients with knee osteoarthritis who underwent TKA were included; these patients were recruited from a previously registered RCT. The patients were divided into a KA group and a rKA group based on different alignment strategies. All TKAs were performed using patient-specific instrumentation (PSI) by the same senior surgeon under general anesthesia. There were no statistically significant differences in the demographic parameters between the two groups of patients. The preoperative and one-year postoperative KOOS-12, visual analogue scale (VAS) pain scores, EQ-VAS scores, range of motion (ROM), and forgotten joint score (FJS) were collected and compared between the two groups. All the data were recorded by a researcher who was not involved in the surgery and was unaware of the group assignments. This researcher received systematic training before the assessment. All patients underwent standardized postoperative pain management, anticoagulation, infection prevention, and rehabilitation measures.
Statistical analysis
Statistical analysis was performed using SPSS 27.0 (SPSS, Chicago, IL, USA). A scatter plot was used to describe the distribution of the CPAK classification in the population. Continuous data are presented as means and standard deviations, whereas categorical data are presented as percentages. The Shapiro‒Wilk test was performed to determine whether the continuous variables in each group were normally distributed. If the data were normally distributed, one-way analysis of variance (ANOVA) was used to compare the differences in the changes in alignment parameters among different alignment strategies. When ANOVA indicated statistical significance, post hoc multiple comparisons were conducted. If the continuous variables were not normally distributed, the Kruskal‒Wallis test was used to determine the differences between groups. Independent samples t tests or Wilcoxon rank-sum tests were used to compare differences in functional outcomes between KA and rKA. Chi-square tests and Fisher’s exact tests were used to determine the differences in categorical variables. A P value <0.05 indicated statistical significance. The intraclass correlation coefficient (ICC) was used to assess the consistency of measurements between the two assessors.
Results
Demographic characteristics.

Abbreviations: BMI: body mass index; LDFA: lateral distal femoral angle; MPTA: medial proximal tibial angle; aHKA: arithmetic hip-knee-ankle angle; JLO: joint line obliquity.

Distribution of the CPAK of native coronal knee alignment. LDFA, lateral distal femoral angle; MPTA, medial proximal tibial angle; aHKA, arithmetic hip-knee-ankle angle; JLO, joint line obliquity.
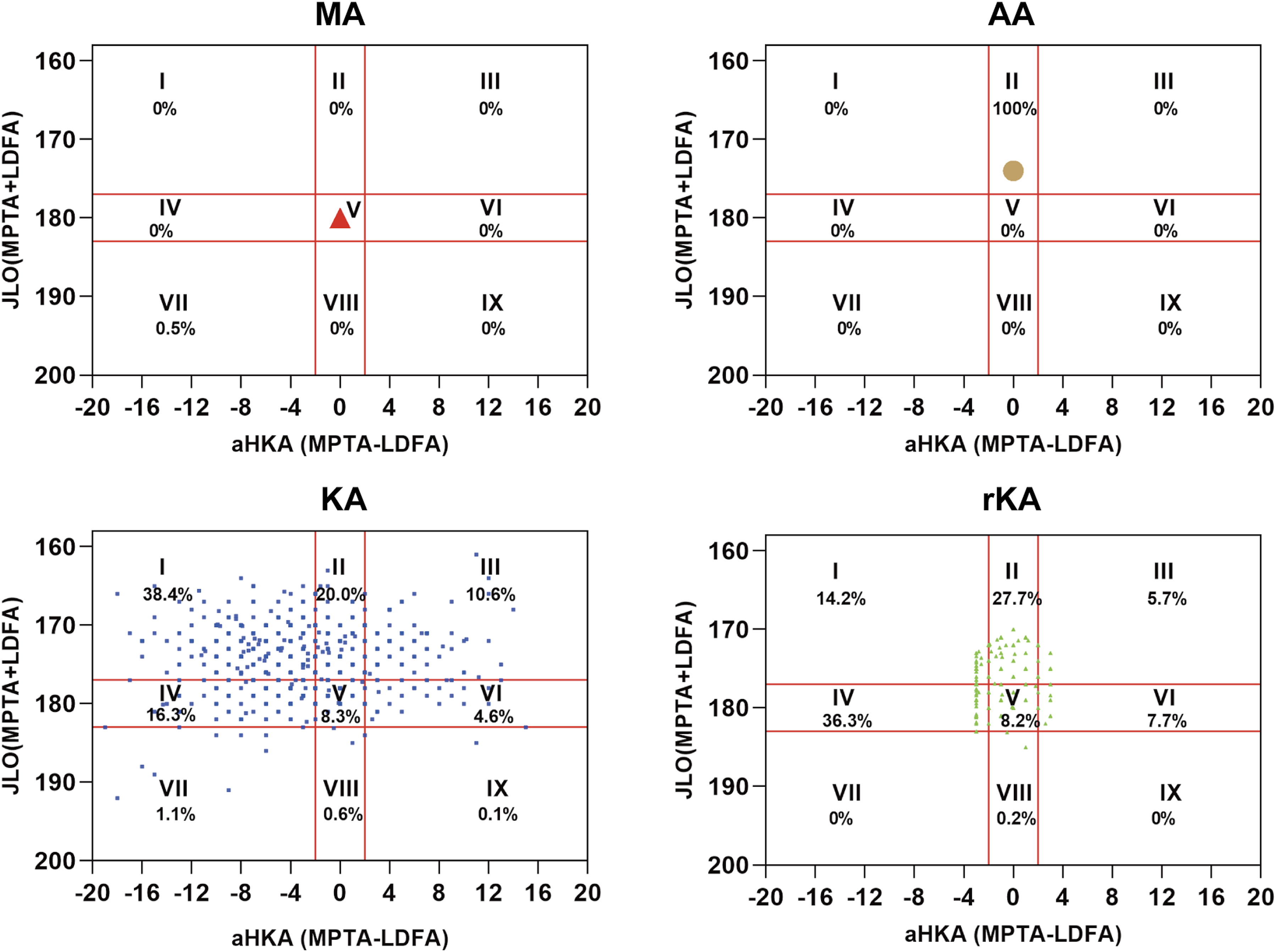
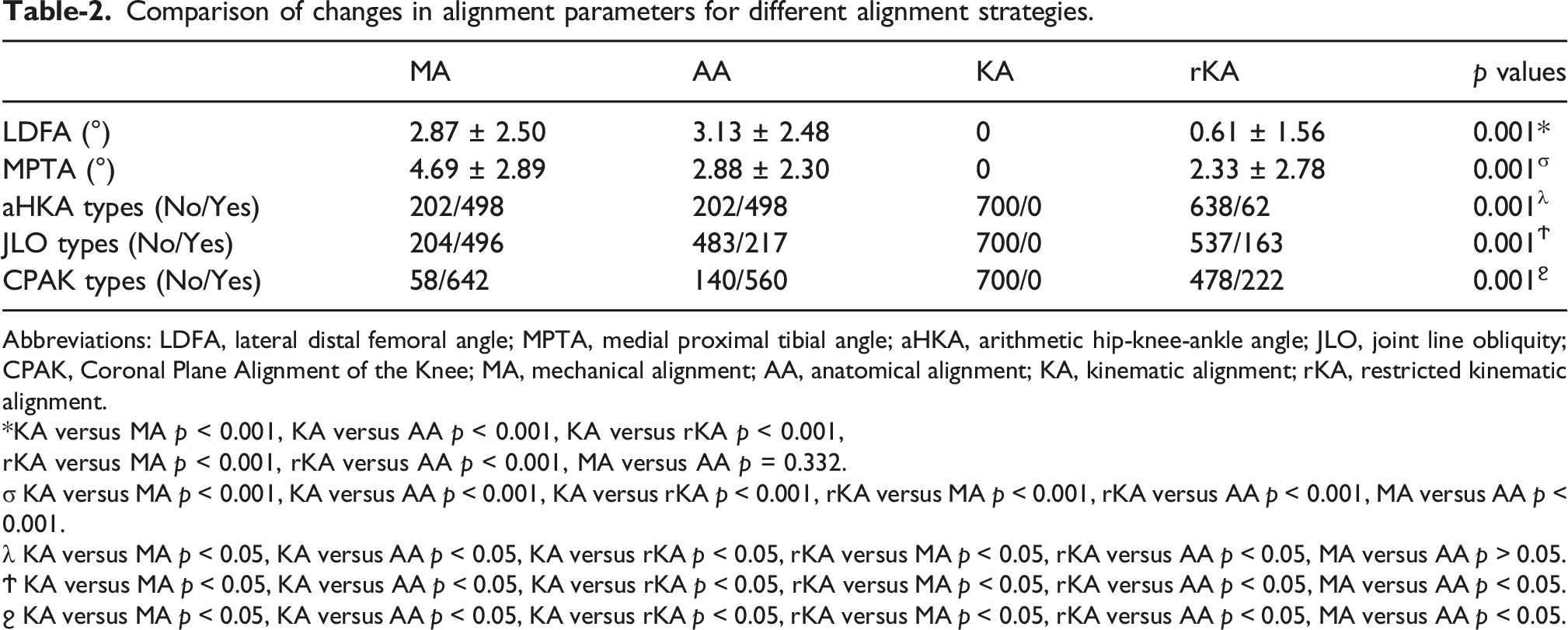
With respect to the postoperative lower limb alignment results (Figures 2 and 3), KA preserved the native coronal alignment and CPAK classification. With respect to the aHKA, both the MA and AA groups achieved neutral alignment postoperatively; in the rKA group, 50% of patients had varus alignment, 36.14% had neutral alignment, and 13.43% had valgus alignment. With respect to JLO, the MA group was in a horizontal position postoperatively, whereas the AA group was consistently in a distal position; in the rKA group, 47.57% were distal, 52.14% were horizontal, and 0.29% were proximal. With respect to the CPAK classification, the MA group was uniformly classified as CPAK Type V, whereas the AA group was uniformly Type II. In the rKA group, 14.2%, 27.7%, and 36.3% were Types I, II, and IV, respectively. In addition to KA, which maintained the original line parameters, rKA resulted in the smallest change in line parameters, with postoperative alterations in the LDFA and MPTA of 0.61° and 2.33°, respectively, both of which were significantly smaller than those of MA and AA (p < 0.05). With respect to the aHKA, rKA maintained approximately 91.1% of the constitutional alignment, whereas both MA and AA caused a shift to a neutral constitutional alignment, with change rates of 71.1%. The differences between rKA and KA were statistically significant. With respect to JLO, rKA maintained 76.7% of the original joint line direction, which was significantly greater than that of MA (29.1%) and AA (69.0%). Additionally, the changes in the MPTA, JLO, and CPAK classification for AA were less than those for MA. See Table 2 for details. Postoperative knee phenotypes according to different alignment techniques. (a) Postoperative constitutional alignment according to different alignment techniques. (b) Postoperative joint line obliquity according to different alignment techniques. aHKA, arithmetic hip-knee-ankle angle; MA, mechanical alignment; AA, anatomical alignment; KA, kinematic alignment; rKA, restricted kinematic alignment. Postoperative CPAK classifications according to different alignment techniques. LDFA, lateral distal femoral angle; MPTA, medial proximal tibial angle; aHKA, arithmetic hip-knee-ankle angle; JLO, joint line obliquity; MA, mechanical alignment; AA, anatomical alignment; KA, kinematic alignment; rKA, restricted kinematic alignment. Comparison of changes in alignment parameters for different alignment strategies. Abbreviations: LDFA, lateral distal femoral angle; MPTA, medial proximal tibial angle; aHKA, arithmetic hip-knee-ankle angle; JLO, joint line obliquity; CPAK, Coronal Plane Alignment of the Knee; MA, mechanical alignment; AA, anatomical alignment; KA, kinematic alignment; rKA, restricted kinematic alignment. *KA versus MA p < 0.001, KA versus AA p < 0.001, KA versus rKA p < 0.001, rKA versus MA p < 0.001, rKA versus AA p < 0.001, MA versus AA p = 0.332. σ KA versus MA p < 0.001, KA versus AA p < 0.001, KA versus rKA p < 0.001, rKA versus MA p < 0.001, rKA versus AA p < 0.001, MA versus AA p < 0.001. λ KA versus MA p < 0.05, KA versus AA p < 0.05, KA versus rKA p < 0.05, rKA versus MA p < 0.05, rKA versus AA p < 0.05, MA versus AA p > 0.05. Ϯ KA versus MA p < 0.05, KA versus AA p < 0.05, KA versus rKA p < 0.05, rKA versus MA p < 0.05, rKA versus AA p < 0.05, MA versus AA p < 0.05. ϩ KA versus MA p < 0.05, KA versus AA p < 0.05, KA versus rKA p < 0.05, rKA versus MA p < 0.05, rKA versus AA p < 0.05, MA versus AA p < 0.05.
In terms of rKA, 22.4% (157/700) of the patients required adjustments on the femoral side, whereas 61.7% (432/700) needed adjustments on the tibial side. Both femoral and tibial adjustments were required in 16% (112/700) of cases to ensure that the target line was within the safe range. Only 31.9% (223/700) required no adjustments at all.
Comparison of functional outcomes between KA and rKA TKA.
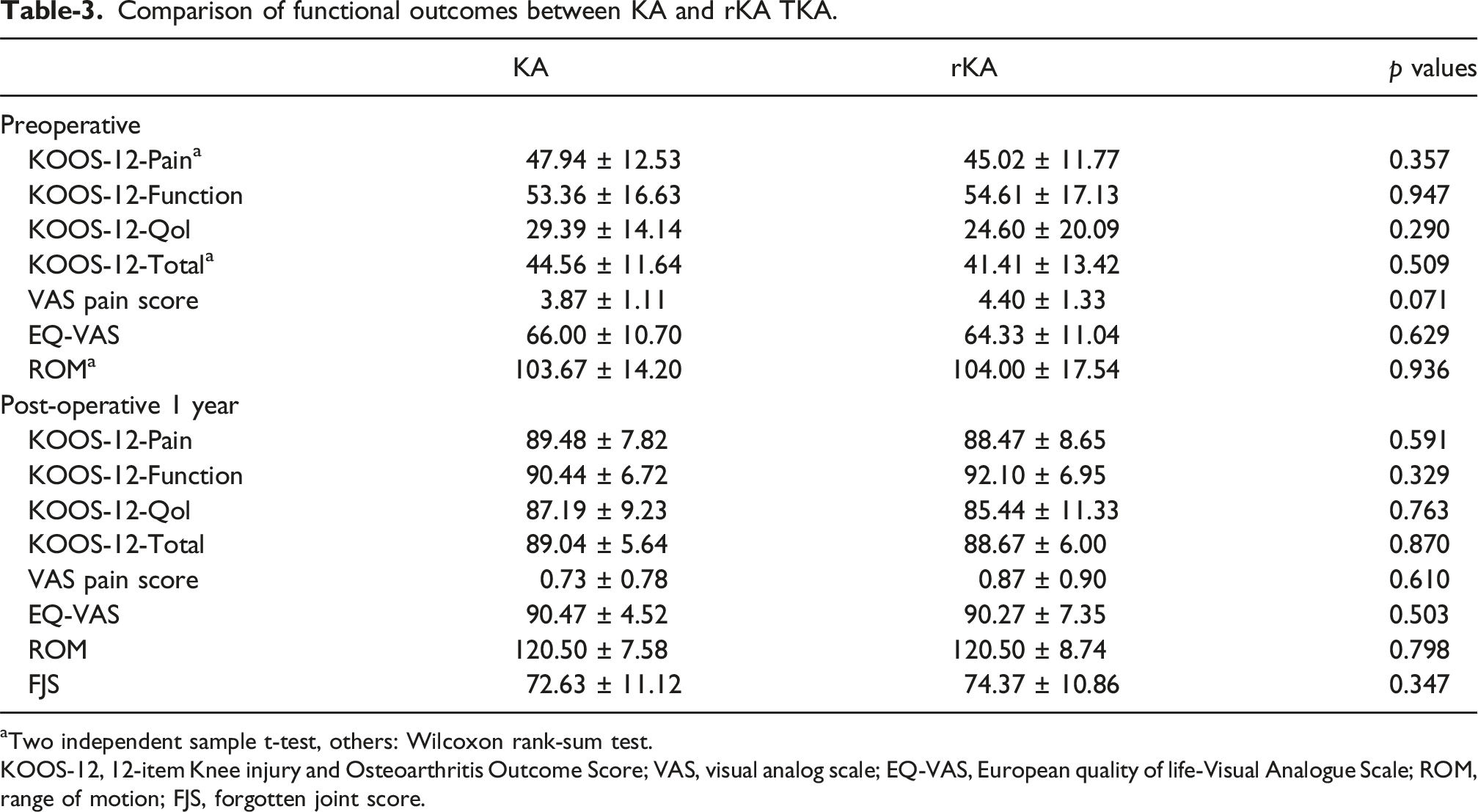
aTwo independent sample t-test, others: Wilcoxon rank-sum test.
KOOS-12, 12-item Knee injury and Osteoarthritis Outcome Score; VAS, visual analog scale; EQ-VAS, European quality of life-Visual Analogue Scale; ROM, range of motion; FJS, forgotten joint score.
Discussion
To our knowledge, this is the first study to explore the impact of different alignment strategies on original alignment changes in TKA among Asian populations. In this study, the KA group maintained the original alignment, whereas the rKA group presented the smallest change in alignment. Furthermore, only 30% of knees subjected to KA fell within the acceptable range for alignment, whereas approximately 70% required adjustments with the rKA technique to avoid extreme alignments postoperatively. However, there were no differences in early functional recovery between the KA and rKA alignment strategies. Given the minimal differences in alignment changes and similar functional outcomes between KA and rKA, along with the potential risk of long-term failure associated with extreme alignment using KA, rKA may be a suitable alternative alignment strategy for TKA in Asian populations.
This study revealed that, in addition to kinematic alignment, postoperative alignment using various TKA alignment techniques significantly differs from the anatomical alignment of the lower extremities. Changes in alignment and anatomical structure can lead to alterations in the tension of the ligaments surrounding the knee joint. 36 Postoperatively, this may result in asymmetrical tension of the medial and lateral collateral ligaments, which can affect knee stability and alter the patient’s movement patterns. Consequently, this may impair the flexion and extension of the knee as well as its internal and external rotation functions, leading to pain and injury. 13 Apart from KA, all other alignment techniques altered the alignment. The changes in the aHKA after the four alignment techniques were 71.1%, 71.1%, 0%, and 8.9%, respectively. Overall, KA is almost a purely bony procedure (except collateral ligament release) and does not affect alignment. Therefore, compared with MA and AA, KA in TKA can achieve faster recovery, better functional outcomes, and a lower rate of forgetting.37–39
In MA, to achieve neutral alignment and balance the load in the medial and lateral compartments of the knee joint, significant bone resection and soft tissue release are needed during surgery. The LDFA and MPTA are adjusted by 2.87 ± 2.50 and 4.69 ± 2.89 degrees, respectively. Moreover, the changes in the aHKA, JLO, and CPAK classifications show the greatest variation, with significant differences compared with other alignment techniques (p < 0.001). Quantitative bone resection and soft tissue release can affect soft tissues and patellar tracking. When the tension of the collateral ligaments is affected, the surgeon may even need to perform surgical release to achieve a suitable balance between flexion and extension. However, the significant changes in ligaments and soft tissues before and after surgery are major causes of dissatisfaction after MA TKA. 13 In AA, owing to the 3° inclination of the tibial prosthesis, it is not necessary to rotate the femoral prosthesis externally to balance the flexion gap. Typically, the femoral prosthesis is positioned parallel to the posterior condylar axis, which helps achieve a more natural knee joint anatomy than MA does and maintains a 3° natural joint line inclination. This alignment helps preserve the tension around the knee joint throughout the entire range of motion.40,41 In this study, compared with those in the MA group, the changes in the MPTA, JLO, and CPAK classification in the AA group were smaller. However, the changes in the LDFA, aHKA, and CPAK classifications were still greater than those in the KA and rKA groups. Compared with MA, AA partially restores the original anatomy of the lower limb alignment but does not sufficiently account for differences in individual alignment distribution.
In this study, the KA group showed no changes in the inherent alignment of the lower limb, JLO, or CPAK classification. Research by Rat, Rivière C, and others has shown that preserving the original knee joint morphology during TKA and UKA significantly improves postoperative patient satisfaction and functional evaluation.19,42 KA compensates for the thickness of worn and resected bone and cartilage by adjusting the thickness of the prosthesis and the insert. After osteotomy, the prosthesis is positioned parallel to the original joint line without pursuing a rectangular flexion‒extension gap, thus avoiding the need for soft tissue release and restoring tension that closely approximates physiological levels.43,44 However, preserving the original structure for all patients raises concerns, as extreme varus or valgus alignment may negatively impact long-term outcomes. Vendittoli et al. noted that certain inherent knee joint anatomical types are likely to exhibit poor biomechanics and that reconstructing these anatomical forms may be detrimental to clinical outcomes. 45 To prevent this situation, researchers have proposed setting boundaries for KA in patients with abnormal or atypical anatomical structures to avoid excessive deviations in alignments.
In MacDessi’s study, approximately 90% of knee joints were found to be within a safe range during KA without the need for adjustments. 25 However, this study revealed that approximately 70% of patients with knee osteoarthritis in the Asian population required adjustable rKA to ensure that the alignment of the prosthesis remained within a relatively safe range. This may be due to the widespread presence of physiological varus in the Asian population. 46 Specifically, 55.9% of patients were found to have structural varus (aHKA < −3°), with type I CPAK (38.4%) being the most common classification among the patients. Given the high prevalence of constitutional varus in Asians, we simulated an rKA boundary of ±5°HKA. The proportion of knees requiring no adjustment increased only modestly from 31.9% to 43.4%. While a wider boundary theoretically preserves more native alignment, it risks accepting extreme component malposition or excessive residual varus, which may compromise long-term durability. Abhari et al. reported that the satisfaction levels of patients who underwent rKA were significantly higher than those of patients who underwent MA, and there were also fewer postoperative complications. 28 By restoring normal gait parameters postoperatively, it is expected that clinical outcomes and patient satisfaction can be improved. In a prospective cohort study, we observed differences in functional scores between the patients who underwent KA and those who underwent rKA in the early postoperative phase after knee replacement surgery. The results indicated that there were no significant differences in various scores between the two groups (Table 3). This result suggested that although rKA altered the patient’s inherent alignment to some extent, there were no significant differences in early postoperative function between the two groups.
Moreover, this study has certain limitations: 1. The comparison of changes in alignment parameters following various alignment strategies in this study was based on X-ray simulations. Owing to the limited precision of surgical instruments, it is challenging to achieve complete postoperative alignment as simulated. 2. The actual thickness of the cartilage cannot be observed on X-ray images; in cases of severe degeneration, there may be wear of the subchondral bone. We used subchondral bone as a substitute, which introduces a certain degree of bias. 3. Owing to the lack of CT data, functional alignment or simulated modified mechanical alignment (aMA) assessments were not included in this study. 4. In this study, females comprised the majority (310 out of 390), which is consistent with the epidemiological findings of knee osteoarthritis in China. 5. Although this study was a prospective analysis of postoperative knee functional scores between KA and rKA, the follow-up period was relatively short, and the sample size was small. Future research should explore the long-term clinical outcomes of these two alignment techniques in a larger sample of patients with knee osteoarthritis.
Conclusion
This study demonstrates that among Asian knee OA patients undergoing TKA, KA fully preserves native coronal alignment, while rKA results in the least alteration among alignment strategies that modify constitutional anatomy. Although approximately 70% patients required adjustments within the rKA framework to avoid extreme alignments, no significant differences were observed in early postoperative functional outcomes between the KA and rKA. Given the potential long-term risks associated with extreme alignments under pure KA, rKA emerges as a viable and safer alternative, offering a balance between anatomical preservation and mechanical safety in this population.
Footnotes
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval from the Institutional Ethics Committee of Peking Union Medical College Hospital. This study was part of the research project named “Development and Validation of Artificial Intelligent Pre-operative Planning System and PSI for Total Knee Arthroplasty”. (I-22PJ942).
Consent to participate
Written informed consent was acquired from all participants.
Author contributions
Peilai Liu, Qunshan Lu and Songlin Li conceived and designed the study. Shihao Li, Songlin Li and Gongkai Chen conducted radiographic measurement. Wenwei Qian and Shihao Li analyzed data. Shusheng Wei and Yifan Li checked the data and methodology. Shihao Li and Gongkai Chen wrote the manuscript and conducted critical analysis. The authors read and approved the final manuscript. Songlin Li, Qunshan Lu and Peilai Liu contribute equally to the work and should be regarded as co-corresponding authors.
Funding
This work was supported by the National Natural Science Foundation of China (82472424), the Special Foundation for Taishan Scholars (tstp20250750), and Shandong Provincial Natural Science Foundation (Grant number: ZR2025QC2006Z).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon reasonable request. Please contact the corresponding author at