
Abstract
Introduction
Wide-awake local anaesthesia no tourniquet (WALANT) surgery was proposed by Dr Don Lalonde and popularized in the recent one to two decades. 1 Conventional knowledge believed that adrenaline use on digits could have risks of finger ischemia and necrosis. Many recent literatures suggested that adrenaline use in the fingers is safe, which is contradictory to conventional knowledge.2–4 WALANT surgery uses a mixture of lignocaine and adrenaline to infiltrate the surgical site and its surroundings to achieve a field of anaesthesia and hemostasis, sparing the use of tourniquet, regional and general anaesthesia. This technique can be applied to limb operations, including soft tissue surgeries and bone surgeries. Soft tissue surgeries consist of carpal tunnel release,5,6 A1 pulley finger release, 7 first extensor retinaculum release, 8 and ganglion excision9,10 while bone surgeries consist of distal radius plating,11–13 metacarpal fracture fixation, 14 olecranon fracture fixation, 15 and ankle fracture fixation. 14 There are many case series on the benefit of WALANT surgery, such as cost-efficiency.16–18 However, there is inadequate evidence based on the efficacy of WALANT surgery.
This is a prospective cohort The objective of this study is to investigate the differences in patient's pain perception, satisfaction and hemostasis control between two groups of patients, the WALANT group (patients who underwent WALANT surgery) and the traditional group (patients who underwent traditional local anaesthesia with tourniquet surgery) on limb operations in our locality. We hypothesized that WALANT was safe, produced less pain and good hemostasis, had a higher patient satisfaction and would be a better technique on limb operations.
Methods
The study was performed in a public hospital in Hong Kong from 1 January 2020 to 31 December 2020. The study protocol was approved by New Territories West Cluster Research Ethics Committee. All patients who underwent minor limb operations in a regional hospital day service centre were recruited. The limb operations at which the usual limb tourniquet could be applied to were included, such as trigger finger release, mass excision, ingrown toenail wedge resection and carpal tunnel release.
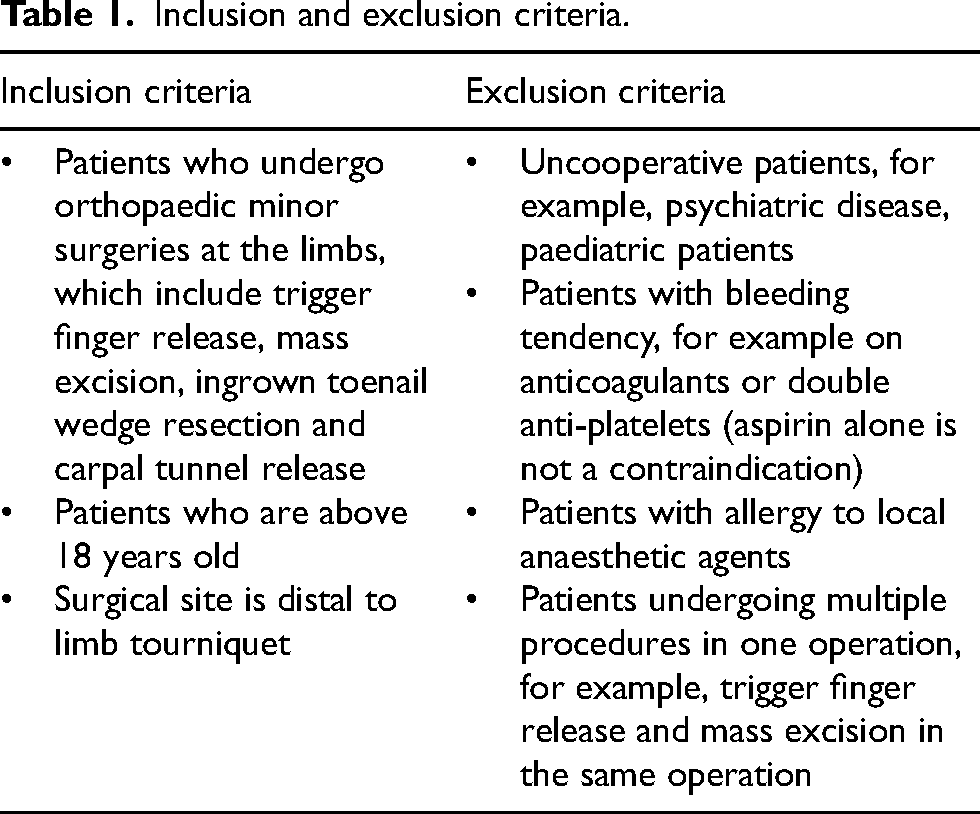
The inclusion and exclusion criteria are as follows (Table 1):
Inclusion and exclusion criteria.
The primary study outcomes are patient's pain perception at different time intervals (during LA injection, during operation, at least 1 h after operation), severity of tourniquet pain and patient's satisfaction. Pain was recorded with the Numeric Pain Rating Scale (0 no pain at all, 10 severe pain). Satisfaction would also be rated 0 to 10 (0 very dissatisfied, 10 very satisfied). Moreover, the secondary outcomes are operation time, hemostasis status and difficulty of operation, which were rated by the surgeon-in-charge. The surgeon would comment on the hemostasis status (1–3 good, 4–6 moderate, 7–10 poor) and the difficulty of the operation (1–3 easy, 4–6 average, 7–10 difficult) immediately after the surgery.
Informed consent (Appendix 1) was signed before operation. Our surgeons were divided into two groups: one group doing WALANT surgery and one group doing traditional local anaesthesia surgery with tourniquet use. Two groups of surgeons were randomly assigned to different surgery sessions, except carpal tunnel release, as this surgery would be performed or supervised by hand specialists mainly, who are the WALANT group surgeons. Patient was blinded to group allocation because patients were informed of the two possible techniques but did not know the technique to be used prior to surgery. The WALANT group surgeon performed operations largely following the WALANT technique suggested by Dr Don Lalonde (Figure 1) while the traditional group surgeon applied an arm tourniquet. There were standby precautions for adverse drug reactions. Phentolamine 1 mg in 1 ml would be applied by local injection for the reversal of vasoconstriction in case of digital ischemia. Equipment for cardiopulmonary resuscitation was prepared for local anaesthetic systemic toxicity and benzodiazepines were prepared for seizure.
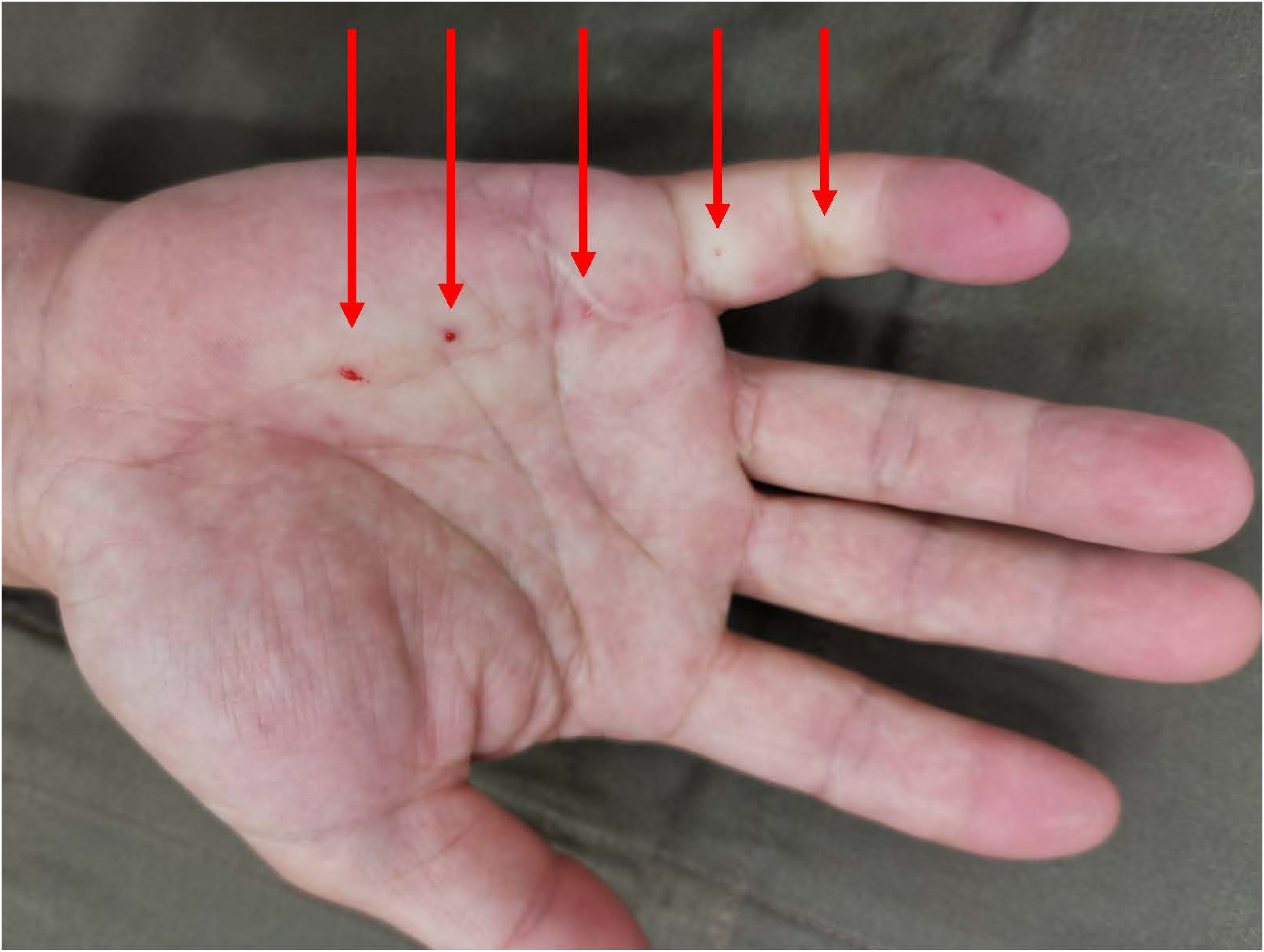
This photo shows a patient undergoing WALANT technique. There are multiple blanching injection sites along the palm and little finger due to adrenaline vasoconstriction.
WALANT technique
For the WALANT group, we used the WALANT technique to minimize pain and provide a bloodless surgical field. The anaesthetic agent was a mixture of lignocaine and adrenaline with or without buffering. It was warmed to room temperature. A small needle 25/27 gauge was used. The injection started proximally and worked distally. The first injection site was touched or pressured or pinched to distract injection pain. The mixture was injected perpendicularly to the subcutaneous layer slowly. The surgical sites would look swollen and firm when the adequate volume is given and they would look blanched when adequate time is given. Then each subsequent LA mixture was injected within 1 cm of the blanched area. These blanched areas provided anaesthetic surgical fields. Figure 1 showed the clinical photo of the right hand after applying the WALANT technique over the right little finger with arrows showing the injection sites.
Power analysis was performed to ensure the sample size was enough. The study data were recorded in the questionnaires. All data were entered into a database and analysed with Statistical Product and Service Solutions Version 26. Demographics were analysed by Chi-square test. Primary and secondary outcomes were continuous ordinal data. Shapiro–Wilk test showed all continuous ordinal data were non-parametric. Mann–Whitney U test was used for data analysis. Data were summarized as frequency and percentage for categorical nominal data, and first, second and third quartiles for continuous ordinal data. A p-value of less than 0.05 was taken as statistically significant.
Results
A total of 143 patients were recruited. Eighteen patients were excluded: one was shoulder surgery, which was not feasible for WALANT surgery. Six operations consisted of two or more procedures, and 11 questionnaires had incomplete study data. The study flow chart was illustrated in Figure 2.
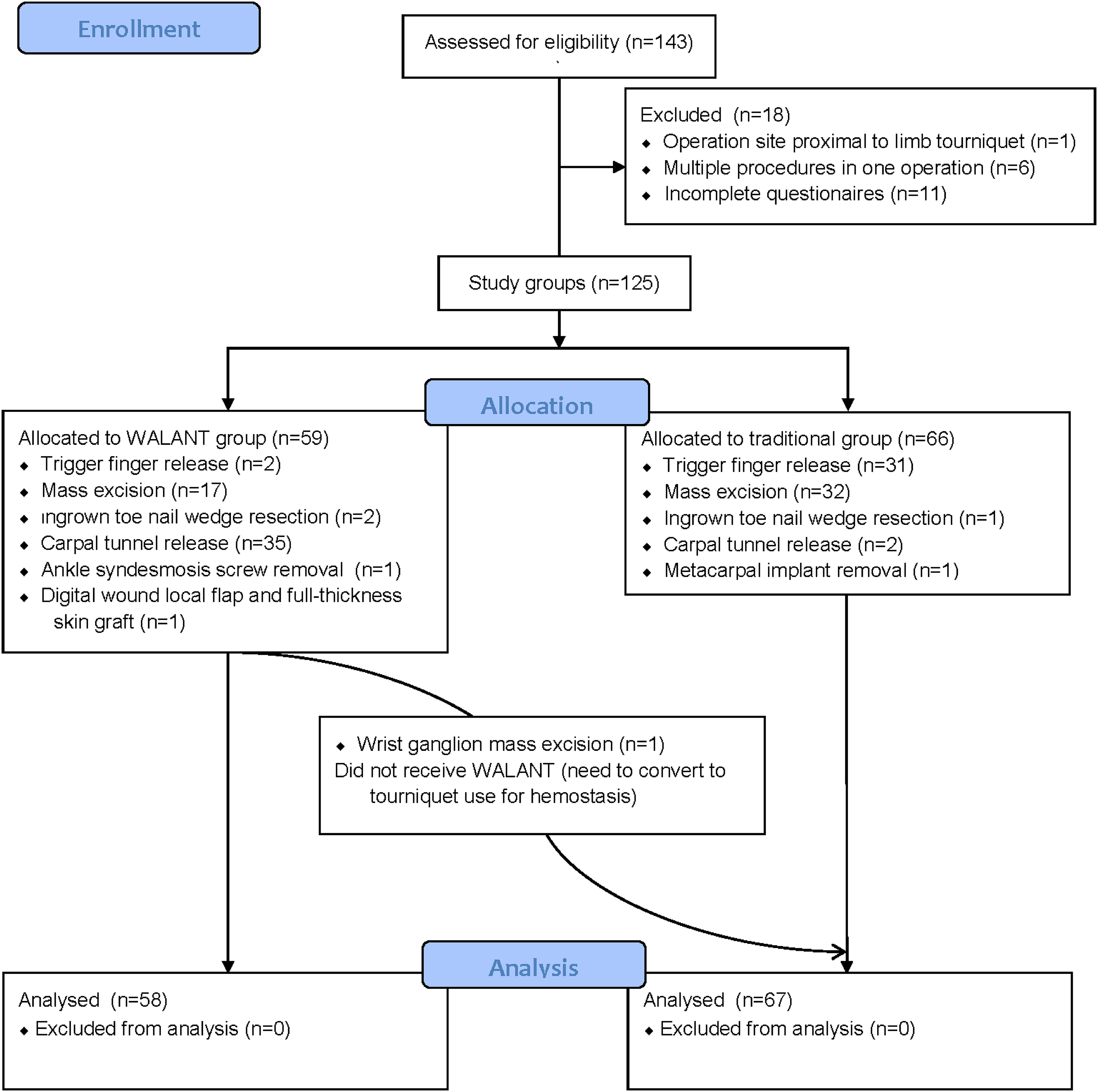
The diagram illustrates the flow of the study.
Demographic data, types of operations, surgeon experience and study outcomes between the WALANT group and traditional group are stated in Tables 2–5.
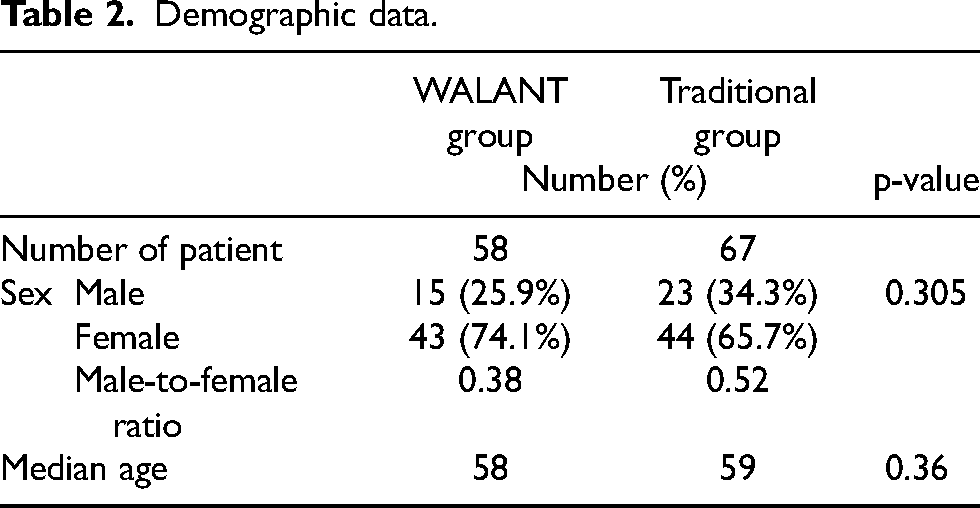
Demographic data.
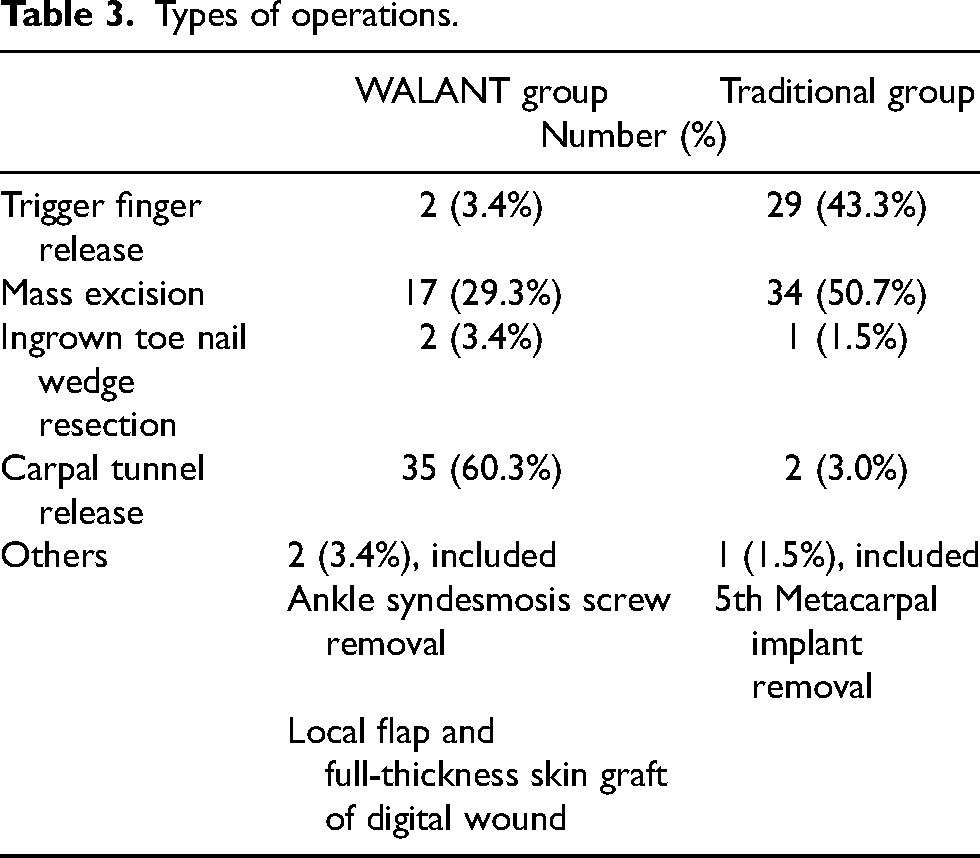
Types of operations.
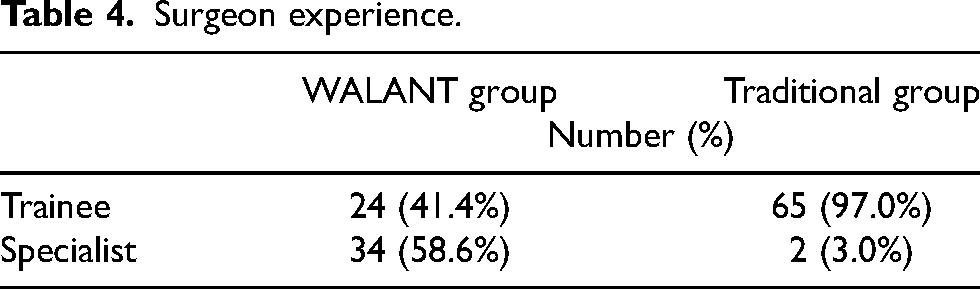
Surgeon experience.
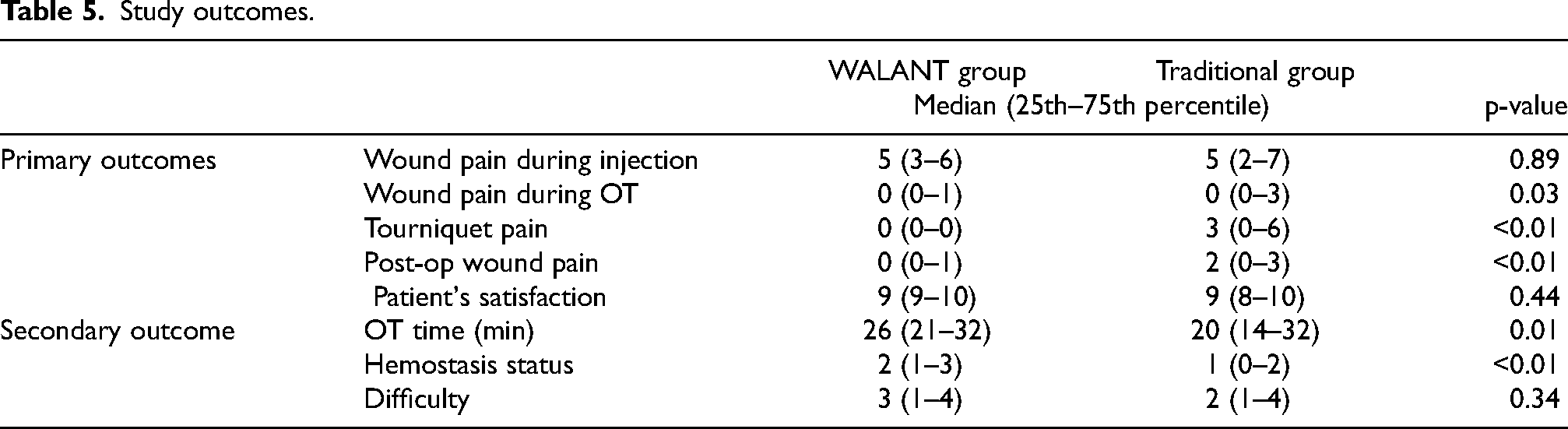
Study outcomes.
Fifty-eight WALANT group patients and 67 traditional group patients were studied. Male-to-female ratios in the WALANT group and the traditional group were 0.38 and 0.52, respectively. The mean ages in the WALANT group and traditional group were 59 and 56, respectively (Table 2). The majority of operation types in the WALANT group were carpal tunnel release (60.3%) while those in the traditional group were mass excision (47.8%) and trigger finger release (46.2%) (Table 3). Moreover, 58.6% of the WALANT group was performed by a specialist while 3.0% of the traditional group was performed by a specialist (Table 4).
In primary outcomes, the difference in pain during injection between both WALANT and traditional groups is similar with a median pain score of 5 (p = 0.89). Both the WALANT and traditional groups had a median wound pain score of 0 (p = 0.03) during surgery, which implied adequate analgesics were given to both groups. However, the traditional group had a median tourniquet pain score of 3 (p < 0.01), while the WALANT group did not apply a tourniquet and thus no pain. WALANT patients scored less post-operative pain with a median score of 0 compared with 2 (p < 0.01) for the traditional group patients. Patient satisfaction was similar with a median of 9 (p = 0.44) in both groups (Table 5, Figure 3).
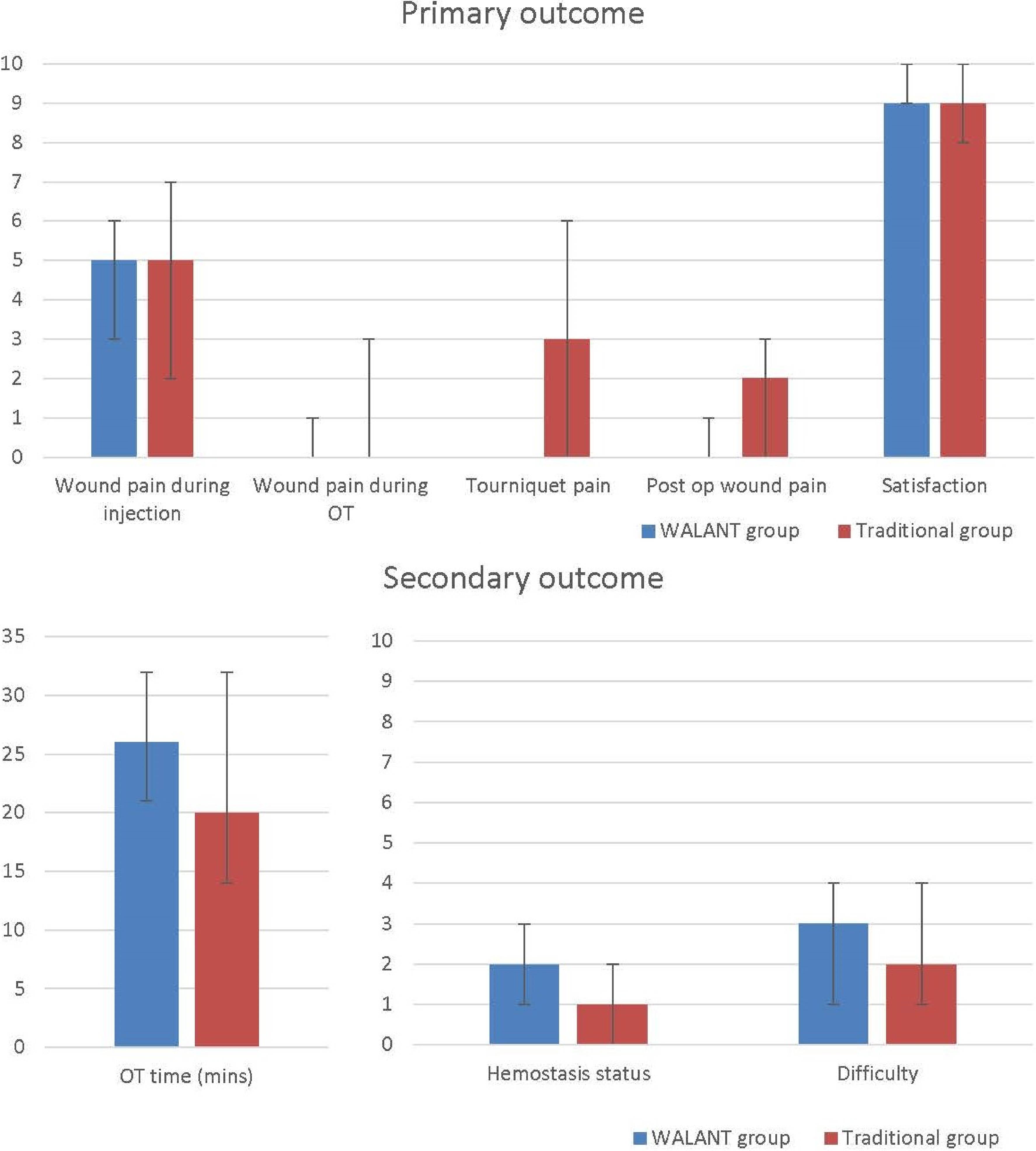
The graphs show median of primary and secondary outcomes, respectively, between WALANT surgery and LA surgery with tourniquet use for limb operations. Value of the positive error bar is 75th percentile while that of the negative error bar is 25th percentile.
In secondary outcomes, the median operation time was 6 min longer in the WALANT group, which was statistically significant (p = 0.002). Both groups could achieve good hemostasis with a median score of 2 and 1, respectively (p < 0.01) and easy operation with a median score of 3 and 2, respectively (p = 0.34) (Table 5, Figure 4).
There was no adverse drug reaction, digital ischemic, seizure or local anaesthesia systemic toxicity reported in this study.
Discussion
Our study aimed to study the WALANT technique's anaesthetic effect and its feasibility. We compared the WALANT and traditional groups by the difference of pain, patient satisfaction, hemostasis, operation difficulty, length of operation time and safety.
Pain during injection
Pain during injection between the two groups was similar (p = 0.844). The result of the comparison of injection pain between the WALANT and traditional groups was not statistically significant because there was a wide variety of injection techniques within the WALANT group. Our study had not standardized the application of injection techniques described by Dr Donald Lalonde 19 (Figure 1), for example, the size of the injection needle and the distraction manoeuvre on the first injection. In our study, the surgeon-in-charge decided on the injection technique to be used, which depended on the nature of the surgical procedure and the surgeon's preference.
Wound pain and tourniquet pain during surgery
The traditional group had tourniquet pain with a median pain score of 3 in our study. In fact, tourniquet pain during surgery is well established in many literatures. Maury et al. 20 conducted a prospective, randomized, controlled trial on tourniquet tolerance in 24 fit, healthy volunteers and suggested mean tolerance for the upper arm tourniquet was 18 min. Whereas, Hagenouw et al. 21 suggested the average duration of tourniquet pain tolerance was 31 min. Hence, if the expected operation time is longer than 18 to 30 min, WALANT surgery may be superior as patients are spared from tourniquet pain.
Post-operative pain
WALANT patients scored less post-operative pain. Adrenaline causes vasoconstriction, which allows local anaesthesia to remain at the surgical site longer. It also reduces systemic absorption, allowing a larger dose of local anaesthesia to be used safely. The residual effect and less dosage restriction of LA used in WALANT surgery can lead to better post-operative pain control. On the other hand, tourniquet release induces metabolic hyperaemia and vasodilation. This reperfusion causes pain and also lowers LA concentration, and thus minimal LA is retained in the surgical field. This result was compatible with Lee's 8 and Evangelista's study. 22 Lee conducted a randomized controlled trial of minor hand surgeries comparing wide-awake local anaesthesia with no tourniquet and local anaesthesia with a tourniquet. The WALANT group had longer anaesthetic duration and less post-operative pain than the conventional group. Our studies have proved that WALANT surgery can reduce patients’ post-operative pain.
Hemostasis status and operation difficulty
Both WALANT and traditional groups could achieve good hemostasis and easy operation. Only one patient who underwent right wrist ganglion mass excision needed to convert from WALANT surgery to a tourniquet for hemostasis.
The hemostasis in the WALANT group could be achieved better by allowing adequate time for the adrenaline to cause vasoconstriction. Daniel E McKee 23 suggested the optimal time between injection and incision was 25 min. To further improve our study, a standardized injection to skin time interval should be proposed.
Operation time
The median operation time was 6 min longer in the WALANT group (p = 0.002). Firstly, in the WALANT group, some surgeons would give a local anaesthesia mixture in multiple injections and need more time for the adrenaline to achieve vasoconstriction. Secondly, more time was allowed to achieve meticulous hemostasis. Thirdly, no tourniquet use in the WALANT group means that the operation time is not restricted by the patient's intolerable tourniquet pain. It gives the surgeon a more comfortable window of time to operate and achieve a better surgical outcome.
Safety
In both groups, there was no adverse drug reaction, digital ischemic, seizure or local anaesthesia systemic toxicity reported. Moreover, 82% of surgeons in the traditional group used tourniquets for hemostasis because of routine use. In fact, many literatures2–4 supported that the use of adrenaline on digits was safe. The digital loss before 1950 was proven to be not related to adrenaline. 24 Before 1950, procaine was the only injectable local anaesthetic agents. There were no expiry dates on local anaesthetic agents. Prolonged storage would acidify procaine and result in digital ischemia. Our routine practice of checking expiry dates before drug administration ensures LA safety use.
Patient satisfaction
Both the WALANT and traditional groups had the same median satisfaction score of 9, but it was statistically insignificant. Many factors could affect a patient's satisfaction, for example, pain perception, the impression of their surgeons and immediate patient-perceived surgical outcomes.
Limitations
As WALANT surgery was a newer technique which was mainly performed by specialists in our centre, surgeon allocation between the two groups was uneven. Varying surgeon experience also created interobserver bias as hemostasis status and operation difficulty were subjectively rated by different surgeons.
In addition, adrenaline usually takes time to achieve good hemostasis. The hemostasis effect and operation time might be better reflected if a standardized duration between adrenaline injection and the start of the operation is used.
Conclusion
In our cohort study, it was shown that WALANT surgery was safe and could achieve good hemostasis with no limitation of tourniquet time, and significantly reduce post-operative pain compared with traditional local anaesthesia with tourniquet use. With the benefit of no general anaesthesia (GA) risks and availability for day surgery, we proposed to extend the application of the WALANT technique on limb operations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.