
Abstract
Objective
To investigate the correlations between clinical, functional, and radiological outcomes in inpatients with coronavirus disease 2019 (COVID-19).
Methods
In this observational study, we recruited inpatients affected by moderate COVID-19 disease. The clinical evaluation comprised the Cumulative Illness Rating Scale (CIRS), numerical rating scale (NRS), modified Rankin scale (mRS), and the modified Borg dyspnea scale (mBDS). Respiratory involvement was assessed with computed tomography (CT) and graded with a CT-severity score (CT-SS). We retrospectively assessed functioning using the International Classification of Functioning, Disability and Health (ICF) codes of the Clinical Functioning Information Tool (ClinFIT) COVID-19 in the acute phase. Correlation analysis was performed 1) between clinical, instrumental, and functional parameters and 2) between ICF categories.
Results
The data showed statistically significant moderate correlations between CT-SS and the following categories: b152 “emotional functions” and b440 “respiratory functions”.
Conclusion
This is the first study to use the ICF framework in people with a moderate form of COVID-19 in the acute phase. Considering the correlations between some ICF categories and radiological findings, our results support the use of the ClinFIT COVID-19 for a comprehensive assessment of COVID-19 patients.
Keywords
Introduction
In December 2019, a novel coronavirus (severe acute respiratory syndrome coronavirus 2; SARS CoV-2) causing coronavirus disease 2019 (COVID-19) emerged in Wuhan, China. Owing to transmission through human-to-human contact, SARS CoV-2 spread rapidly across the world, causing a pandemic. 1 Several SARS CoV-2 variants have been identified and these have led to different clinical manifestations of COVID-19, with variable transmissibility, morbidity, and mortality.2,3 The common clinical findings of COVID-19 are respiratory signs and symptoms, namely cough, shortness of breath, and chest pain, as well as other physical and psychological disorders. Mild, moderate, or severe forms of COVID-19 have been described, and the latter comprise severe pneumonia, acute respiratory distress syndrome (ARDS), sepsis, and septic shock.4,5
Hospitalized COVID-19 patients require isolation to avoid propagation of the virus. This intervention, with few environmental stimuli, may cause psychological issues that range from depression to anxiety, and eventually may lead to cognitive decline. 6 In this context, rehabilitation represents the mainstay of care in the post-intensive care unit for enhancing functional recovery, reducing the length of stay (LOS), and preventing possible long-term consequences.7,8 This approach also reduces COVID-19-related disability, thus leading to less disease burden and lower costs for healthcare systems.7,8 The pandemic has highlighted the huge need for specific rehabilitation services in COVID-19 patients, from early acute to post-acute care.9,10
Rehabilitation is defined by the World Health Organization (WHO) as “a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment”. 11 The comprehensive assessment of body functions and structures, activities and participation, and environmental and personal factors of an individual is the starting point of the person-centered rehabilitation process. The International Classification of Functioning, Disability and Health (ICF) represents the universal framework for this assessment. 12 To address the growing need for the evaluation of changes in functioning related to COVID-19, a task force of the International Society of Physical and Rehabilitation Medicine (ISPRM) developed the Clinical Functioning Information Tool (ClinFIT), which, as ClinFIT COVID- 19, is used for the assessment and reporting of functioning in COVID-19 patients in acute, post-acute, and long-term care settings. 13
The aim of this real-practice study was to correlate clinical and instrumental parameters with changes in functioning of inpatients with a moderate form of COVID-19 in a hospital in southern Italy.
Materials and methods
Participants
We collected clinical, instrumental, and functional data for inpatients with a moderate form of COVID-19, who were hospitalized in the COVID-19 Unit of the San Giovanni Bosco Hospital in Naples, Italy, from 1 January 2021 to 31 May 2021. We enrolled both men and women older than 18 years with 1) positive results for nasal and pharyngeal swabs for SARS-CoV-2, evaluated by the real-time reverse transcriptase-polymerase chain reaction (RT-PCR) assay; 2) diagnosis of moderate illness (evidence of lower respiratory disease during clinical assessment or imaging, with oxygen saturation (SpO2) ≥94% on room air at sea level) in accordance with COVID-19 treatment guidelines; 14 and 3) absence of cognitive impairment (Short Portable Mental Status Questionnaire (SPMSQ) score ≥8). All patients’ details were de-identified to protect their privacy, and all patients provided written informed consent, in accordance with the guidelines of the Helsinki Declaration. The Ethical Committee of the University of Campania Luigi Vanvitelli approved the study (approval number: 0017390/2020).
This study was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. 15
Outcomes
Data collection comprised anamnestic and anthropometric data, and the following outcome measures:
Cumulative Illness Rating Scale (CIRS), which was used to assess physical illness burden through two indices, the Illness Severity Index (SI) and the Comorbidity Index (CI);
16
numerical rating scale (NRS), which was used to measure pain intensity; we considered a score of 0 as “absence” of pain; 1–3 as “mild” pain, 4–6 as “moderate” pain, and 7–10 as “severe pain;
17
modified Rankin scale (mRS), which was used to evaluate patient disability;
18
modified Borg dyspnea scale (mBDS), which was used to measure patient-reported dyspnea.
All patients underwent chest computed tomography (CT), and the images were analyzed by a radiologist who reported the CT severity score (CT-SS), which is an objective method to identify significant radiological differences between severe and mild cases of COVID-19. The overall CT-SS ranges from 0 (no signs) to 25 points, with a cut-off value of 7 (sensitivity: 80.0%; specificity: 82.8%).19,20
We also retrospectively assessed the functioning of COVID-19 patients using the ICF codes for COVID-19 identified by the ClinFIT task force. 13 The ClinFIT COVID-19 for the acute phase comprises 13 ICF categories; 10 for “body functions” and 3 for “activity and participation” (Table 1). 13 To rate the severity of a problem, we used the scale provided in the ICF indicated as “qualifiers”. The qualifiers are classified as 0 for no problem, 1 for mild problem, 2 for moderate problem, 3 for severe problem, and 4 for complete problem. 21
ICF codes included in the ClinFIT COVID-19 categories for the acute setting.

Statistical analysis
The collected data were analyzed using the Statistical Package for the Social Sciences 25 (SPSS 25; IBM Corp., Armonk, NY, USA) software to perform a correlation analysis between the patients’ vital signs, disability level, patient-reported dyspnea, CT-SS, and ClinFIT COVID-19 categories. Normality was evaluated using the Shapiro–Wilk test. Correlation analysis was performed using Pearson’s correlation coefficient or Spearman’s rank correlation, in the case of non-parametric variables. We considered a significance threshold of p < 0.05, and we considered the following cut-offs and strengths for the correlation coefficient: 0.2–0.39 as weak, 0.40–0.59 as moderate, 0.6–0.79 as strong, and 0.8–1 as very strong correlation.
Results
The demographic, clinical, and functioning/disability data of the 23 recruited patients are shown in Table 2. Regarding the severity of dyspnea, 8 patients (34.8%) had no dyspnea, 3 (13.04%) had mild dyspnea, 10 (43.5%) had severe dyspnea, 1 (4.3%) had very severe dyspnea, and 1 (4.3%) had critical dyspnea. The CT-SS indicated moderate to severe radiological disease (overall score >7) in 14 patients (60.9%), while 9 patients (39.1%) had mild signs. The severity of each problem in accordance with the ICF codes identified in the ClinFIT COVID-19 and retrospectively obtained from the information reported in the medical records of our population is shown in Table 3.
Demographic, clinical, and functioning/disability data of our population.

All variables were normally distributed. Continuous variables are expressed as mean ± standard deviation; discrete variables are expressed as total number (%).
COVID-19, coronavirus disease 2019; T, temperature; HR, heart rate; bpm, beats per minute; SpO2, oxygen saturation; NRS, numerical rating scale; CIRS-SI, Cumulative Illness Rating Scale-Severity Index; CIRS-CI: Cumulative Illness Rating Scale-Comorbidity Index; mRS: modified Rankin scale.
The ICF codes of ClinFIT COVID-19 and their qualifiers obtained retrospectively from the medical records of our population (n = 23).

Note: The values are expressed as number (percentage).
ICF, International Classification of Functioning, Disability and Health; ClinFIT, Clinical Functioning Information Tool; COVID-19, coronavirus disease 2019.
The correlations between age, vital signs, disability level, patient-reported dyspnea, CT-SS, and functioning level are shown in Table 4. Specifically, age was moderately correlated with impairment of “mobility of joint functions” (ICF code: b710) (p = 0.046), and the CIRS-SI was moderately correlated with ICF code b280 “sensation of pain” (p = 0.045) and “walking” (ICF code: d450) (p = 0.033). Regarding pain, no correlations were found between the NRS scores and the ICF codes. The mBDS and mRS scores showed moderate correlations with reduced “muscle power functions” (ICF code: b730) (p = 0.041 and p = 0.037, respectively), and the mBDS score was moderately correlated with “walking” (ICF code: d450) (p = 0.011). Regarding the instrumental findings, moderate correlations were found between the CT-SS and impairments in the following ICF codes: b152, “emotional functions” (p = 0.040) and b440, “respiratory functions” (p = 0.004). Table 5 shows the correlations between the different ICF codes.
Correlation coefficients and p-values between age, pain, disability level, comorbidity, patient-reported dyspnea, CT severity score, and the ICF codes included in the ClinFIT COVID-19.
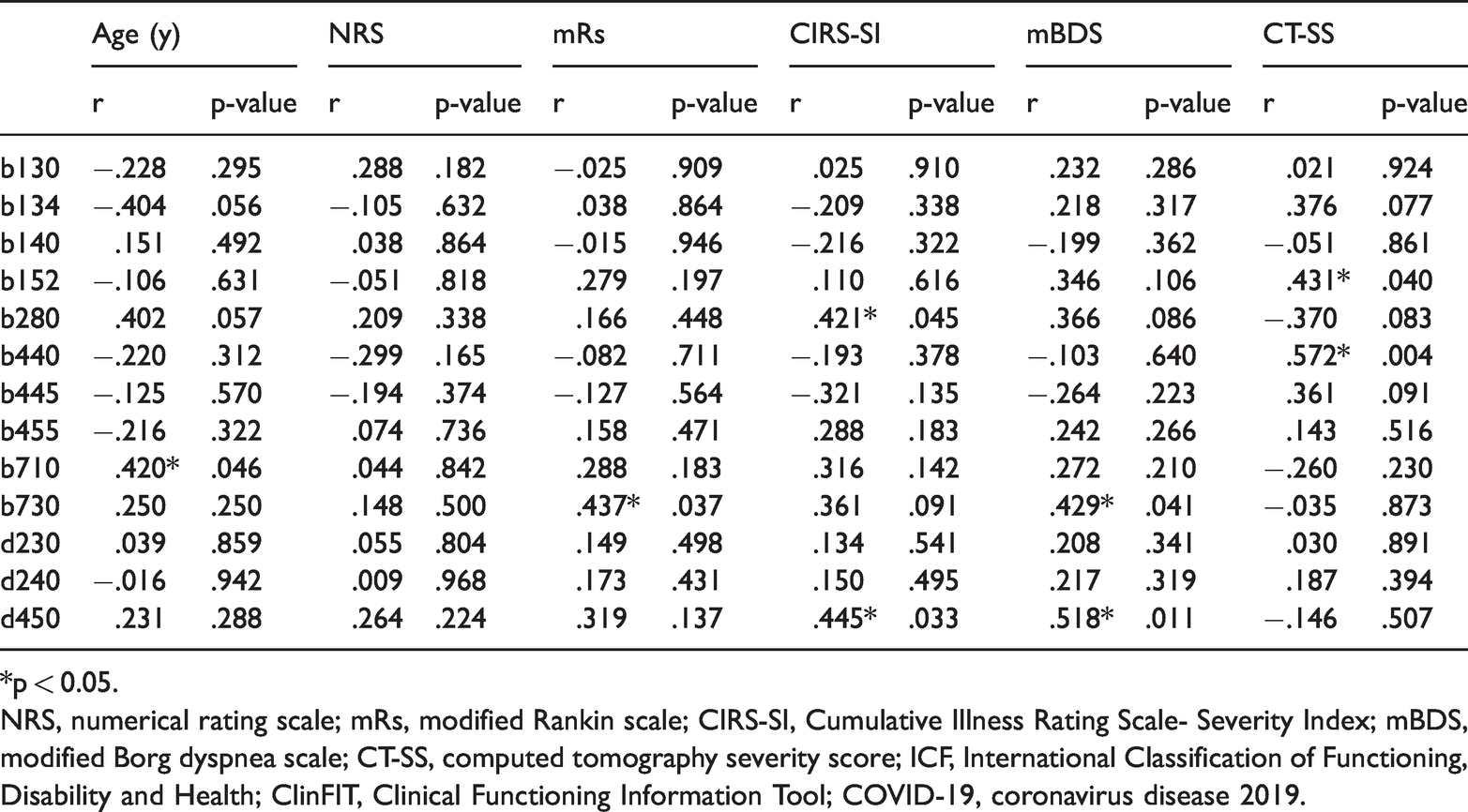
*p < 0.05.
NRS, numerical rating scale; mRs, modified Rankin scale; CIRS-SI, Cumulative Illness Rating Scale- Severity Index; mBDS, modified Borg dyspnea scale; CT-SS, computed tomography severity score; ICF, International Classification of Functioning, Disability and Health; ClinFIT, Clinical Functioning Information Tool; COVID-19, coronavirus disease 2019.
Correlation coefficients and p-values between the ICF codes included in the ClinFIT COVID-19.

*p <0.05.
ICF, International Classification of Functioning, Disability and Health; ClinFIT, Clinical Functioning Information Tool; COVID-19, coronavirus disease 2019.
Discussion
To the best of our knowledge, this is the first study to use the ICF framework to characterize the functioning level of people with a moderate form of COVID-19 in the acute phase and to correlate clinical, functioning, and instrumental data to better understand the potential role of rehabilitation in this population.
We used the ICF codes identified by the ClinFIT Task Force for the ClinFIT COVID-19 retrospectively and analyzed the correlations between each category and between each category and all other clinical and instrumental data. We found statistically significant very strong correlations, as expected, between some categories, namely b134, “sleep functions” and d240, “handling stress and other psychological demands”, and between b710, “mobility of joint functions” and d450, “walking”. We also found strong correlations between “respiratory functions” and “respiratory muscle functions”, “mobility of joint functions” and “muscle power functions”, and “muscle power functions” and “walking”. As expected, we found a correlation between the CT-SS and “respiratory functions”, which confirmed the utility of the instrumental tool to evaluate functional lung damage. Moreover, it is key to note the relationship between CT-SS and “emotional functions”, suggesting that an impaired clinical and radiological scenario might lead to anxiety, sadness, and anger in the acute setting. This issue has not been as well investigated in acute patients as it has in patients with long-COVID syndrome 22 and discharged patients. 23
Patients affected by COVID-19 complain of several signs and symptoms involving systems other than the respiratory system. Indeed, since the beginning of the pandemic, the heavy impact of SARS-CoV-2 infection on different body systems has been clear, with a negative influence on body functions, activities, and social participation. 24 To improve and standardize the assessment of functioning in people with COVID-19, the ClinFIT COVID-19 was recently developed for acute, post-acute, and long-term care settings. 13 This tool aims to identify the main clinical and functional issues and rate their severity in patients with COVID-19, a mandatory approach to providing effective and appropriate rehabilitation care.
From the analysis of our data, as expected, the respiratory system was heavily impacted in COVID-19 patients in the acute phase. Approximately half of our patients showed severe to very severe dyspnea. These results are similar to those reported by Al Chikhanie et al, who reported a mean of 4.4 ± 2.3 (“somewhat severe dyspnea”) using the modified Borg dyspnea scale in patients undergoing pulmonary rehabilitation, demonstrating severe short-term respiratory sequelae in patients with COVID-19 after ICU discharge. 25
Aiming to standardize pulmonary involvement in patients with COVID-19, the CT-SS was proposed to aid decision-making for hospital admission. This tool enables localization of lung involvement (parenchymal opacification of each region), but does not provide further information on functional and clinical parameters. The 13 ICF codes included in the ClinFIT COVID-19 for the acute phase provide a comprehensive functioning assessment, which is essential to determine an appropriate rehabilitation approach in this population. The ClinFIT COVID-19 was published in October 2021;13 however, to date, no study has evaluated this tool, clinically.
Regarding the other outcomes that we investigated, over one-third of our cohort reported moderate-to-severe musculoskeletal pain. This degree was lower compared with two previous studies, which reported a pain prevalence between 70% and 82.5% in COVID-19 patients,26,27 with a mean visual analog Scale (VAS) score of 4.8 (moderate pain). However, this symptom is poorly studied in people hospitalized with COVID-19 and appears to negatively affect functional recovery. 28 Our findings did not suggest a correlation between pain and other functioning categories; however, this might be because of the small number of people reporting this symptom. In our opinion, the severity and influence of pain on the clinical and functional status of COVID-19 patients should be properly investigated to provide the most appropriate management.
Strength and limitations
Our study is the first to use the ICF codes in the ClinFIT-COVID-19 in real practice in an acute care setting. The main limitation of our study is that the data related to the ICF codes were obtained retrospectively. Other limitations are the limited number of patients and the single-center design, which may affect the external validity of our results.
Conclusions
In inpatients with COVID-19, we demonstrated a correlation between clinical, instrumental, and functional parameters using the ICF categories. In particular, the codes within the ClinFIT COVID-19 may be used to detect functioning changes in patients with COVID-19, providing useful information to formulate an accurate prognosis.
Footnotes
Acknowledgements
The authors acknowledge the physiotherapists who contributed to the data collection; in particular: Paglierucci Fabrizio, Borriello Gerardo, Caiazzo Michele, Castaldo Gennaro, Della Corte Salvatore, Galasso Maurizio, Izzo Cristiana, Mastranzo Manuela, Pezzella Giuseppe, and Romanucci Umberto.
Author contributions
Authors AM, AB, and GI contributed to the conception and design of the paper; AM and FG contributed to the methodology; AM, SL, and MP performed the data analysis; MB, SL, and MP wrote the original draft of the manuscript; AM, GT, and FG reviewed the second draft of the manuscript; and AB and GI contributed to the study supervision. All authors contributed to manuscript revision and read and approved the submitted version.
Data availability statement
Data will be provided upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.