
Abstract
Introduction
Fragility hip fractures are associated with morbidity, disability, and mortality.1,2 It also has a significant impact on healthcare resources. Treatment for hip fractures in Asia has been estimated to cost almost 20% of the countries’ annual gross domestic product per capita. 3 It is predicted that by 2050, over half of all hip fractures will occur in Asia.3,4 Among the countries in this region, Malaysia is predicted to have the largest increase in hip fracture numbers by the year 2050. 4 Around 5800 hip fractures occur annually in Malaysia with the cost of treatment amounting to over USD35 million. 4 The number of hip fractures and the cost of treating them is estimated to increase by 3.5-fold in the next three decades to over 20,800 hip fractures annually costing USD125 million in direct treatment costs alone. 4
Hence, it is crucial for hip fracture treatment to be delivered effectively to optimize recovery, reduce disability, and minimize its associated complications. Orthogeriatric care, an inter-professional multidisciplinary collaboration, has been shown to be the most effective model of care for hip fracture treatment in hospital. 5 This model of care focuses on restoring function as soon as possible by ensuring early surgery (usually within 48 h of hospital admission) and early mobilization post-operatively. 6 Doing this has been shown to reduce hospital length of stay, inpatient, and long-term mortality.5,7,8 However, there have been barriers and challenges to its successful implementation. In Malaysia, the average waiting time from hospital admission to surgical fixation was 5 days and only around 20% were operated within the target of 48 h from presentation. 9 A lack of operating theater capacity, ongoing medical issues, patients on anticoagulation, and financial issues were reasons purported as reasons for the delay. 9 Time to mobilization post-operatively has never been reported in a local setting.
Due to a long time to surgery and uncertainty of how prompt mobilization occurs post-hip fracture surgery in the local setting, a service mapping process was performed to understand hip fracture management delivered in this hospital, a tertiary center. This study aimed to identify factors that would contribute to the delay in hip fracture surgery and early mobilization post-operatively.
Methods
Patients aged 65 years and over admitted to the orthopedic ward of a tertiary hospital in Malaysia from August 1, 2020 to October 31, 2020 with a fragility fracture of the hip were included in this study. This period was chosen because there was a downward trend in Covid-19 cases and resumption of routine orthopedic services. This hospital provides an orthogeriatric model of care. Patients with hip fractures are admitted to the orthopedic ward under the care of the trauma orthopedic team. They will also be reviewed by a geriatrician (consultant or specialist trainee) daily on weekdays during their inpatient stays to address any pre- and post-operative issues. Patients will then undergo surgery during the weekdays when clinical status allows and an operation theater slot is available. In our model of care, patients would be screened for delirium before and after operation routinely. The orthopedic ward has its own dedicated therapist who will review patients once an inpatient referral is made to them. Post-discharge, patients are routinely followed up in the orthopedic clinic unless this was deemed inappropriate by the clinical team, for example, short life expectancy, difficulty in transferring, or severe cognitive impairment. Outpatient therapy is arranged based on clinical needs.
Hospital electronic medical records were used to collect data retrospectively on barriers to early surgery, defined as 48 h from admission to the orthopedic ward, and early mobilization, defined as either the day of or the day after hip fracture surgery with documentation that the patient was sat at the edge of the bed. Change in mobility status at three-time points (pre-fracture, on discharge, and at 12 weeks (usual outpatient follow-up interval) after discharge based on documented clinical entry. Those not operated were excluded from this analysis. Data collection was performed in April–May 2021.
Descriptive analysis was performed for demographic data, comorbidities, acute medical conditions, and causes for surgical delay. Causes for the delay in surgery and mobilization were based on documentation in health records and categorized into groups determined at the start of the study. Barriers to early surgery were categorized and presented descriptively. Analyses were only performed on available data. Statistical significance was defined as a P-value of less than 0.05. All analyses were conducted using SPSS version 19. This study received approval from the institution’s research ethics committee (reference number MREC 2020722-8908).
Results
Patient characteristics
Fifty patients with hip fractures were admitted over these 3 months. Eight patients were subsequently excluded from further analysis. Four patients were managed conservatively, three patients were transferred to another hospital before surgery and one patient was admitted electively from the outpatient clinic for treatment. Of the 42 patients, 33 (78.6%) were female, had an average age of 78 years, frail, and half had at least two chronic diseases (Table 1). The most frequent surgery performed was hemiarthroplasty (19/42, 45.2%), followed by proximal femur nail (18/42, 42.8%).
Patient characteristics, n = 42.
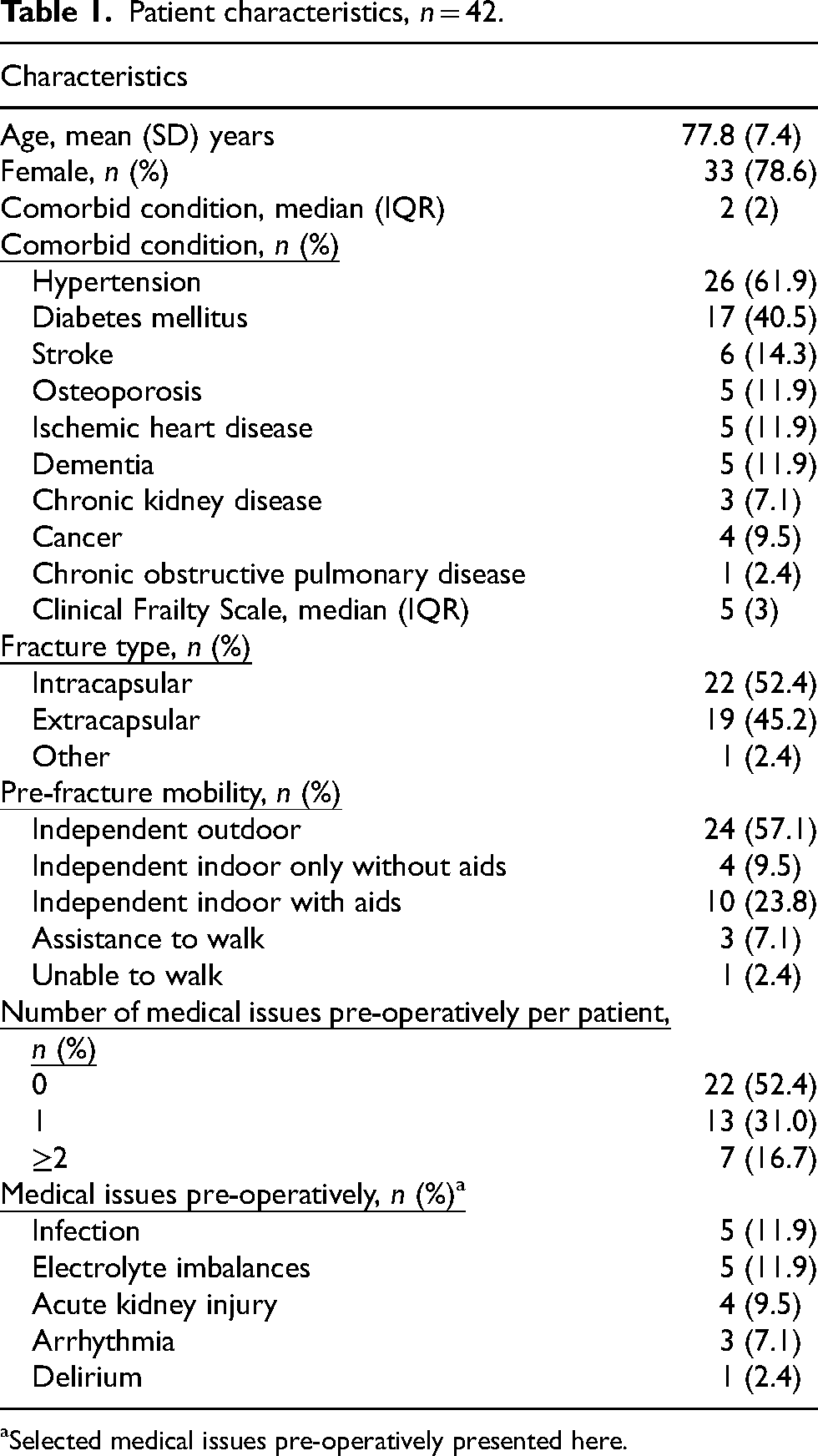
Selected medical issues pre-operatively presented here.
Ten patients (23.8%) had their surgery performed within 48 h of admission. The median (IQR) waiting time was 4 (3) days. The median (IQR) duration of hospitalization was 7 (4) days.
Pre-operative barriers
Prior to the operation, a median (IQR) of 1 (1) referral was made for each patient by the orthopedic team. This was in addition to the routine geriatric medicine and anesthetic assessments.
The most common referral was to cardiology services (18/42 patients, 42.9%). Indication for referral was not consistently documented in health records. The median (IQR) waiting time from referral to a review by the cardiology team was 16 (24) hours. Only six reviews were performed by either a cardiology consultant or a specialist cardiology trainee, with the rest by a junior doctor team member (medical officer). Of the 18 patients reviewed, 14 patients had only their peri-operative mortality and cardiac complication risk calculated (Revised Cardiac Risk Index) as part of surgical risk stratification assessment with no further direct change to the ongoing management plan. Nineteen patients had echocardiograms requested from different clinicians and performed pre-operatively. Only nine patients had an indication for the echocardiogram documented (six patients had non-specific electrocardiogram changes, one had a history of ischemic heart disease and two were noted to have murmur incidentally). The indication for the other echocardiograms was uncertain. 7/19 (36.8%) patients had it performed on the same day of the request. The median (IQR) waiting time for an echo was 43 (33) hours. 12 of 19 cases had echocardiograms performed more than 48 h after admission. No significant abnormalities were reported in all the echocardiograms performed, except for one patient who had reduced left ventricular ejection fraction, but no severe valvular pathology was encountered. This did not change the subsequent surgical and anesthesia management plan.
Other causes for surgery after 48 h from admission are detailed here (Table 2). Eleven cases with medical issues which required treatment prior to the surgery, were encountered.
Additional reasons for hip surgery >48 h from admission to the orthopedic ward (n = 32).
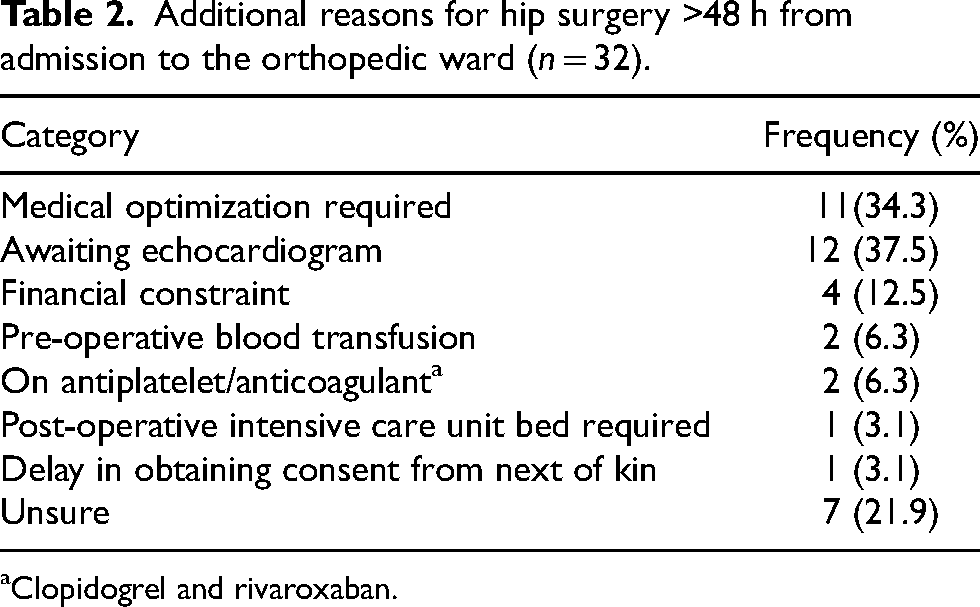
Clopidogrel and rivaroxaban.
Post-operative mobilization and rehabilitation
Patients spent a median (IQR) of 4 (2) days in hospital after their surgery. Post-operatively. 22/42 (52.4%) patients were reviewed by the physiotherapist either on the day of or the next day after surgery. Delayed physiotherapy review was due to the lack of a weekend service (11/20 patients, 55.0%) and delays in making the physiotherapy referral (4/20 patients, 20.0%). Among those reviewed early, only 9/22 (40.9%) patients were documented to be able to mobilize. Documented reasons that the 13 patients were unable to mobilize included uncontrolled pain (15.4%), hypotension (7.7%), anemia (15.4%), delirium (15.4%), and intensive care unit observation (7.7%).
On discharge, none of the patients were deemed able to walk independently without aid or supervision. Twenty-seven patients were referred for community physiotherapy but only 11 patients attended. The median (IQR) time from discharge to the first outpatient physiotherapy appointment was 35 (19) days. 3/11 patients only had a single visit within 12 weeks of discharge. Majority of cases (90.4%) had independent mobility either indoors or outdoors prior to their hip fracture. At 12 weeks post-surgery, data on their mobility status was available for 36 patients. The majority (31/36 patients, 86.1%) reported a deterioration in their mobility.
Discussion
Balancing between patients’ medical status, prompt surgical intervention, and early mobilization is key toward better outcomes for those with hip fractures. This process mapping exercise has highlighted this center's performance, and the barriers toward early surgical intervention and mobilization. The majority do not get operated within 48 h of their admission and post-operatively, most still struggle to be able to at least sit at the edge of the bed. There were several reasons for the delay in surgical fixation but the largest contributor to this was the need for an echocardiogram. The average wait from request to an echocardiogram was 2 days. This investigation did not lead to any change in management for this group of patients.
The average time post-surgery when patients could participate in inpatient rehabilitation was just four days. Actual days where rehabilitation could take place would be even shorter as half was seen 2 days after their operation. Even when patients were seen by the physiotherapist on either the day of or the day after their operation, less than half were able to mobilize. Patients’ mobility was restricted by pain, hypotension, anemia, and delirium. This study further highlighted the paucity of ongoing rehabilitation after operation and discharge. Hence, ways to ensure early and adequate rehabilitation should be considered before discharge.
This was the first time such an exercise was performed to identify the current level of hip fracture care in this hospital. All patients admitted with a hip fracture planned for surgery were included. With the service running at the usual capacity, albeit with COVID-19 precautions, it provided a useful indication of where the barriers to prompt treatment were. However, this study was performed in a single center, that is, a tertiary hospital in an urban setting of a middle-income country which does limit how well it relates to other centers. The number of patients included here was comparatively small, but deemed representative of the numbers expected for this center over a 3-month period. This study only focused on early surgery and mobilization and was unable to report on other aspects of hospital hip fracture care. The findings of this study also relied on information entered in electronic health records by healthcare team which would be dependent on its completeness and accuracy. Additionally, it was not able to assess data not captured in health records, such as information on the wider hospital system which would include theater space availability and staffing level.
The existing scientific literature has consistently confirmed patients benefit from early surgery. Surgical repair within 48 h was associated with improved survival, less complications, and potentially better function. 10 Early surgery has been incorporated into several national guidelines and clinical standards.11–15 In recent times, there has been emerging evidence that early mobilization post-hip fracture surgery is also associated with improved outcomes, such as a higher rate of discharge home, lower in-hospital, and 30-day mortality.7,8,16 Many of the barriers identified that delayed surgery and early mobilization were modifiable.
Almost half of the patients had a cardiology review and an echocardiogram. For many, the indication was uncertain, did not involve a senior cardiology practitioner, and when it was performed did not lead to a change in operative or anesthesia practice. Unnecessary pre-operative cardiology assessments and echocardiograms have been reported elsewhere.17,18 In one study, the authors quantified these excess requests to be almost 2.5 times more than would be recommended. 18 Introducing a pre-operative assessment pathway which details indications for cardiology input and echocardiography could help streamline this assessment.12,19 Utilizing existing routine geriatric medicine expertise to support this part of the assessment and risk assessment which patient would require specialist cardiology input will reduce this pre-operative burden and streamline the process. Many geriatric medicine specialists are already trained in peri-operative care involving older people. Besides that, many patients with hip fractures had a concomitant acute illness or a comorbid condition that required optimization pre-surgery. This would support the geriatrician's role in the pre-operative phase, working alongside other members of the multidisciplinary team to make individualized assessments with the patient on the risk and benefits of surgical fixation. Continuous national audits, such as those in the United Kingdom, Republic of Ireland, Australia, and New Zealand have demonstrated that it was possible to achieve early time to surgery and deliver real-world data on improved clinical outcomes. 20 This impact on overall hospital length of stay remains uncertain. A meta-analysis of orthogeriatric care's impact on inpatient stay did report a decrease of 1.5 days compared to services without a co-management model. 21 However, studies included in the meta-analysis were highly heterogeneous.
Generally, rehabilitation should be initiated as soon as the patient is clinically stable after surgery. Ensuring appropriate pre-operative care to minimize the risk of dehydration, hypotension, pain, and delirium would help the patients mobilize. These issues were identified as barriers to early mobilization in this center. This was similar to reasons identified in a large national audit in the UK specifically looking at mobilization after surgery. 22 From this audit, emphasis was placed on the role of the multidisciplinary team to support patients’ rehabilitation. Early mobilization was also recognized as a key quality indicator in hip fracture care.11,13,16 While in hospital, adequate multidisciplinary inpatient rehabilitation can confer better outcomes on patients’ long-term functional status. 22 Hence, professional societies, such as the UK's Chartered Society of Physiotherapists published recommendations for hip fracture rehabilitation covering frequency, intensity, and duration required post-surgery. 23 This study reported a 4-day period post-operatively. This short period of time was likely driven by bed pressures to ensure adequate bed capacity which is crucial to maintain patient flow. Hence, if the inpatient setting is unable to meet the required demand for rehabilitation, a more comprehensive outpatient rehabilitation program needs to be developed to support these patients’ recovery. However, there is a lack of post-acute facilities to support this initiative locally.
We acknowledge our limitations as single-center data with small sample size. However, we believe the 3 months study period was representative of our existing health services. Retrospective analysis of our electronic medical records also restricted our understanding of other systemic and organizational reasons such as availability of operation theater, manpower, and affordability of surgery by patients in our study. As this mapping process was only able to highlight service provision gaps, subsequent work has to now focus on identifying the factors associated with them and potential solutions to the problem.
Mapping the process of care is a good way of understanding the existing service being delivered with a view toward improving it. This study has demonstrated how an exercise like this forms the beginning of what is a quality improvement project. Dissemination of findings and stakeholder engagement is now required to plan areas of improvement, study the impact those changes would have had, consolidate it, and re-assess it again later on through regular clinical audits. This cycle of quality improvement is key if we want to deliver a service that is ready to manage the expected increase in hip fracture numbers over the coming decades.
Conclusions
This process mapping of hip fracture orthogeriatric care has identified several key areas which contributed to delays in surgical intervention and the start of the patient’s rehabilitation. These can be resolved by introducing pathways, consolidating multidisciplinary involvement, stakeholder engagement, and continuous audit.
Footnotes
Acknowledgments
The authors are grateful for the support provided by the Department of Orthopaedic Surgery and Patient Information Department.
Consent to participate
Patient consent was waived as this is a non-interventional retrospective study. We use routinely recorded hospital records. No additional participant data required beyond that. Consent to access these records provided by Research Ethics Committee.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and ap-proved by the University of Malaya Research Ethics Committee (MREC ID NO: 2020722-8908).
Presentation at meeting
Part of the study was presented as posters in 9th FFN Global Congress, 28–30 September 2021.