
Abstract
Minimally invasive trans-symphyseal screw (TSS) for pubic symphysis diastasis was recently advocated, and its feasibility and reproducibility under 3D-navigation guidance are explored. Fifteen cases between 2016 and 2021 with a background of pubic symphysis diastasis are reviewed in this case series. Twenty-two TSS were inserted with an average Injury Severity Score of 35.3. Sixty percent received a one-stage procedure including fracture reduction, intra-operative 3D imaging, and planning followed by execution. The mean operative time and blood loss were 132 minutes and 160 ml, respectively. Average fracture healing was 5.8 months with two delayed unions at 9 months. The pubic symphysis distance was maintained in all cases at 6 months post-op. The average Marjeed score, Multicenter Study Group Pelvic Outcome Score, and Numeric pain rating scale were 60.2, 6.5, and 2.7, respectively. We conclude that 3D-navigation-guided percutaneous TSS restores pelvic stability and provides satisfactory pain control, and thus a safe and effective alternative to open reduction internal fixation.
Introduction
It is crucial to restore mechanical stability in traumatic pelvic fractures. Considerations must be given to the deformity, displacement, as well as anatomy while planning incision and exposure for reduction and fixation. For anterior pelvic ring fixation (including pubic ramus fracture and pubic symphysis diastasis), open reduction and internal fixation (ORIF) remain the gold standard.1,2 However, it is associated with large wound exposure, increased blood loss, and carries considerable surgical morbidities. In patients who suffer from open pelvic fractures, significant crushing, or internal degloving injuries and polytraumatized patients with multisystem injuries, ORIF becomes unfavorable. Since surgical morbidities are potentially magnified, external fixation as a definitive treatment is a common alternative. Their drawbacks include pin tract complications, infections, challenging rehabilitation, and nursing care. In these cases, minimally invasive surgery (MIS) could be a safe feasible alternative.
In the past two decades, imaging devices and orthopedic surgical techniques have greatly improved.1,3–5 Three-dimensional (3D) navigated MIS has the advantage of shorter operative time with decreased blood loss and reduced amount of radiation exposure compared to the conventional fluoroscopic guided approach.1,6,7 Previous studies have suggested early weight-bearing walking exercise for selective cases, which led to a shorter length of stay and early mobilization.6–8 For anterior pelvic ring fracture, MIS anterior column (AC) screws (antegrade/retrograde) are gaining popularity and fixation strength has shown to be comparable, whereas trans-symphyseal screws (TSS) are less commonly mentioned. It has been a developmental milestone in our center as we accumulate more experience with 3D navigation-guided MIS since 2015.3,5,9 Fixation of pubic symphysis diastasis using MIS TSS was explored and described in this study.
Patients and methods
Patients with pelvic fracture admitted from January 2016 to June 2021 were retrospectively reviewed. Those with pubic symphysis diastasis were included in our study. 3D-navigation MIS TSSs were chosen for the appropriate cases. These include patients with poor local soft tissue conditions and those with concomitant complicated fractures or visceral injuries requiring extensive dissection and open pelvic fractures. We excluded patients who are medically unfit for definitive fixation, and they were treated with external fixators or bed rest to promote fracture union. The patient demographics, Injury Severity Score (ISS), operative parameters, post-operative complications, and radiological measurements were documented by our resident.
With the accumulated experience of 3D-navigation MIS pelvis fixation and later utilization of Ziehm Vision RFD 3D Flat Panel that provides a higher resolution and larger field of view (FOV), we have extended our indications of MIS TSS to those with stable hemodynamics and a less complicated fracture pattern without excessive displacement since February 2019. A special indication for MIS TSS is when MRI-compatible plating instruments are not available for patients who require MRI assessment for other indications such as concomitant spinal injury. For every MIS surgery, we also anticipate the possibility to convert to open procedures as MISs are known to be technically demanding and tolerate a narrow margin of error. Informed consent, expertise, and instruments are always prepared.
Fracture reduction and pre-operative planning
MIS can only be performed for fractures that can be cannulated by screws and reducible, be it with simple limb traction or joystick manipulation using an external fixator. 10 The reduction maneuver should reverse the deforming force of the pelvic injury, and reduction maintained by locking the external fixator. Pelvic computed tomography (CT) was performed pre-operatively once the patient was hemodynamically stable. Bone quality as well as the feasibility to execute navigation-guided MIS were assessed then. We also planned the optimal entry and trajectory of screw insertion pre-operatively in the navigation system. For example, the superior entry should be avoided due to easy stripping and potential entry to the true pelvis; the entry point should not be too inferior either due to the risk of urethral injury; nor should the trajectory be too horizontal to avoid difficult execution. The trajectory of TSS should avoid penetrating the posterior cortex of the pubic rami risking bladder injury. Patients with a larger body build or an oval-shaped pelvis make guide pin placement more difficult since a more horizontal screw trajectory was required. In these cases, multiple trajectories were planned to strike a balance between the most stable yet executable one with minimal adjustments intra-operatively (Figure 1(a) to (c)).
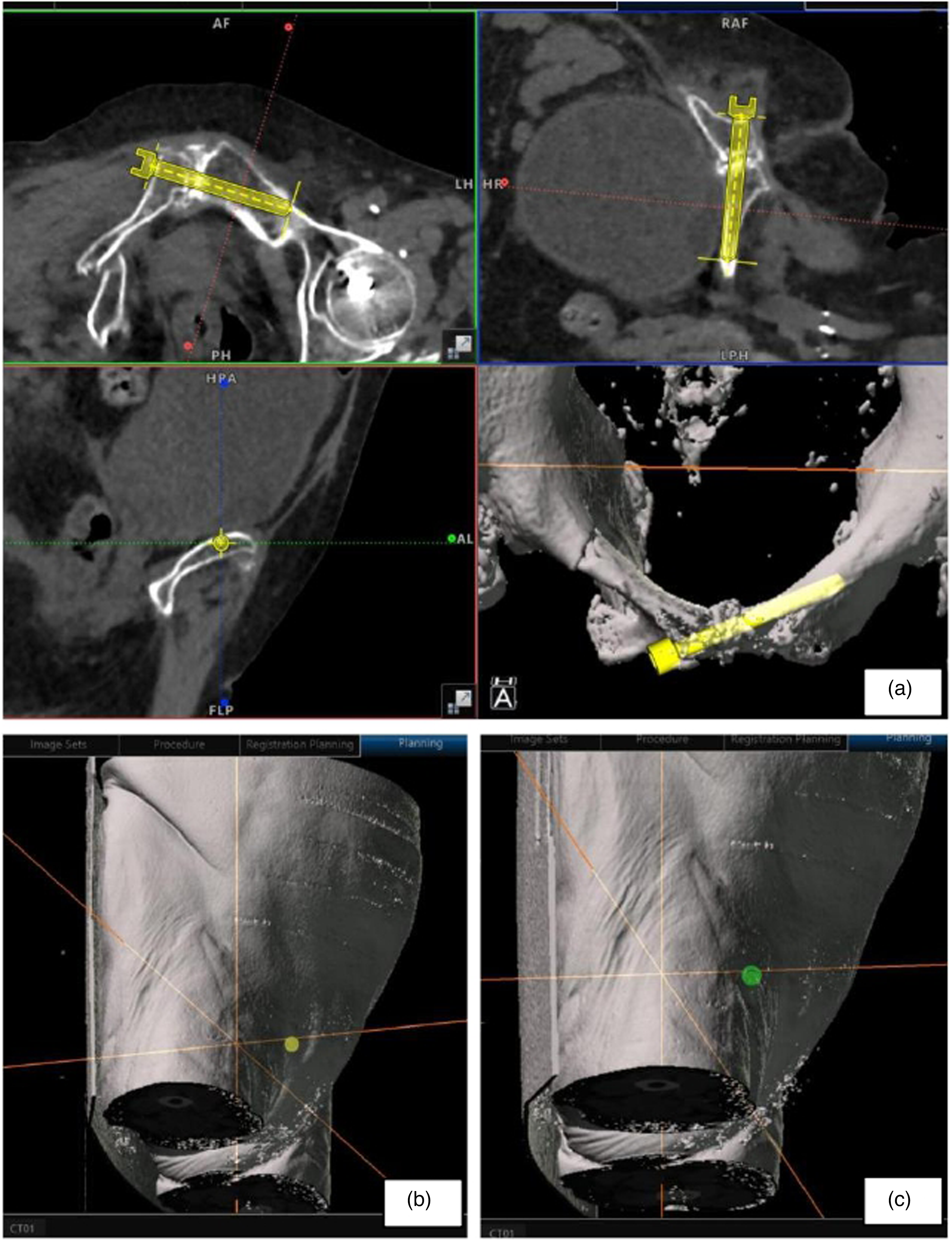
As demonstrated in the CT scan (a), patients with oval-shaped pelvis or large body size, multiple trajectories should be planned. Guide pin placement was more difficult since a more horizontal screw trajectory (b) was required. Balance should be taken to avoid the green planning (c) which would have been too horizontal causing an unideal approach through the anterior thigh.
Operative setup and execution
The patient was given general anesthesia and positioned supine on the OSI radiolucent table. This allows intra-operative 3D screening, pelvic radiological assessment, and preparation for the potential need of on-table vascular or urethral contrast studies. The Stryker NAV3i navigation system was connected to the Arcadis Orbic 3D C-arm or Ziehm Vision RFD 3D Flat Panel. The pelvis and abdomen were draped with urinary catheter inserted to decompress the bladder and to monitor urine output. This is particularly important as a urethral injury during screw insertion may present with hematuria; thus, its presence warrants an immediate pause of the operation to evaluate the potential cause. A patient tracker was installed on the external fixator or to a stable iliac crest. Intra-operative 3D scanning of the region of interest followed by fusion of intra-operative 3D images to pre-operative CT scan allows the execution of planned screws. If we were unable to merge the scans or if further reduction is needed, we would proceed with intra-operative planning and accept a smaller FOV, less optimal imaging quality, and extra anesthetic duration. Skin incision and careful blunt dissection of soft tissue along the planned screw trajectory should be guided by navigation to minimize unnecessary soft tissue trauma. Clear dissection down to the periosteum to include the whole screw trajectory path decreases the risk of soft tissue coiling by screw threads upon insertion. We also advocate draping the contralateral lower limb as one may need to manipulate it to facilitate screw insertion. If a pelvic external fixator has been applied for stabilization upon admission, it should be included in the sterile operative field as well. Not only does it maintain the reduction and hemostasis, but it could also be used to manipulate the fracture throughout the procedure to facilitate the execution of our procedure. After all guide pins were inserted, we loosen all the external fixator connections before the final tightening of screws. Two 6.5-mm cannulated screws are preferred over a single screw if anatomy and execution were possible in order to achieve improved fixation stability. Partially threaded screws were chosen for better inter-fragmentary compression while fully threaded screws have increased pullout strength. Antero-posterior, inlet, outlet, and cross-table lateral X-ray views of the pelvis were taken for verification of the finalized guide pins and screws positions. Ipsilateral obturator oblique outlet view is useful to visualize the relationship of the screw to hip joint.
Post-operative measurements
Our resident made and standardized all measurements on an inlet view X-ray films taken before, immediately after, and at least 6 months after the operation. The pubic symphysis distance is taken as the greatest transverse width at the mid-third of the symphyseal joint. The screw back-out distance is defined as the distance from the center of the screw head 6 months after the operation to that immediately after the operation.
Results
We reviewed 15 consecutive patients with pelvic fracture and pubic symphysis diastasis undergoing 3D-navigation-guided MIS for trans-symphyseal fixation (Table 1). The mean age was 57.9 (24–95) years old. Fourteen patients (93.3%) had multidisciplinary trauma activation upon arrival at the Accident and Emergency Department. The average ISS was 35.3 (9–66). Eleven patients with unstable hemodynamics (73.3%) underwent our 3-in-1 exsanguinating pelvic fracture damage control protocol for emergency pelvic hemostasis including external fixation, retroperitoneal packing, followed by angiogram +/− embolization. 4 Mean duration from injury to definitive MIS fixation was 5.7 (2–10) days. Nine cases (60%) received one-stage procedures, which included close reduction, intra-operative 3D imaging, intra-operative planning, and navigation execution of TSS. The remaining six cases (40%) required separate operative sessions for close reduction and definitive fixation, due to prioritization of management to concomitant injuries. We inserted 76 screws in total, 22 (28.9%) were TSS; 61 (80.3%) screws were partially threaded screws and the rest were fully threaded; 69 (90.8%) of the screws were successfully inserted completely under 3D navigation. The average total operative time per navigated screw was 29.1 (18.0–52.5) minutes. The mean total operative time was 132.3 (80–240) minutes, and the mean operative blood loss was 159.6 (20–480) ml.
Patient details and intra-operative parameters.
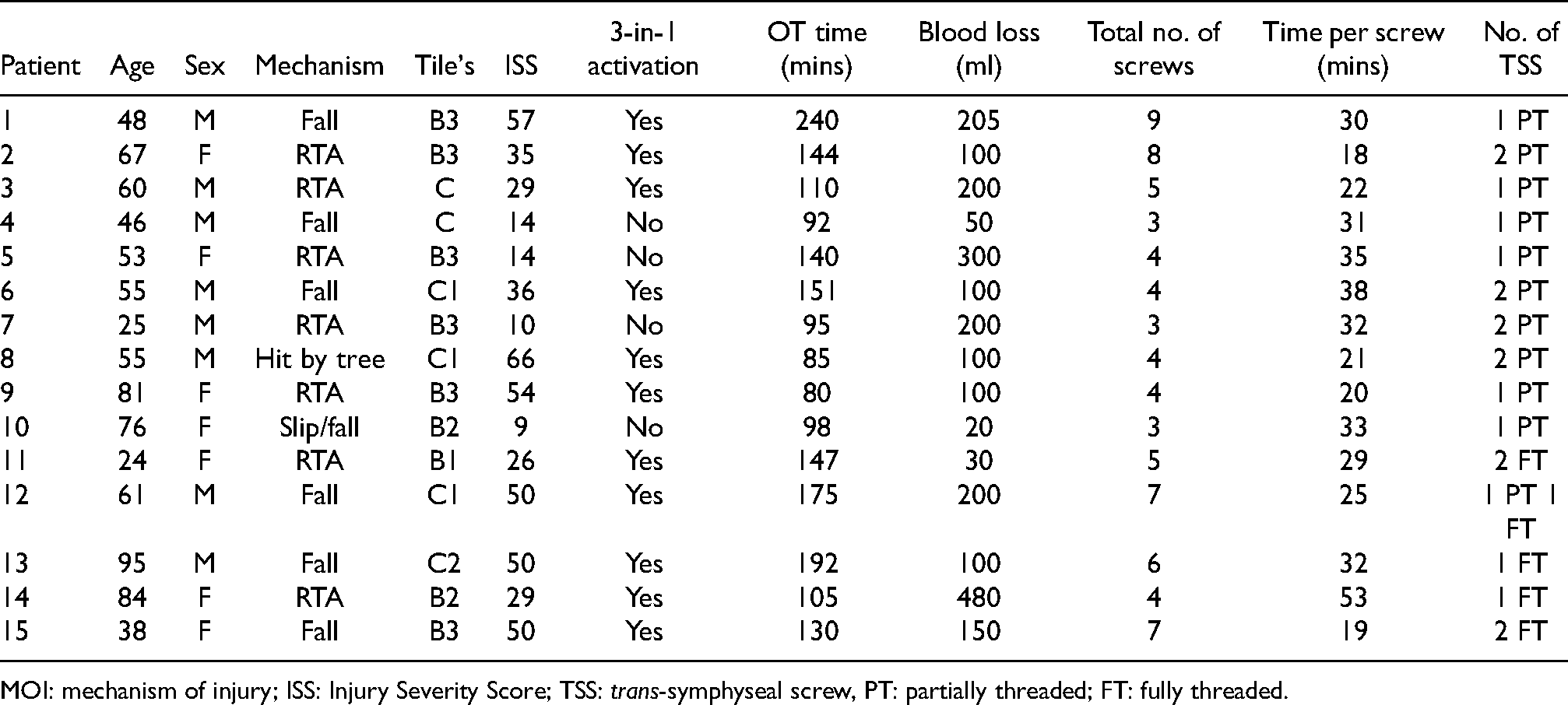
MOI: mechanism of injury; ISS: Injury Severity Score; TSS: trans-symphyseal screw, PT: partially threaded; FT: fully threaded.
There were no immediate, early, or major surgical complications apart from a case of a broken drill bit (Table 2). One patient was transferred to a private hospital and defaulted our follow-up; another patient who walked unaided upon a 3-month follow-up defaulted subsequently. The remaining 12 (80%) patients were followed up in the outpatient clinic for at least 6 months. Nine patients had a follow-up pelvic CT scan. Average fracture healing was 5.8 (3–9) months. There was no cortical perforation of screws. Four out of 22 (18.2%) TSS backed out (in three patients) for an average of 14.5 (8–26) mm; all of them are partially threaded. One of these patients required the removal of screws due to impingement symptoms after attaining fracture healing. The average pubic symphysis distance was reduced from 7.4 (4.6–18.7) mm to 4.0 (2.3–5.9) mm immediately post-operation. X-ray 6 months later remained static with an average distance of 3.6 (1.9–6.0) mm thus reflecting a stable fixation with no further widening of pubic symphysis. Upon follow-up, three patients (23.1%) walked unaided, three (23.1%) required a stick, four (31%) walked with a frame, three patients (23.1%) were bedbound with one patient being non-ambulatory before injury; one patient sustained a concomitant severe head injury and spinal fracture rendering him paraplegic; another one patient sustained concomitant massive stroke evident on initial trauma CT. The average Marjeed score was 60.2 (27–100), the average Multicenter Study Group Pelvic Outcome Score was 6.5 (5–9), and the average post-operatively numerical pain rating scale was 2.7 (0–6).
Patient details and post-operative parameters.
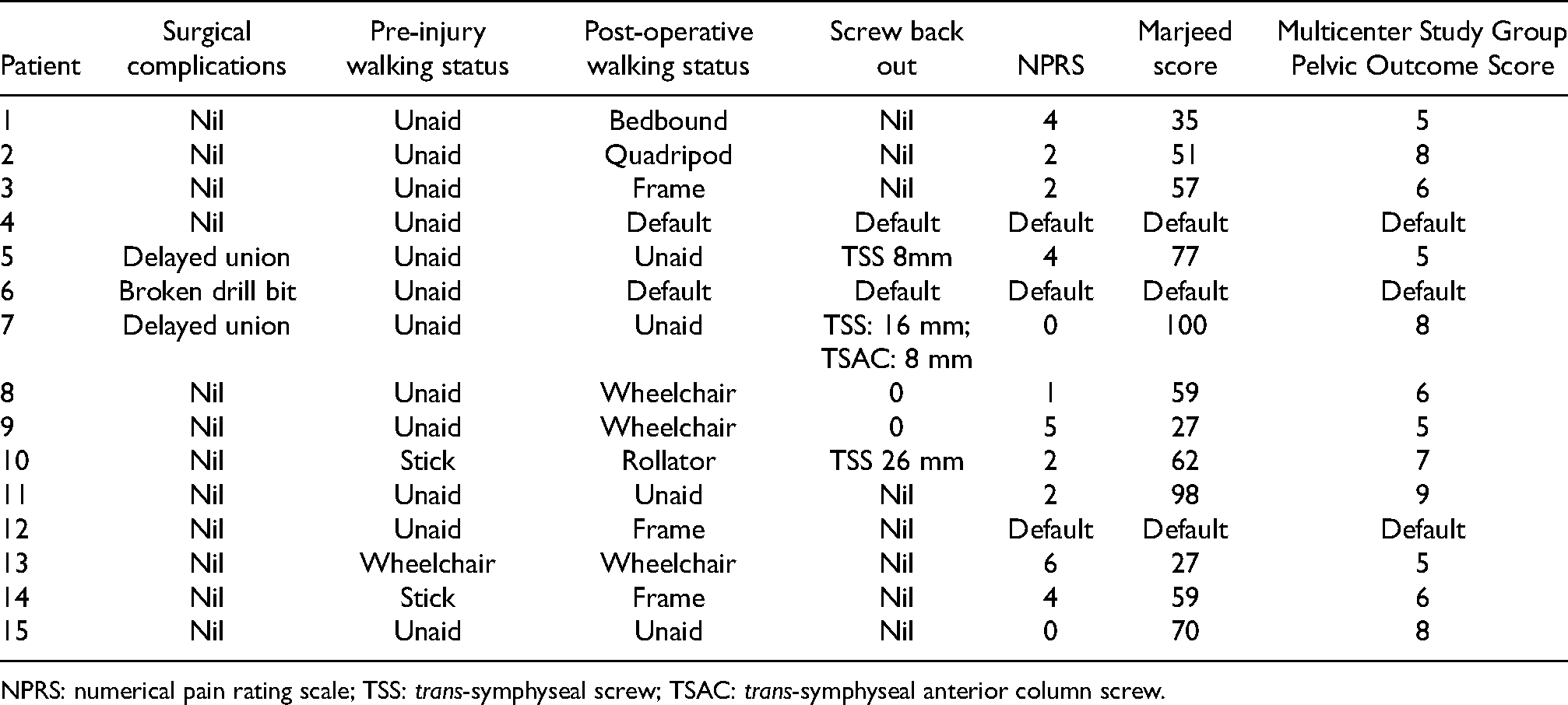
NPRS: numerical pain rating scale; TSS: trans-symphyseal screw; TSAC: trans-symphyseal anterior column screw.
The following cases are selected to illustrate our developmental milestones of the TSS technique:
Case 1 (Figure 2(a) to (c)): A 67 years old lady suffered from Tile B3 pelvic fracture with left posterior hip dislocation and a mangled left lower limb injury after a road traffic accident. Delayed primary left above-knee amputation was performed. CT showed an oval-shaped pelvis with bilateral sacroiliac joint and pubic symphysis diastasis plus a left acetabulum and posterior wall fracture. Kocher-Langenbeck's approach was adopted for the acetabular fixation. MIS TSS and bilateral retrograde AC screw were used to substitute a long plate fixation in the traditional anterior approach ORIF, which would have required a very extensive dissection to the far lateral edges of the pelvic brim.
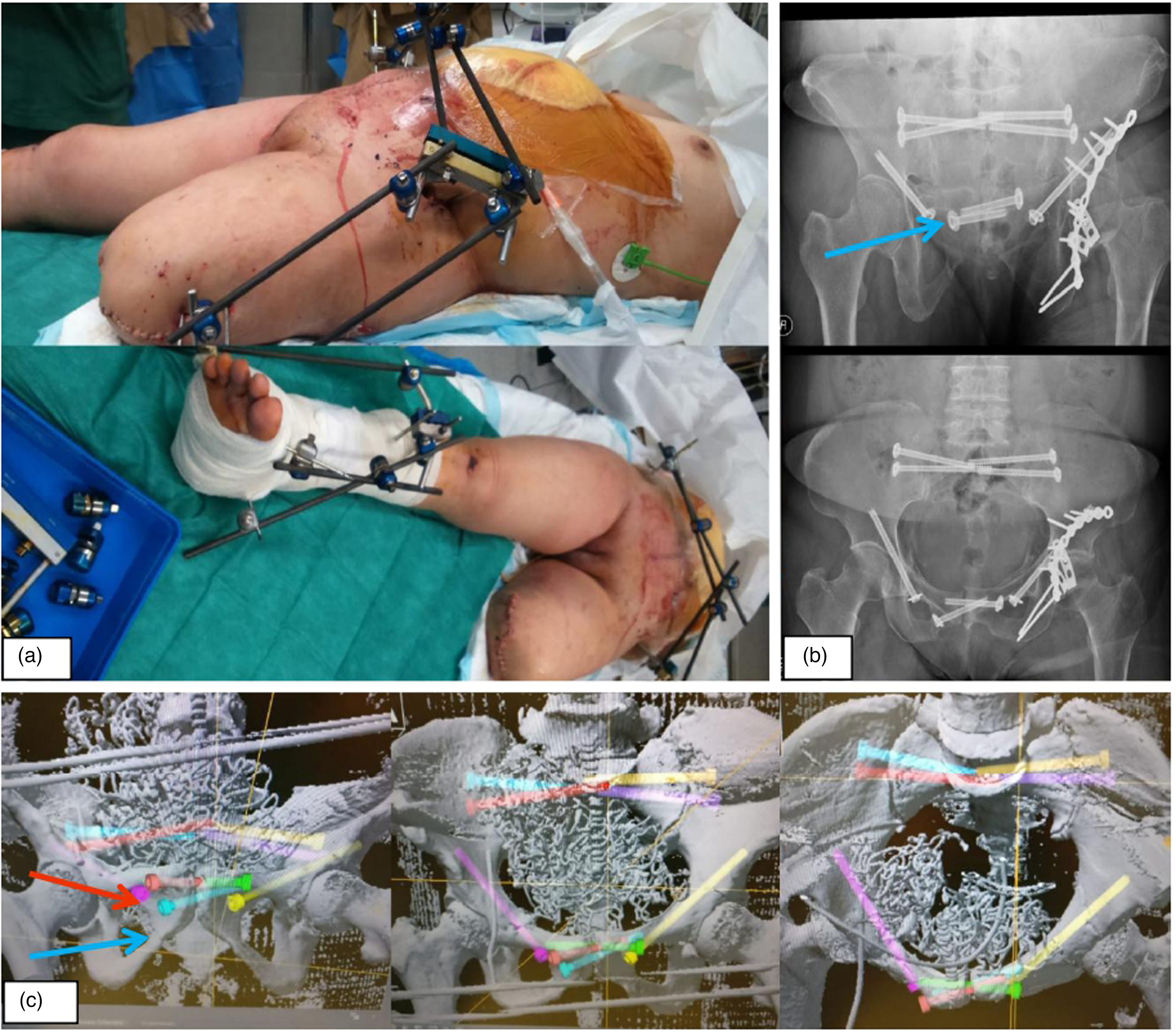
Multiple trajectories of TSS were planned pre-operatively as we foresaw difficulty in the execution of MIS due to the horizontal anatomy of the pubic rami in this oval-shaped pelvis. To tackle both the complex pelvic and acetabulum fractures in this case, a combined MIS and ORIF approach (a, b) was used to avoid two open approaches with extensive surgical dissection and lengthy surgery in this polytraumatized patient in order to reduce surgical morbidity and promote early recovery. The most executable planning was chosen intra-operatively (c), the right side TSS in blue was chosen over the red screw.
Case 2 (Figure 3(a) to (c)): A 51 years old gentleman was admitted for Tile C pelvic fracture after a road traffic accident. One-stage close reduction followed by navigation TSS with bilateral sacroiliac (SI) screws fixation was planned pre-operatively. However, navigation of TSS was abandoned in view of the anticipated unusually high stress on TSS. ORIF double plating of the pubic symphysis and bilateral SI screw fixation was performed instead. This case is not included in our series but we would like to illustrate the importance of open plating as a backup plan for percutaneous TSS. TSS may not be stable enough for a pelvic ring with gross mechanical instability.
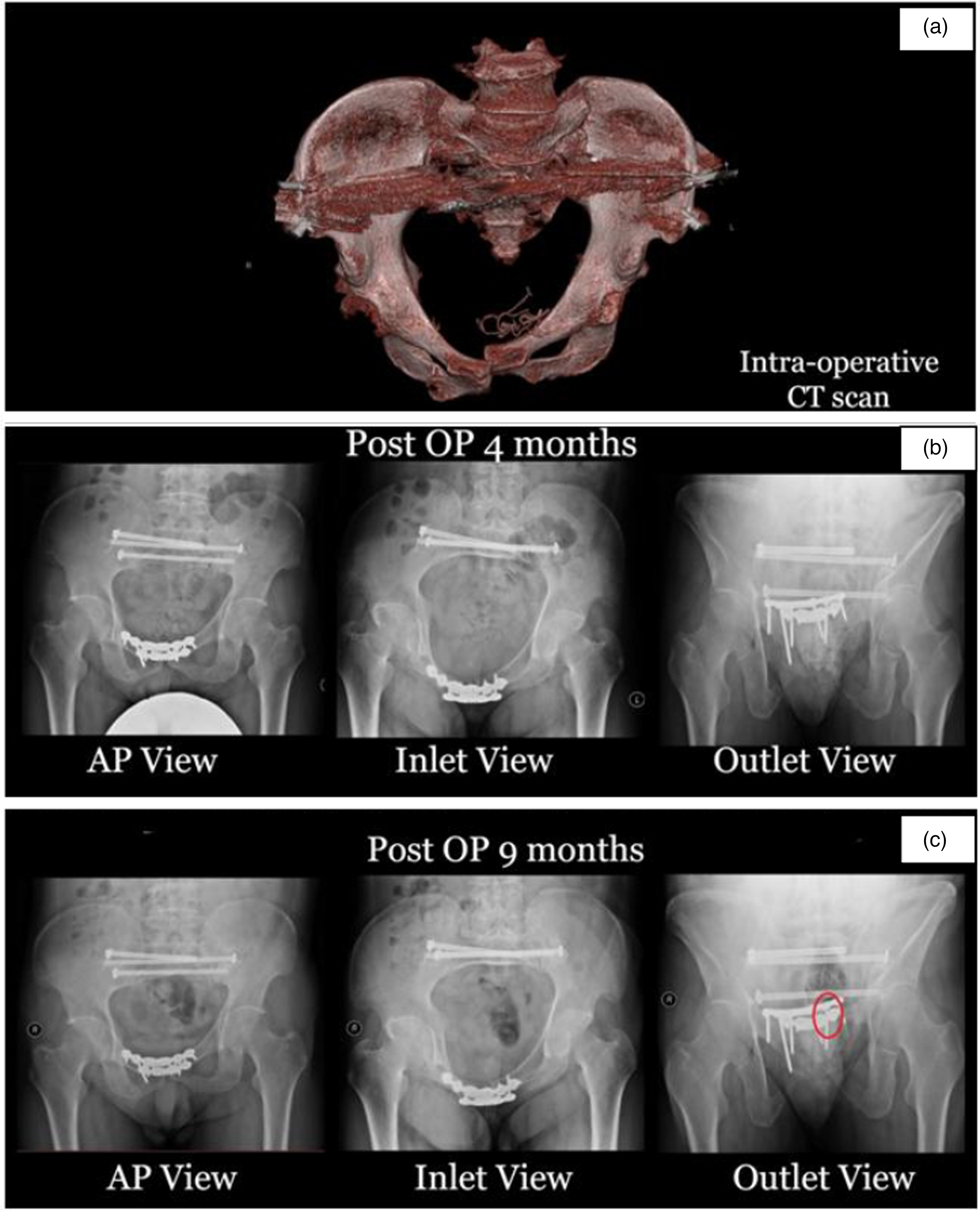
One-stage close reduction followed by navigation TSS with bilateral SI screws fixation was planned pre-operatively. However, intra-operative CT scan (a) confirmed severe pubic symphysis diastasis even after external fixation was used for close reduction. Therefore, navigation of TSS was abandoned in view of the anticipated unusually high stress on TSS. ORIF double plating of pubic symphysis was performed via modified Stoppa approach, followed by navigation-guided bilateral SI screws. The instability of pelvis is reflected by the fact even with anterior double plating (b), there was significant stress over the pelvis causing screw breakage at the superior pubic symphysis plate 9 months after the operation (c).
Case 3 (Figure 4(a) to (f)): A 25 years old gentleman suffered from Tile B3 pelvic fracture with pubic symphysis diastasis, left AC, and right pubic ramus fracture. One right partially threaded TSS, one right partially threaded trans-symphyseal anterior column screw (TSAC), and one left partially threaded antegrade AC screw were used to fix the fracture. We started right touch down walking and left full weight-bearing walking exercise for him post-operatively for 4 weeks followed by 4 weeks of right partial weight before full weight bearing. During the follow-up X-ray, we noticed backing out of the TSS by 16 mm and the TSAC by 8 mm at 5 months post-operation requiring screw removal. From this case, we learned that one should consider the use of fully threaded screws to improve purchase,11–13 especially in young active patients with early rehabilitation. Another point would be to consider fixation of the posterior pelvic ring with a left SI screw for more stabilization of the iliac wing as there was a suspected crack over the left sacrum retrospectively.
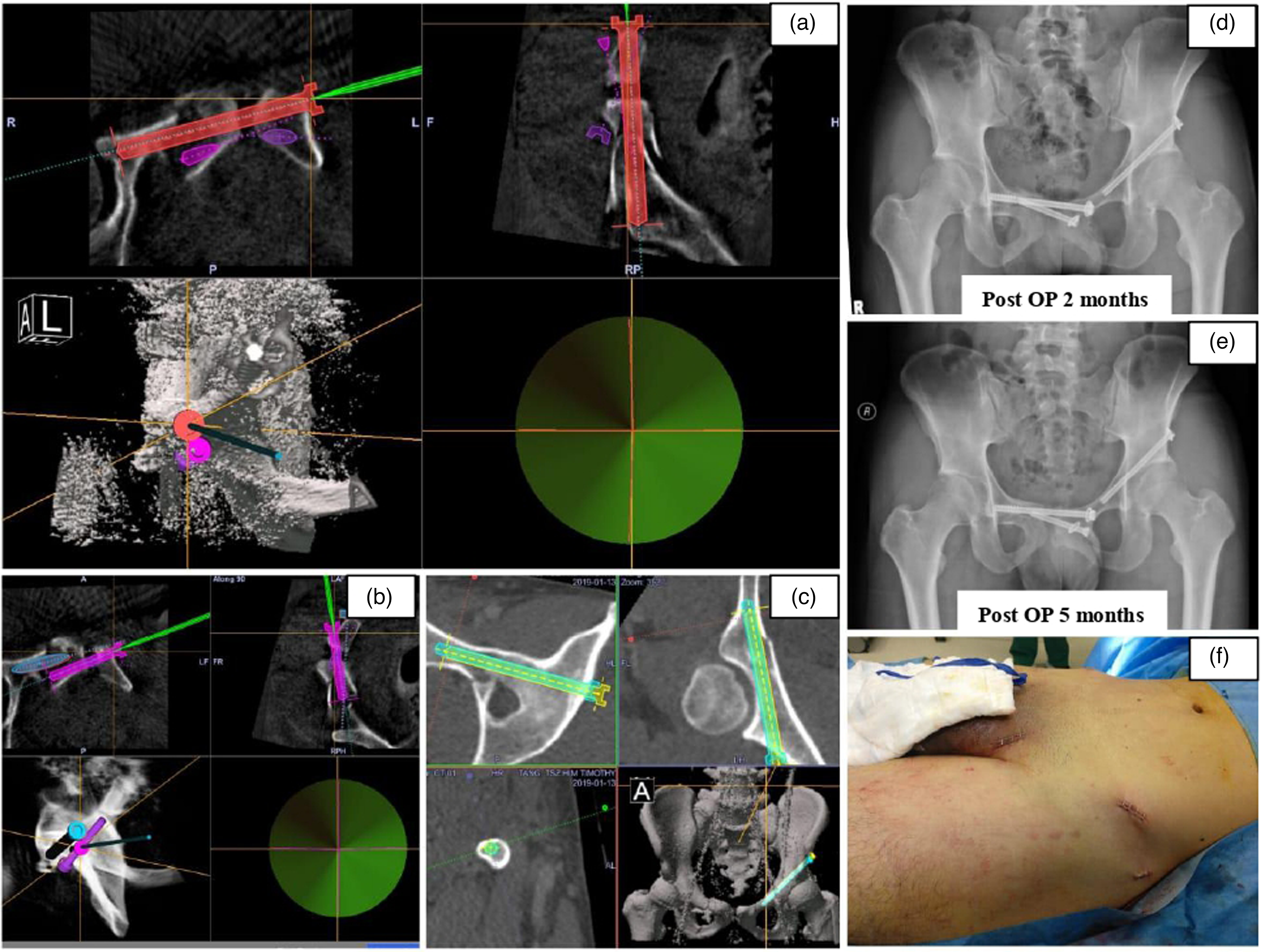
One right TSAC (a) and one right TSS (b) were inserted with a guide pin centered along planned trajectory as demonstrated by the overlapping of crosses and green indicator. Another left anterior column screw was inserted (c). During the follow-up X-ray, we noticed backing out of the TSS by 16 mm and the TSAC by 8 mm at 5 months post-operation (d, e). They caused impingement symptoms requiring screws removal. Latest follow-up at 2 years post fixation, the pelvic alignment was maintained and he is walking unaided with satisfactory activities of daily living. Only small stab wounds were required for these MIS insertions (f).
Case 4 (Figure 5(a) and (b)): A 24 years old lady was hit by a taxi and was admitted for Tile B1 pelvic fracture with right sacrum, right superior and inferior pubic rami, and pubic symphysis diaphysis. External fixation of the pelvis was performed upon admission. During the definitive operation, the fixator was loosened and used as a joystick to manipulate the right ilium. Additional direct manual pressure on the right medial pubic ramus was required in order to achieve satisfactory reduction. Two fully threaded SI screws, one partially threaded AC screw, and two fully threaded TSS were inserted. The use of fully threaded screws along with dual TSS provided stronger fixation strength for this young active patient. Follow-up CT 6 months shows satisfactory alignment.
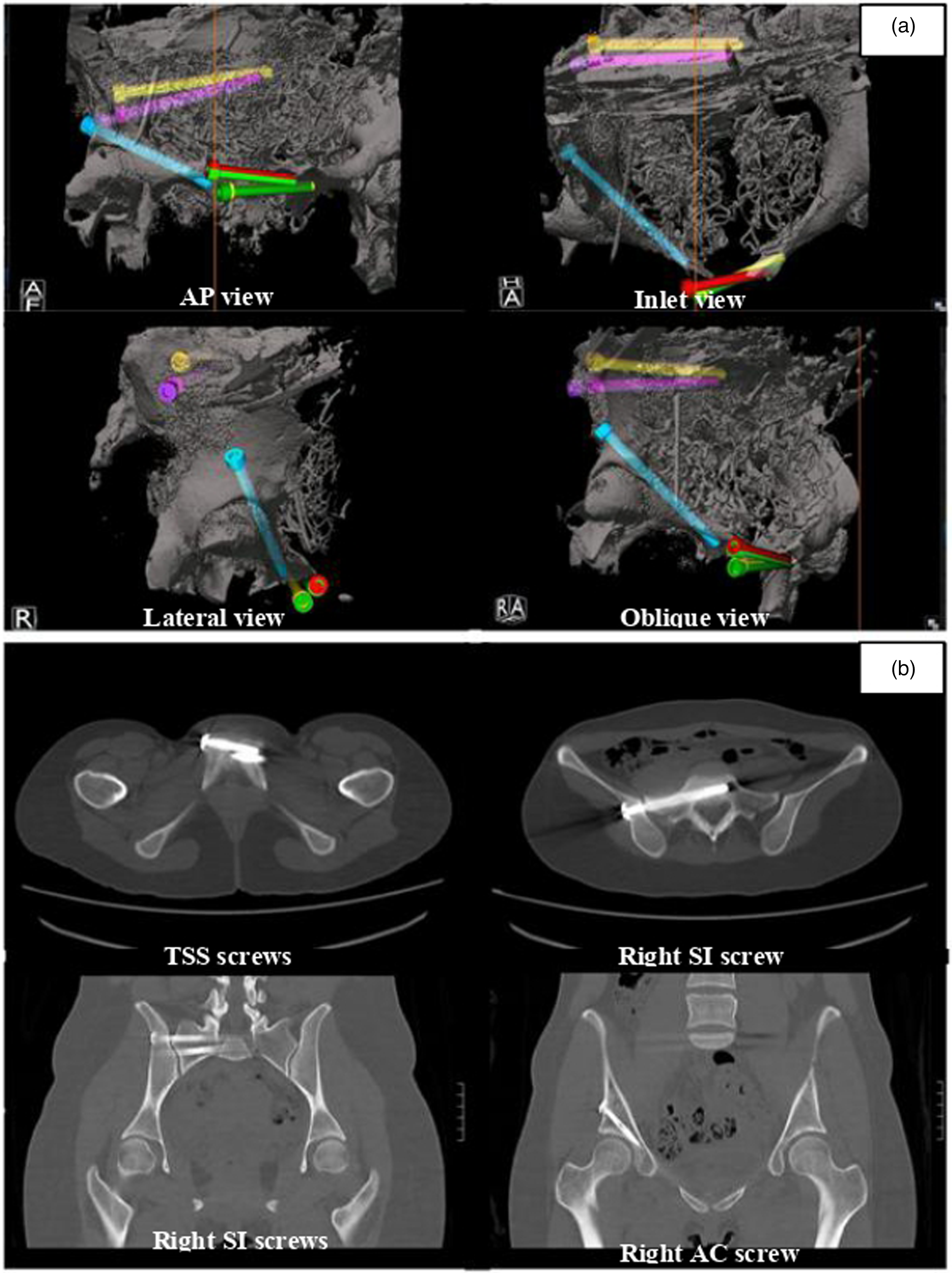
External fixation was performed on admission for Tile B1 pelvic fracture with right sacrum, right superior and inferior pubic rami, and pubic symphysis diaphysis. The use of flat panel 3D machine allows for a large FOV of a single intra-operative 3D (a) to include the whole pelvis. This facilitated a one-stage operation that included reduction, planning, and execution thus simplifying logistics and shortened operative duration. Two fully threaded SI screws, one partially threaded AC screw, and two fully threaded TSS were inserted. The CT scan 6 months after the operation showed satisfactory pelvic alignment without screws backing out or loosening (b).
Discussion
In a meta-analysis, 14 3D navigation had lower cortical perforation rates and better adherence to planned screw trajectories compared to 2D fluoroscopy-based navigation in model and cadaveric acetabular fractures. Based on our experience, 3D-guided navigation MISs reduces blood loss, radiation exposure to operative staff, and improved screw placement accuracy within reasonable operative time in most pelvi-acetabular fractures—including those with pubic symphysis diastasis.
The anterior pelvic ring had a 40% effect of stabilizing the pelvis while the posterior ring constitutes the remaining 60%. 6 Biomechanical study 15 has shown that incomplete pelvic mechanics can lead to instability of the pelvis and the stability of the anterior ring greatly affects the load and displacement of the posterior ring. Therefore, it is of utmost importance that we aim to restore the mechanical stability of both anterior and posterior pelvic rings in order to achieve the best clinical outcomes. Multiple fixation options exist for pubic symphysis diastasis, including pelvic external fixator alone, plate and screws, with or without additional tension band wiring/strong suture materials, or combination of both.16–18 However, open reduction is associated with a longer operative time and higher infection risk while external fixators are functionally inconvenient for the patient. 19 A new percutaneous technique using cannulated screws under radiological navigation has been proposed and has shown comparable biomechanical properties to reconstruction plate screw fixation in selected pelvic fracture patterns.11,13,16,19 Furthermore, percutaneous screws have the advantages of being minimally invasive, less blood loss, shorter operative time, and a smaller scar. 13
Mu et al. 11 reported eight patients with MIS fixation under 2D navigation, and Yu et al. 13 reported another 24 patients with Tile B1 fracture reduction performed under X-ray guidance. All these cases had pubic symphysis diastasis and were treated with percutaneous screw fixation. A biomechanical study conducted by Yu et al. showed that the maximum stress on a cannulated screw was much less than on a plate (30.9 vs 1846 MPa). Yu also demonstrated comparable results in repairing and avoiding further pubic symphysis separation with a cannulated screw when compared to the reconstruction plate with a maximum displacement of 0.41 mm for plating and 0.64 mm for screws. Cano Luis et al. 20 compared the biomechanical properties of cannulated screws and intact pubic symphysis that supported the idea of cannulated screws having the ability to resist rotational forces. However, more studies on the configuration of TSS and its fixation strength for various types of pelvic instability will be required before any definitive conclusion can be made. Other factors that affect the fixation strength and outcome include the screw diameter, whether it is partially or fully threaded and whether three or four cortices are required for stable fixation. From the literature, the diameters of the most commonly used cannulated screws were 6.5 and 7.3 mm.
The most challenging aspect of TSS is the requirement of a horizontal trajectory in a retrograde fashion, which is easier to execute in a skinnier patient and those with a triangular-shaped pelvis (more common in male) as compared to an obese patient with a bulky trunk that potentially blocks the screw trajectory. We have an early case in our series that had a broken drill bit due to difficult execution. In order to avoid this, we proposed a careful assessment of feasibility in pre-operative planning in order to design a less horizontal trajectory. We also suggest draping of the contralateral lower limb, which will allow us to put it in a figure-of-4 position. Together with the manual pressure of the contralateral proximal thigh, this will minimize the amount of soft tissue blocking the execution trajectory and increase the amount of working space for the surgeon. As previously advocated, multiple entries and trajectories should be planned across the same fracture site and a balance should be taken between the most executable yet stable screws with the best possible purchase when difficult cases are anticipated. We also experimented with the use of the “drop screw” function in the Stryker navigation system. It allows the real-time creation of a virtual screw in the planning system that simulates the most preferable yet executable screw position while the instrument tracker is being placed. Last but not least, we believe the pre-operative preparation for alternative pubic symphysis diastasis fixation methods including open plating is always a safe practice.
Concerning post-operative screw displacements, we noticed that fully threaded screws showed less screw back out compared to partially threaded screws. Four out of 61 partially threaded screws in three patients backed out for an average of 14.5 mm, in which three of them were TSS (back-out distance 8, 16, and 26 mm, respectively) and one was a trans-symphyseal AC screw (8 mm back out). Fully threaded screws are most beneficial in the osteoporotic bone as they have better bone purchase with the additional benefit of solid tactile feedback upon insertion during the operation. The drawback remains the lack of inter-fragmentary compression and difficulty in removal. In the case of concomitant posterior pelvic ring injury (more commonly seen in patients with wider pubic symphysis diastasis), additional SI screws should be added to further stabilize the pelvic ring and to neutralize the stress of anterior fixation, as demonstrated in Case 3. In patients with poor bone quality (especially elderly ladies with osteoporosis) or those considered to have serious mechanical instability but contraindicated for anterior ORIF, successful screw purchase may be an issue hence temporary external fixation can be added or kept on a pro re nata basis. Cement augmentation or specially coated screws may reduce screw loosening but more studies are required to ascertain their use in anterior pelvic ring injury.
In our case series, TSS was not only used to fix pelvic fractures with pubic symphysis diastasis, but its use was also extended in fixing medial pubic rami fractures with very small medial fragments with the aid of the contralateral medial pubic bone to provide better purchase for proximal fixation of TSS compared to retrograde AC screw. In cases where pubic rami fractures with low to mid-anterior column fractures are identified, TSAC can be used to fix both the pubic symphysis and the superior pubic ramus, with another TSS as a positional screw. SI screws should also be added if posterior pelvic fractures are suspected and unstable. In cases where a single fixation approach may not be the best strategy to tackle the fracture, a combined MIS and open reduction could be the ideal approach as illustrated in Case 1. Less surgical dissection was required for two TSS and antegrade AC screws via the MIS approach as compared to the traditional open method. We believe it was a reasonable, if not ideal, fixation strategy for this lady with concomitant transverse and posterior wall fracture along with a dislocated hip and mangled left leg in the hope to reduce the blood loss and enhance recovery while providing the best reduction and fixation.
Based on our experience with 3D-navigation MIS fixation of all pelvi-acetabular fractures since 2015, we observed satisfactory fracture healing with minimal screws displacement even in cases of very early or immediate post-operative full weight-bearing walking exercise, with no implant failure. 7 In this case series, our post-operative physiotherapy regimen has also progressed from being conservative to becoming more aggressive. In the early phase of our series, we offered a non-weight-bearing walking exercise to our first case with an external fixator as an adjunct. In later cases, immediate partial or full weight-bearing walking exercise was adopted, depending on the fracture pattern, intra-operative screw purchase, and bone quality. The transition toward a more aggressive rehabilitation is supported by previous biomechanical studies that have shown that cannulated screws are able to resist rotational forces well with a lower stress loaded across the screw due to its intramedullary fixation.13,20,21 It has also been shown that anterior pelvic fractures fixed with cannulated screws exhibit similar physiological behavior to an uninjured pelvis under stress. They also concluded that fixation of the posterior ring fracture, if present, would provide additional stability compared to anterior fixation alone. Follow-up imaging did not show any screw breakage and the average screw back out was minimal. All follow-up X-rays showed normal age-related pubic symphysis distance with an average distance of 3.6 mm.
Conclusion
3D navigation-guided percutaneous TSSs restore pelvic stability, provide satisfactory pain control, and allow effective fracture and symphyseal healing. It is a safe and effective fixation alternative to ORIF in cases with pubic symphysis diastasis or in pelvic fracture involving very medial pubic ramus. The benefit of this MIS technique is most appreciated in cases with concomitant local soft tissue injuries or associated complex pelvi-acetabular fracture, which usually requires extensive soft tissue dissection for fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our study has been approved by our cluster's ethics committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.