
Abstract
Background:
Trigger finger release utilizing wide-awake local anesthesia no tourniquet (WALANT) usage in extremity surgery is not widely used in our setting due to the possibility of necrosis. Usage of a tourniquet is generally acceptable for providing surgical field hemostasis. We evaluate hemostasis score, surgical field visibility, onset and duration of anesthesia, pain score, and the duration of surgery and potential side effects of WALANT.
Methods:
Eighty-six patients scheduled for trigger finger release between July 2016 and December 2017 were randomized into a control group (1% lignocaine and 8.4% sodium bicarbonate with arm tourniquet; given 10 min prior to procedure) and an intervention group (1% lignocaine, 1:100,000 of adrenaline and 8.4% sodium bicarbonate; given 30 min prior to procedure), with a total of 4 ml of solution injected around the A1 pulley. The onset of anesthesia and pain score upon injection of the first 1 ml were recorded. After the procedure, the surgeon rated for the hemostasis score (1–10: 1 as no bleeding and 10 being profuse bleeding). Duration of surgery and return of sensation were recorded.
Results:
Hemostasis score was grouped into visibility score as 1–3: good, 4–6: moderate, and 7–10: poor. The intervention group (with adrenaline) had a 74% of good surgical field visibility compared to 44% from the controlled group (without adrenaline; p < 0.05). Duration of anesthesia was longer in the intervention group (with adrenaline), with a 2.77-h difference.
Conclusion:
WALANT provides excellent surgical field visibility and is safe and on par with conventional methods but without the usage of a tourniquet and its associated discomfort.
Introduction
A tourniquet is an essential tool for providing a bloodless surgical field. There are different types of tourniquets all aiming to provide better tolerance and fewer complications. When a surgical operation requires prolonged usage of a tourniquet, discomfort of the patient is a major issue, resulting in the utilization of sedation or general anesthesia.
Lately, the usage of adrenaline is gaining popularity. Wide-awake local anesthesia no tourniquet (WALANT) technique with the combination of common drugs, pioneered over the last decade, has seen excellent outcomes. It has various significant advantages, namely, faster operating time, ability to visualize functional repair of bone and soft tissue while providing adequate tension for tendon repair as well as discarding the tourniquet in hand surgery together with its associated complications. 1 It also provides rapid patient turnover without the need for general anesthesia, thus becoming cost-effective and economical. 2
The biggest detractor for WALANT is the taboo created using adrenaline in digits, which is believed to cause gangrene of the extremities due to its vasoconstrictor effects. Fitzcharles-Bowe et al. reviewed extensive literature between 1990 and 2005 and reported that none of the 59 patients who received an injection of high-dose epinephrine (1:1000) reported finger necrosis. 3 In another prospective study by Lalonde et al. involving 3110 patients, none of the patients reported skin necrosis. 4 These two studies started the new debacle regarding the safety of adrenaline usage in extremities. Gunasagaran et al. concluded that none of their patients developed digital necrosis post-WALANT, while attributed tourniquet pain was the main cause of discomfort. The study, however, involved different procedures on a variety of cases such as carpal tunnel, trigger finger, and ganglion. 5
Trigger finger is one of the commonest hand case presentations to the orthopedic clinic. Demographically it represents 2.2% of the adult populations aged 30 years and older. 6 It is more common in women in their fifth and sixth decades compared to men. 7 Symptoms may vary from pain upon movement of the digits to demonstrable locking. At the extreme end, this will interfere with the normal day-to-day activity. 8 This cumbersome disease, a result of narrowing of the canal at A1 pulley of flexor tendon of the hand, can be caused by external or internal factors. Thickened A1 pulley or inflammation over the flexor tendon is one of the main reasons. 9 Treatment varies from night splinting and activity modifications with analgesia or surgical release of A1 pulley for those who failed conservative treatment. 10,11
The usual practice is to perform trigger release surgery with a tourniquet for a better surgical field and, subsequently, proper A1 pulley released. 12 Usage of tourniquet causes intraoperative pain to patients; hence, with this new practice where a tourniquet is not required, one can be more comfortable doing the surgery without the risks and pain of tourniquet, resulting in a better patient experience. 5,13
To the best of our knowledge, there is no prospective study of WALANT on just trigger finger release only. Our main objective is to assess the effectiveness of WALANT in terms of surgical field visibility in comparison with the conventional method in trigger finger release. Additionally, we also analyzed the effects of anesthesia by means of onset and duration, pain upon injection of the solution, ease of surgery, and the presence of digital necrosis
Methodology
We obtained ethical committee approval from our university (JEP-2016-305). We enrolled 86 consecutive cases of trigger finger release between July 2016 and December 2017. Both the control and the intervention groups were randomized. The balloting technique was utilized for randomization with even and odd numbers. Control group was assigned with even numbers and odd numbers to the intervention group. Local anesthesia of lignocaine and tourniquet was defined as the control group, while local anesthesia of lignocaine and adrenaline without tourniquet (WALANT) comprised the intervention group. Inclusion criteria included patients who are above 18 years old and planned for surgery. Exclusion criteria were patients with peripheral vascular disease (PVD), diabetes mellitus, ischemic heart disease, and known allergy to lignocaine or adrenaline.
The patient was brought to the treatment room in a day-care setting. In the intervention group, we used a mixture of lignocaine 1% with adrenaline 1:100,000 and 1 ml of 8.4% sodium bicarbonate. The injection was given 30 min prior to the procedure in the treatment room in the day-care surgery complex. In the control group, we used a mixture of lignocaine 1% and 1 ml of 8.4% sodium bicarbonate. An arm tourniquet was applied. The tourniquet pressure was set to 100 mmHg above the systolic pressure. We did not use an Esmarch bandage for exsanguination as the surgery is considered minor with minimal bleeding. The limb was kept in an elevated position for 1 min. The injection was given in the operation theater 10 min prior to the procedure. For both groups, skin preparation was done with an alcohol swab, and a 26-gauge needle was injected 90° perpendicularly just over the palpable A1 pulley by the researcher. One milliliter of anesthesia was injected over the A1 pulley region. Following this, a 26-gauge needle was used to gently prick the pulp of the finger until the patient did not feel the sharp sensation anymore. This is considered as the onset of anesthesia. The needle position is checked whether it was in the tendon by asking the patient to move the respective finger. The pain score upon injection of the solution was recorded using a visual analogue scale (VAS) score of 0–10. The surgeon is required to provide a hemostasis score (1–10: 1 as minimal bleeding and 10 as profuse bleeding), and the surgery duration was recorded. The surgeons were not blinded in the study. The duration of anesthesia, defined as the return of the tip of the finger to normal sensation, was assessed using a charting method given to the patient to record on an hourly basis. Patients were then contacted at 5 p.m. on the same day to enquire on their sensation over the finger. All patients were reviewed on day 5 postoperatively to assess any complications.
Mean and the standard deviation were used for standard data tabulation for numerical data, whereas percentage and frequency were used for categorical data. Independent t-test was used for continuous variables, while χ 2 test was used for categorical variables for correlation. A p value of <0.05 was considered significant. All data were analyzed using statistical application R version 3.4.3.
Statement of informed consent
Informed consent obtained from all individual participants was included in the study.
Statement of human and animal rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Results
There were 86 patients in the study, of which females accounted for 69% (n = 59) while males 31% (n = 27). Demographically, the age group of 55–65 corresponds to the highest percentage at 43% (n = 36), while the youngest age-group of 35–45 contributed to the lowest percentage at 3% (n = 3). Most of them were Malay participants at 60% (n = 52), Chinese at 33% (n = 33), and Indians at 7% (n = 6; Figure 1). Trigger thumb was the most common presentation for the intervention group (n = 16 at 37%), while the control group involved the ring finger (n = 13 at 30%; Table 1).

Bar graph indicates demographic distribution in the study population.
Baseline characteristicsa

WALANT: wide-awake local anesthesia no tourniquet.
aIntervention: WALANT with adrenaline; control: local anesthesia without adrenaline with arm tourniquet.
IF: index finger; LF: little finger; MF: middle finger; RF: ring finger; TF: thumb.
In terms of hemostasis score (rated from 1–10: 10 being profuse bleeding by the surgeon), the intervention group showed the highest frequency at scores 2 and 3 with a median score of 3, whereas in the control group, the data were more broadly distributed from scores 1 to 9 (Figure 2). Based on the hemostasis score, the surgical field visibilities grouped into good (1–3), moderate (4–6), and poor (7–10). In the intervention group, usage of adrenaline provided the highest percentage of good visibility at 74% (n = 32) as opposed to 44% (n = 19) in the control group (Figure 3). Multivariable analysis showed the odds of scoring moderate to poor visibility score from good visibility score reduced by 78% after all other variables held constant. These differences were statistically significant (p = 0.013; Table 2).
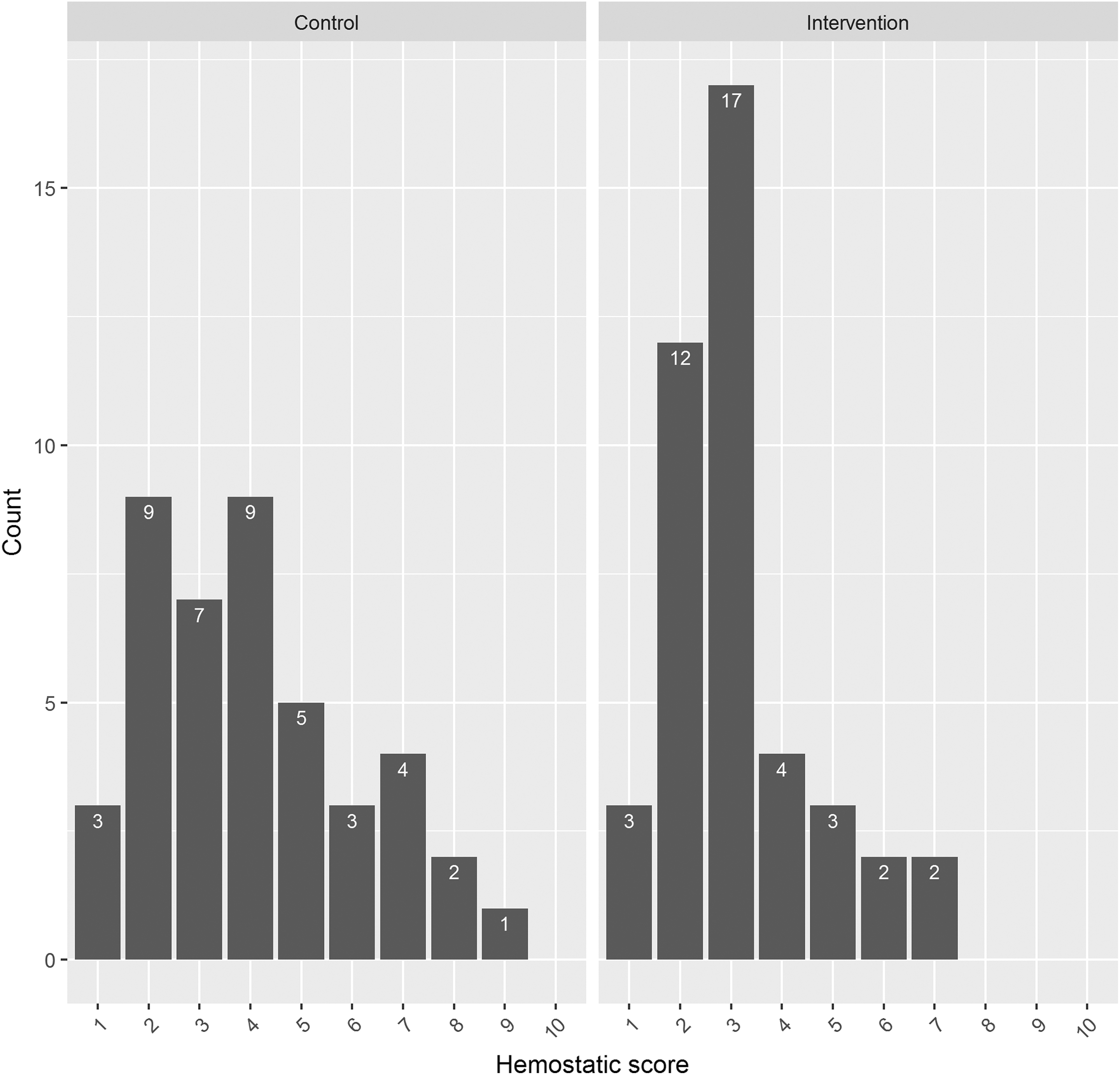
Bar graph showing data distribution in hemostasis score. Intervention: WALANT with adrenaline; control: local anesthesia without adrenaline with arm tourniquet. WALANT: wide-awake local anesthesia no tourniquet.
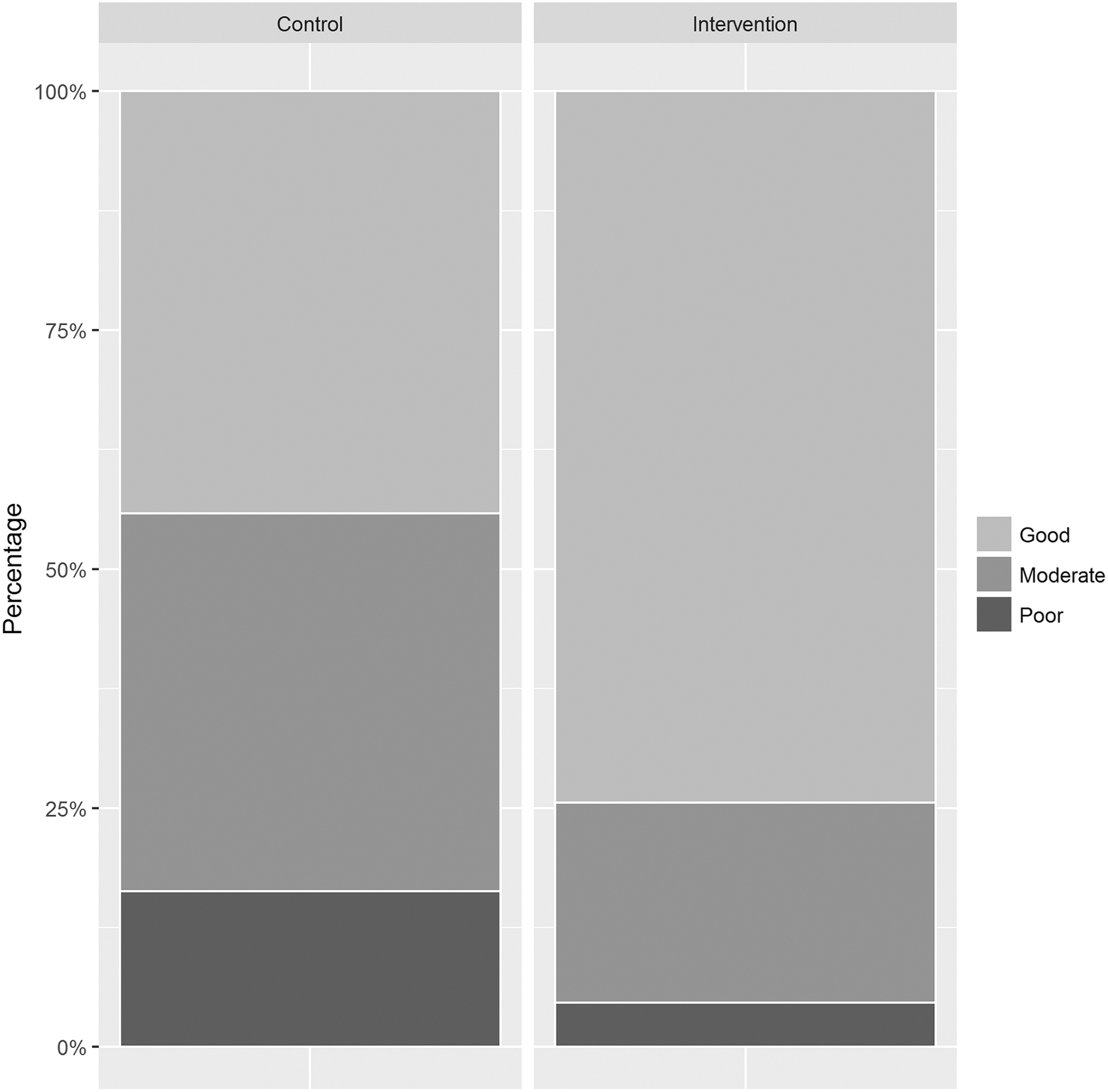
Hemostasis score was grouped into surgical visibility score; good (1–3), moderate (4–6), and poor (7–10) with *p = 0.013. p Value was calculated using the χ 2 test. *p < 0.05: statistically significant.
Multivariate analysis for the intervention groupa
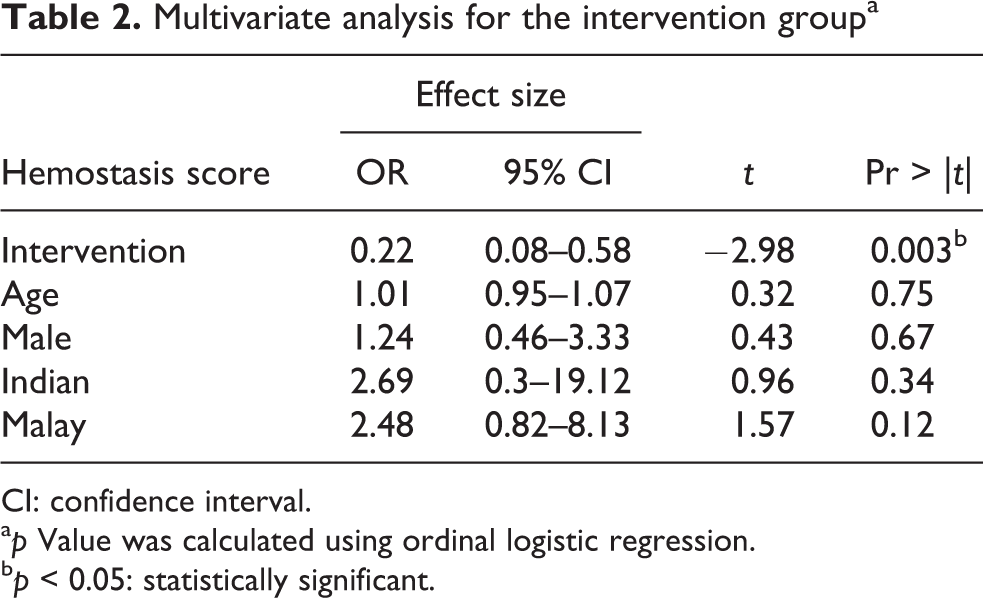
CI: confidence interval.
a p Value was calculated using ordinal logistic regression.
b p < 0.05: statistically significant.
The onset of anesthesia was 85.16 s for the intervention group compared to 102.07 s for the control group. This was not statistically significant (p = 0.204; Table 3). However, the duration of anesthesia (return of sensation) recorded a difference of 2.77 h, 6.86 h for the intervention group and 4.09 h for the control group (p < 0.001; Figure 4).
Comparison of intervention and control group in other variablesa

SD: standard deviation.
a p Value was calculated using the independent t-test (equal variance).
b p < 0.05: statistically significant.
s: second; h: hour.
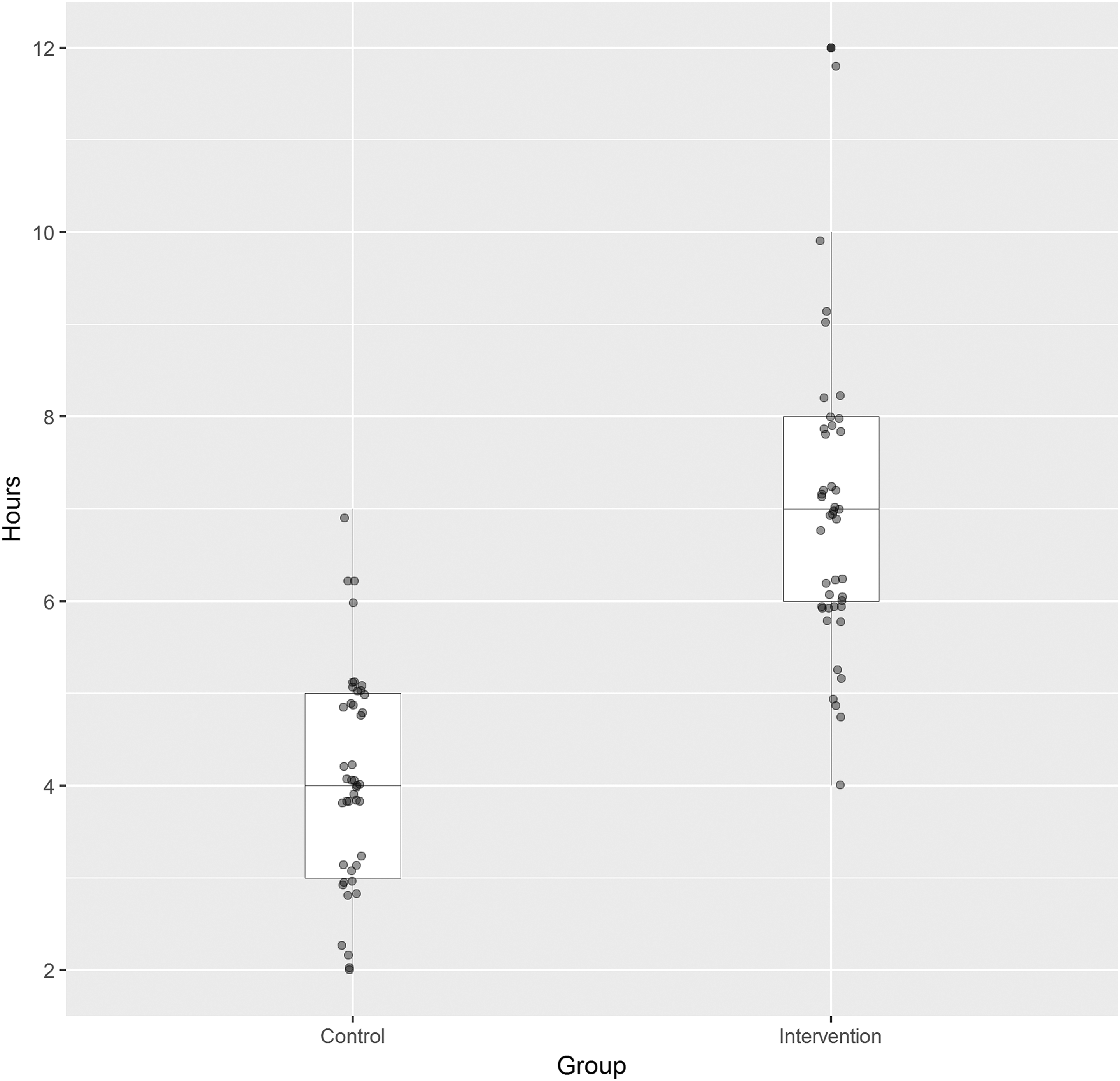
Duration of anesthesia (return of sensation) is presented using a box-plot graph. Control group ranging from 2 h to 7 h, while 4–12 h in the intervention group with *p < 0.001. p Value was calculated using the independent t-test (equal variance). *p < 0.05: statistically significant.
Despite the perceived better surgical visual field, the duration of surgery was not statistically significant as both intervention and control groups showed a minimal difference at 20.33 minand 19.65 min, respectively (p = 0.671; Table 3).
The mean pain score for the intervention group was 4.88 while 5.3 in the control group, which was not statistically significant (p = 0.385; Table 3).
Local anesthesia given was adequate for both groups, with no intraoperative additional injection given. No patient required deflation of tourniquet. There was no evidence of digital skin blanch or necrosis in our study. All patients recovered well without postoperative complications.
Discussion
Hemostasis is fundamental in any surgery, especially in hand surgery with small and delicate structures. It is traditionally achieved using an arm tourniquet. This, however, can result in an unpleasant experience for the patient during the procedure. 5,13,14 Ralte et al. concluded in their study that patients experienced more discomfort during open carpal tunnel release in the tourniquet-applied group. 13 Meanwhile, Gunasagaran et al. reported that the tourniquet was the main cause of discomfort in their study, which comprised multiple hand pathologies as well as attributing no difference in blood loss between WALANT and the conventional method. 5
On the other hand, tourniquet tolerance can vary between individuals. Maury et al. found that the mean arm tourniquet tolerance was 18 min (range 10–26), while Hagenouw et al. reported a tolerance of up to 31 min. 15,16
Meanwhile, according to Yousif et al., patients were able to tolerate tourniquet less than 30 min without medications. 17 It should be made clear that tolerance is the maximal time of tolerable discomfort or pain. Despite multiple studies, showing longer tolerance time compared to the surgical procedure, many patients were subjected to pain throughout the inflation of tourniquet. These studies do not consider those patients who are embarrassed to inform their surgeons of their discomfort or those who are willing to tolerate discomfort just so that their condition, that is, trigger finger, is resolved. Nevertheless, none of our patients required deflation of the tourniquet during the procedure. Our study showed a significant advantage in the WALANT group as it provides better surgical visual field with 74% (n = 32) in a good visibility group as compared to only 44% (n = 19) in the control group. The result was markedly favorable with the usage of adrenaline. We did not use an Esmarch tourniquet for exsanguination of blood, as this is not the common practice in our center for trigger release. Trigger release is considered a minor procedure with minimal or no bleeding. Additionally, the usage of an Esmarch bandage has potential adverse effects such as massive pulmonary embolism and excessive soft tissue compression (>1000 mmHg). 18,19 We utilized a hemostasis score as a measure of intraoperative blood loss as it was difficult to gauge very small amounts of blood loss. Nevertheless, the Esmarch tourniquet may be utilized if the center commonly uses it as it will improve the surgical field. A further study comparing the use of Esmarch tourniquet in WALANT surgery may be useful.
The timing of injection given is paramount for successful WALANT. Ruxasagulwong et al. in their study favored the conventional group as compared to the WALANT group, although there was more blood loss in the former. 20 It was not described in the study on when WALANT was given. McKee et al. recommended adrenaline injection to be given at least 26 min prior to the surgery for optimal vasoconstriction. 21 The preparation time (mixing WALANT components) was just marginally longer by 1 or 2 min (where we added one vial of lignocaine and dilute it with normal saline), and the injection was given about 30 min in the treatment room prior to operation theatre (OT) arrangements (attire changing namely), thus saving time while waiting for optimal vasoconstriction. We certainly found it more convenient to give all the WALANT injections all at once very early on before commencement of the day-care list as we spend time communicating gently with the patients and reducing any fear and anxiety in a relaxed section of the day-care area rather than injecting local anesthesia on the operating table when patients are more anxious. However, in centers where WALANT is not allowed to be administered outside the operation theater, either a special section in the operation theater itself can be allocated for the injection to be given or the first case can be done under conventional anesthesia to allow optimal time of WALANT for vasoconstrictive effect to take place. Therefore, this would be a limitation in certain centers. We are of the opinion that administering WALANT is not a complicated procedure and can be easily done in any section of a daycare center.
Usage of a tourniquet also leads to complications such as neurovascular injury, deep vein thrombosis, and skin damages. 22,23 Usage of WALANT removes the potential side effects of a tourniquet and greatly improves patients’ surgical experience. In 2004, Altinyazar et al. conducted a study to evaluate the extent of the vasoconstrictive effect of adrenaline and discovered biphasic blood flow returned within 90 min. 24 This would be equal to the recommended time for tourniquet deflation, especially in more complex surgery. 22 The advantage of WALANT here is the possibility of “topping up” to provide further bloodless surgical field, without having to wait for reperfusion time.
In terms of providing duration anesthesia effects, our study showed a large difference of 2.77 h. Unsurprisingly, adrenaline provided local vasoconstriction and prolonged the effect of lignocaine. Our WALANT outcome of 6.86-h anesthesia was more than the average of 2-h duration which can go up to 5 h. 25,26 However, Thomson et al. reported 10.9-h average anesthesia time, when using a mixture of 2% lidocaine with adrenaline 1:100,000 compared to our 1% solution lidocaine. 27 There is a possibility of recall bias as some of our patients were discharged early and provided with a card to document their return of sensation. We then followed up the patients retrospectively to retrieve the data. Many of the patients in the WALANT group preferred the longer duration of anesthesia and felt more comfortable at home. Although it would be ideal to admit the patients and monitor on our own, it was not cost-effective and would further burden the patients. Prolonged period of anesthesia also has its own disadvantage. In 2003, Bergman et al. reported that one patient developed pressure sores from compressive bandage, in his 405-brachial plexus block series. 28 Although our WALANT only lasted for an average of 6 h, patients need to be well informed on the effects of prolonged anesthesia (local and systemic) and to observe color and capillary refill time of their respective fingers.
There are also studies reporting on the adverse effects of adrenaline usage in extremities. Thomson et al. in his review attributed 21 cases of digital infarction with the usage of procaine and adrenaline due to the acidity of procaine itself. The cases were recorded mostly pre-1950s. 29 There have been five cases of digital necrosis with the usage of lignocaine and adrenaline reported between 2012 and 2017. 30 –34 All patients were given adrenaline 1:100,000, except in one case where it was not mentioned. Phentolamine, a potent α-blocker, was given to one patient, which reversed the adrenaline vasoconstrictive effect. Various factors, such as undiagnosed PVD, intra-tendinous, and high-volume injections, attributed in these cases. In our setting, injection was given subcutaneously and movement of the respective digit was checked to ensure it was not in the tendon. Secondly, phentolamine was made available on the injection table. We excluded those patients with PVD, ischemic heart disease, and diabetes. In a study involving 3110 patients by Lalonde et al., only those diagnosed with PVD of any variants were excluded. None of the patients had any tissue ischemia. 4 However, a stricter screening and patient selection would be beneficial.
No significant differences were found in pain score upon injection and duration of surgery. These results are comparable to recent studies. 5,20 Patients did not complain of any pain upon the second injection as it was done after the pinprick test. The surgical area had a duration of 17 s faster to achieve anesthesia compared to the control group, but this was not significant. No additional WALANT injection needed intraoperatively. Thus with WALANT, we were able to provide equal outcomes to the conventional method but without the tourniquet discomfort. Our study is limited because it is not double-blinded. As injections for the control group were given in the operation theater, the surgeons were aware of the grouping of the patient. This could lead to bias in hemostasis scoring.
Conclusion
WALANT provides excellent surgical field visibility and is safe and on par with conventional methods but without the usage of a tourniquet and its associated discomfort. Timing and technique of injection are paramount in maximizing WALANT ability. Therefore, we recommend WALANT in a selected group of patients.
Footnotes
Acknowledgment
The authors thank Mohd Kamarulariffin for his data and statistical assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Research Council of Faculty of Medicine, Hospital University Kebangsaan Malaysia (FF-2016-284).