
Abstract
A three-in-one protocol comprised of pelvic external fixation, retroperitoneal pelvic packing, and angiography with or without embolization has been developed and used in our centre to improve survival outcomes of hemodynamically unstable pelvic fractures since 2008. Fourteen paediatric patients over a period of 15 years are reviewed in this case series. The mean age is 11.6 and standard deviation is 4.6. The mean injury severity score is 31.6. Sixty four percent underwent three-in-one protocol management. The overall survival rate at index hospital admission and at one year is 85.7% which is higher than the adult group (81%) from a study conducted at our centre and comparable to the rate in paediatric group. One patient had pelvic external fixator pin tract infection and two had lower limb ischemia post embolization. At 6 months follow up, one patient had pelvic pain and one had hip protrusio. We conclude that improvement in survival outcome also applies to the paediatric population. Technical differences in the paediatric group is highlighted to minimize potential complications.
Keywords
Introduction
Paediatric pelvic ring fracture is a relatively rare injury in paediatric fractures with reported incidence of 0.04–4.6%. 1 However, due to the high energy frequently involved, they are associated with concomitant multiple injuries and high morbidity.
Timely intervention of these fractures is the key in management which requires seamless collaboration between multiple disciplines. Since the year 2008, our centre has implemented a three-in-one pelvic damage control protocol for hemodynamically unstable pelvic fracture patients. Promising results have been reported in our centre.2,3 This protocol has also been adopted for management in the paediatric group.
Patients and methods
We retrospectively reviewed the records of consecutive patients younger than 18 years old with pelvic fracture who were admitted via trauma activation from 2008 to 2022. The primary outcome is survival rate at index hospital admission and at one year. The secondary outcome is complications related to three-in-one management, the type of definitive treatment for pelvic fracture, functional outcome at 6 months follow up, and pelvic fracture-related complications at 6 months follow up. The patient demographic, mechanism of injury, injury severity score, fracture pattern, associated injuries, method of definitive pelvic fracture management, intensive care unit (ICU) and acute ward length stay, and the usage of fluid resuscitation, massive transfusion protocol (MTP) and transamine are also analysed.
This study had obtained approval from the hospital Institutional Review Board. These fracture patterns are grouped according to Tile classification and Torode and Zieg classification, which classify based on mechanism of injury, fracture pattern and fracture stability. 4
Upon arrival at the Accident and Emergency Department, these patients would be evaluated for mechanism of injury and vital signs for decision on trauma activation.
At our centre, absolute indications for activation of trauma call are physiological derangement or major injuries. Physiological derangements are defined as Glasgow coma scale less than or equal to 13, age adjusted systolic hypotension, or age adjusted decrease or increase in respiratory rate. Major injuries include major pelvic fracture, two or more long bones fracture, extensive facial injury or flail chest. Relative indications include patient age less than 5, road traffic accident and fall from height more than 3 m or 2 to 3 times the height of the child. A flowchart of the three-in-one pelvic damage control protocol is shown below. (Figure 1) The classification of pelvic fracture is not relevant in this protocol.
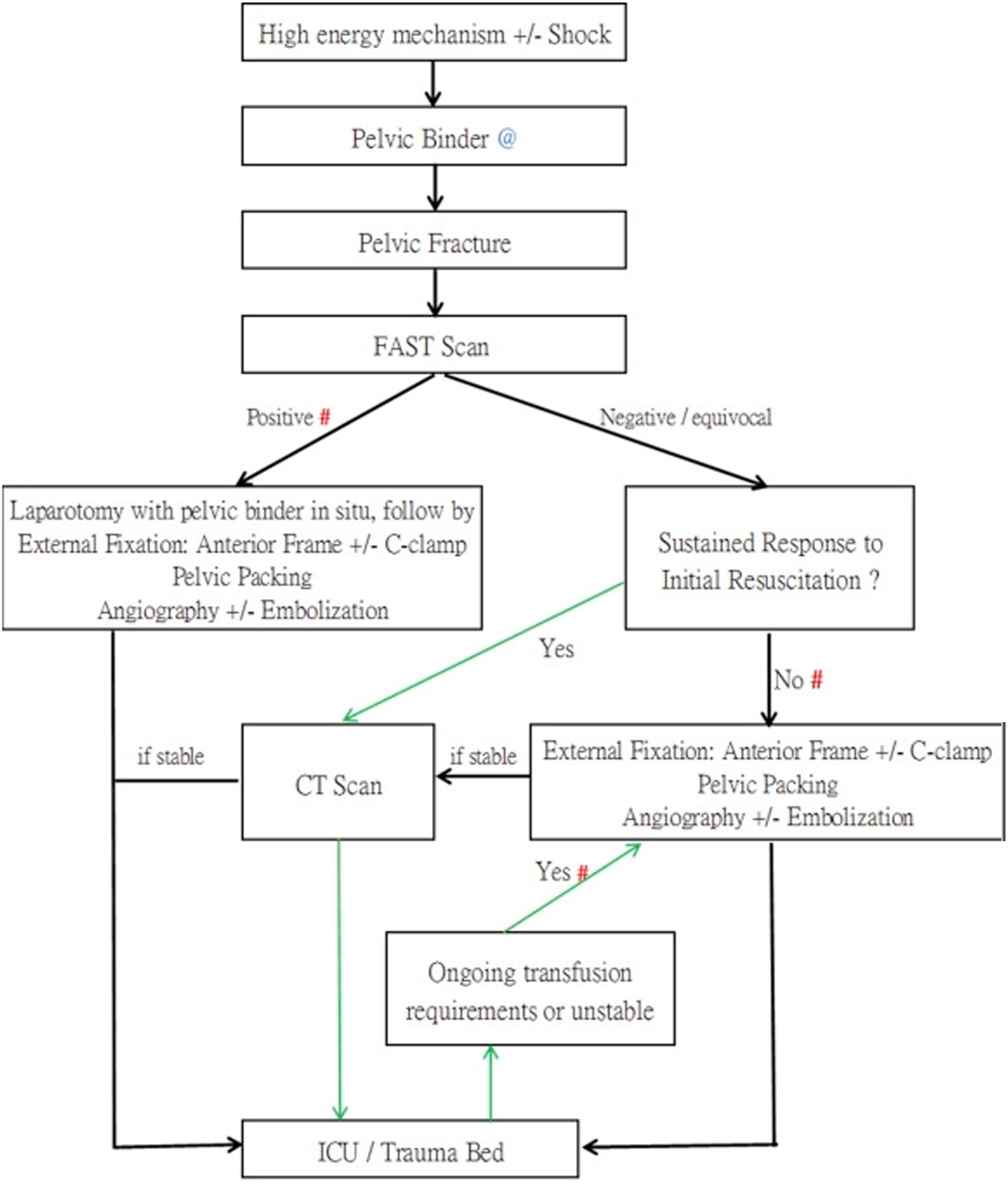
Management algorithm of the 3-in-1 pelvic damage control protocol, revised in September, 2016.
Upon arrival at the resuscitation room and activation of trauma call, these patients will undergo primary survey. Active resuscitation, intravenous fluid challenge, blood products, massive transfusion protocol (MTP) and the use of transamine together with pelvic binder and neck collar application will commence immediately as needed. Pelvic binder without the need for prior x-ray is the first step in stabilization of the pelvis in our management protocol.
Secondary survey is done at appropriate timing to assess major associated injuries. On-site X-ray of the chest and pelvis or babygram in the infant group will be arranged at the same time.
After confirming pelvic fracture, subsequent management depends on the hemodynamic stability after resuscitation. Fluid resuscitation in the form of 20 mL/kg crystalloid bolus is used. For those below the age of one, the systolic blood pressure lower limit is 70 mm of mercury (mmHg), with the lower and upper limit for heart rate being 80 and 180 beats per minute (bpm), respectively. For those above the age of one, the systolic blood pressure lower limit is 70 + (age (years) × 2) mmHg and the heart rate lower and upper limit is 60 and 160 bpm, respectively. Responders are those with stable vitals after fluid bolus. Partial responders are those with stable vitals initially after fluid bolus but unable to maintain that stability. Non-responders are those with persistent vitals instability after fluid bolus. Other signs of haemorrhagic shock like capillary refill, respiratory rate, urine output and mental status will also be under close observation.
Responders will undergo whole-body computed tomography (CT) with contrast study and be put under close observation in ICU for definitive management. Partial and non-responders will proceed to 3-in-1 pelvic haemostasis procedures. For Focused Assessment with Sonography for Trauma (FAST) positive patients, laparotomy with pelvic binder in situ will be done first. Three-in-one procedures, executed in one sequence, at the same operating suite, and preferable within the first golden hour will commence.
Technique for external fixation
External fixation is done first in order to reduce and stabilize the disrupted bony pelvis so that the pelvic volume can be limited for subsequent pelvic packing. Hoffmann II external fixator system is used in our centre. Two 5 mm or 4 mm Apex pins are inserted into each iliac crest 2 cm posterior to the anterior superior iliac spine. (ASIS) For fractures involving the iliac crest or iliac wing that might jeopardize the stability of the pins, a supra-acetabular pin is inserted on each side from anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS) with x-ray guidance. Closed reduction of pelvic fracture reversing the mechanism of injury by joysticking both iliac crest clamp, manual medial compression of greater trochanter with or without limb traction is performed if necessary, before tightening the external fixator. For posterior instability not controlled by anterior clamp with refractory hemodynamic instability, C-clamp will be utilized, generally at age 12 or above with an appropriate sized pelvis (Figures 2 to 5).
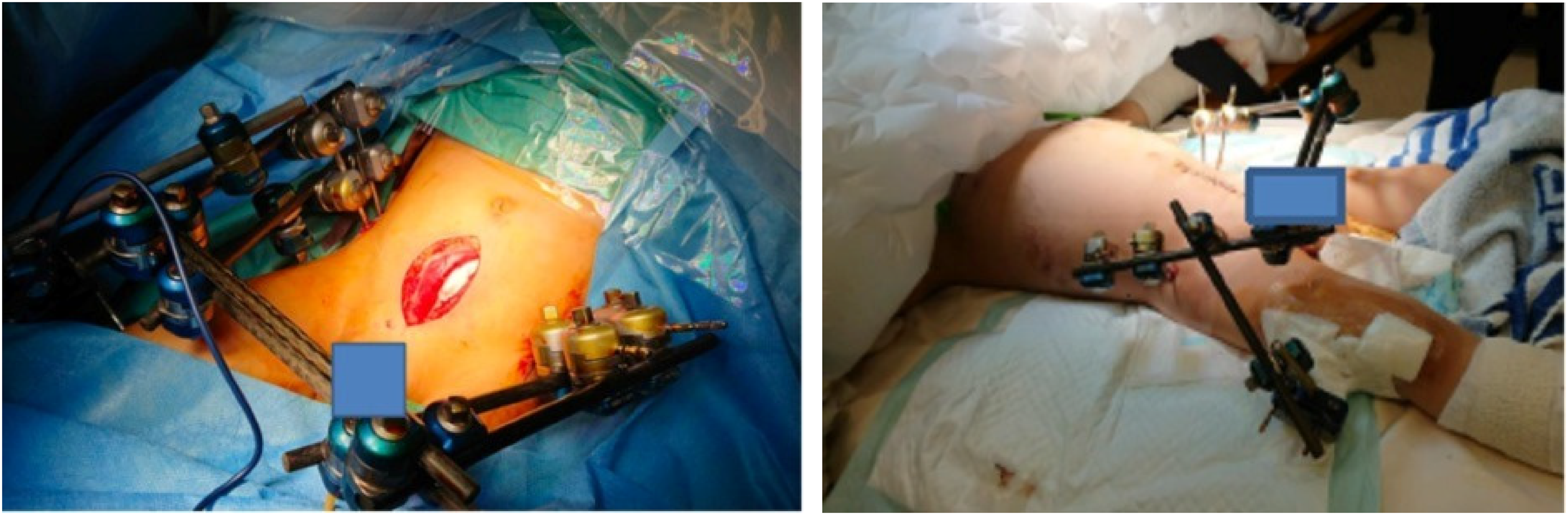
low midline incision (modified Stoppa approach) for retroperitoneal packing, which is separated from intra-peritoneal cavity. Care taken for external fixator configuration to allow access to abdominal and groin, away from abdomen to allow anticipated abdominal distension, and to allow unobstructed subsequent radiological assessment of abdominal and pelvic region. Note external fixator connected to femur for concomitant proximal femur fracture in figure 3.
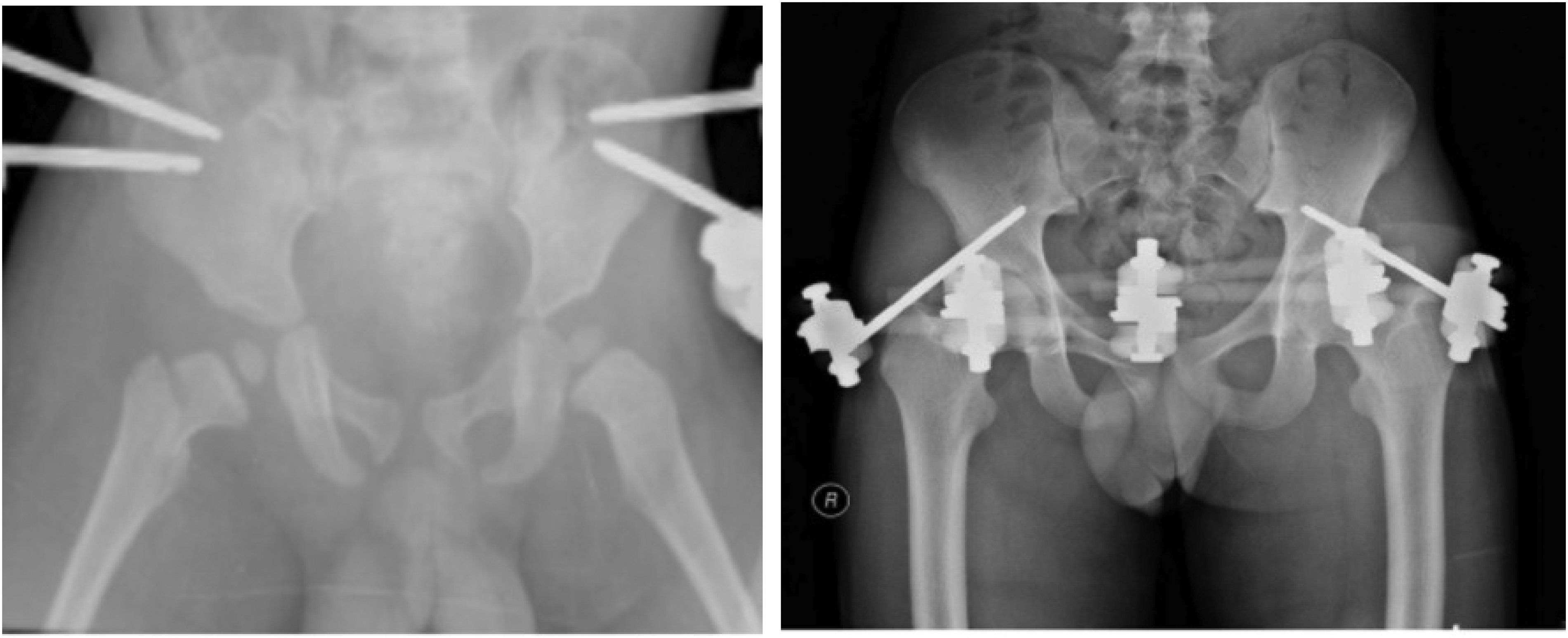
X-ray pelvis with iliac crest pins (Left) and anterior inferor iliac pins (Right).
Technique for retroperitoneal packing
Retroperitoneal packing mainly tackles venous and fracture bleeding. It is done after pelvic external fixation, and before arterial angio-embolization since majority of pelvic bleeding is from venous plexus injury and fracture sites. Access to the bleeding retroperitoneal space is achieved and packing of the pre-sacral and para-vesical region is done. It is important to ensure packing of the true pelvis without breaching the peritoneal fascia, instead of intra-abdominal packing which has virtually no tamponade effect on retroperitoneal bleeding. Re-exploration will be done after 24–48 h of achievement of hemodynamic stability for the packing gauzes to be removed, or be exchanged if persistent retroperitoneal bleeding is still present.5,6
Technique for angiography and embolization
An arterial introducer is positioned via the femoral artery at the groin. An angiogram is performed by non-selective injection of contrast medium just above the aortic bifurcation then selective injection of the branches of the internal iliac arteries. Signs of active bleed and macrovascular lesions such as false aneurysms, missing arteries and wall irregularities of arteries are detected. Vascular occlusion is achieved using gelfoam coils or glues depending on the size and site of the breach. In cases of major hemodynamic instability that persists while angiography fails to identify any arterial lesion, non-selective bilateral embolization of the internal iliac arteries with gelfoam would be performed, to reduce risk of rebleeding from any potential arterial injuries that was temporarily stopped by retroperitoneal packing or profound hypotension. At the end of the procedure, angiography is repeated to confirm that the embolized areas are occluded and to ensure there are no other regional bleeding sources (Figures 6 and 7). 7
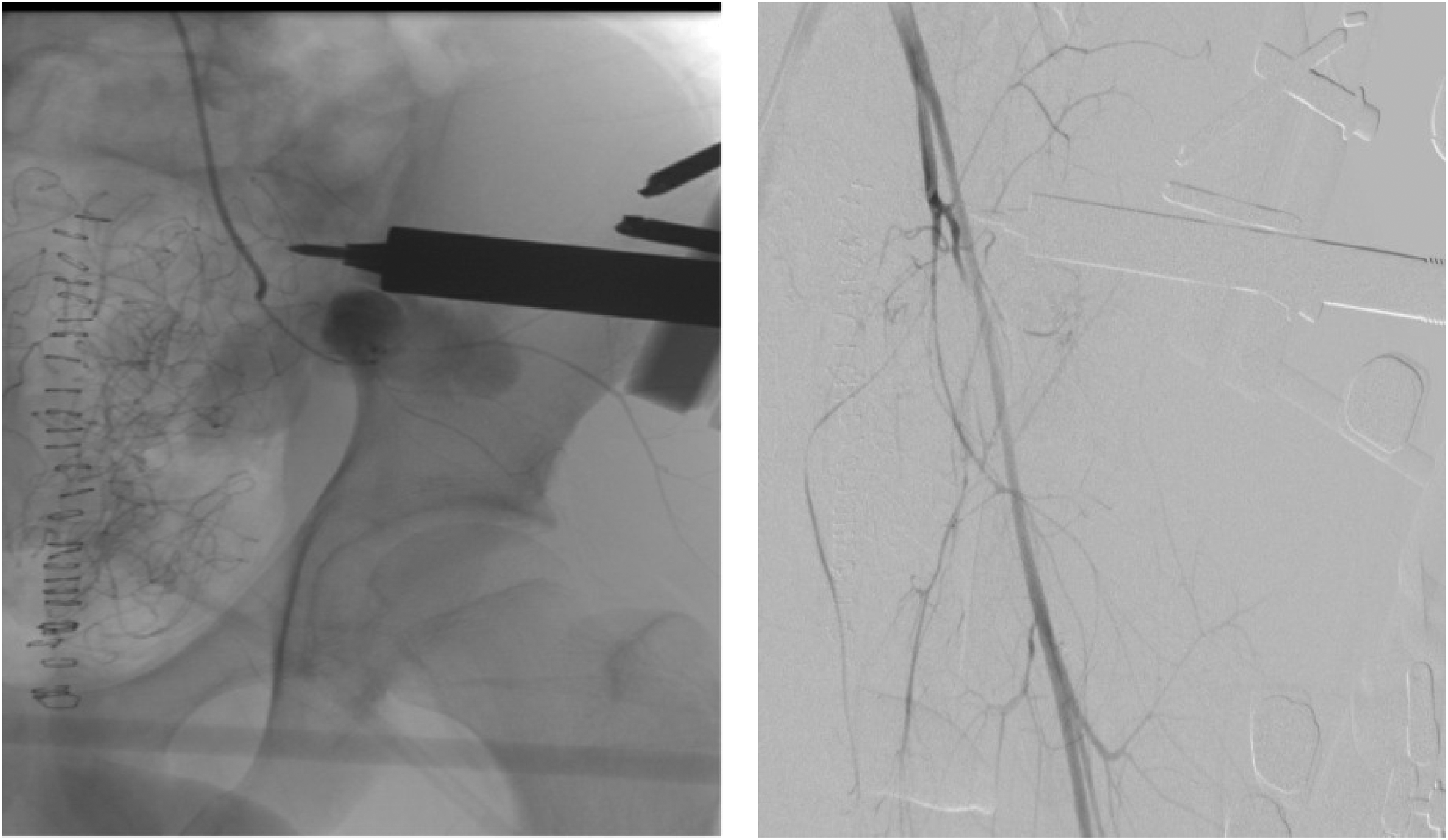
Angiogram showing active contrast extravasation from a branch of left internal iliac artery posterior division (left) embolization of the branch with gelfoam was done with cessation of extravasation (right).
Results
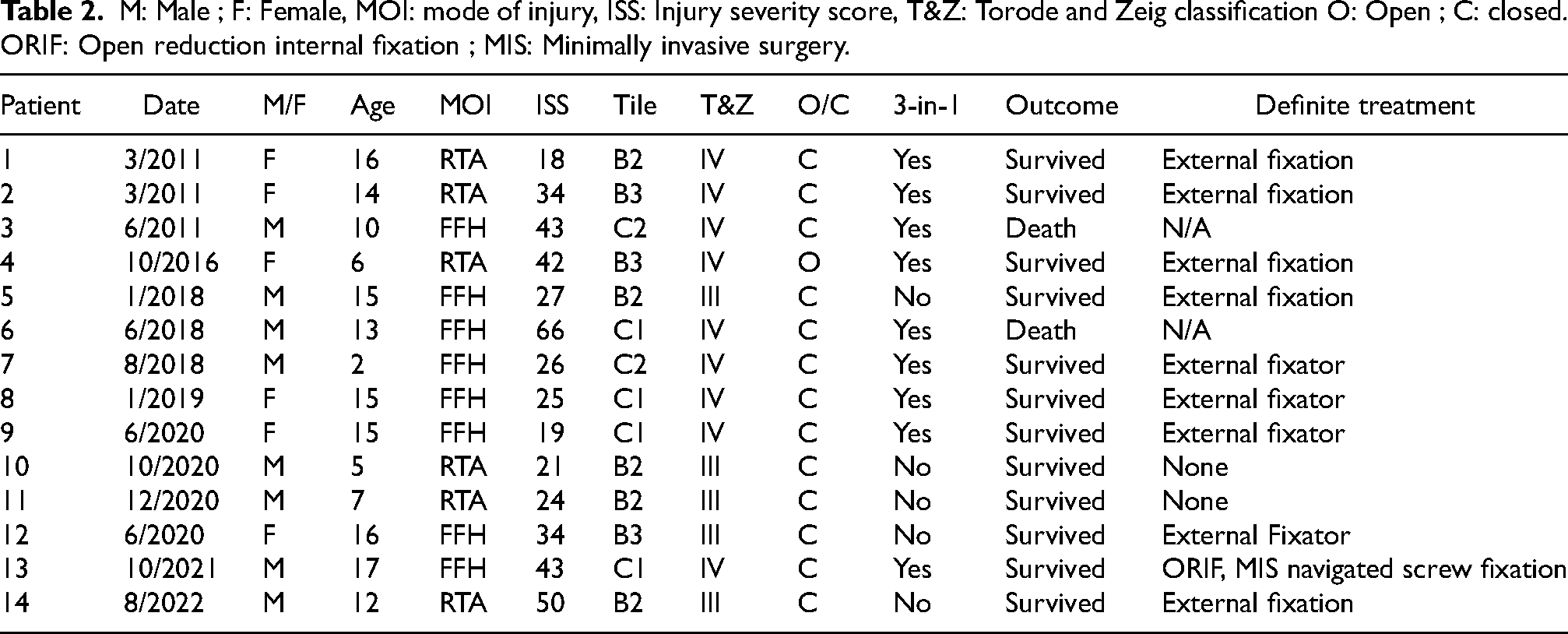
For the study period, there were a total of 14 patients who were admitted to our centre with pelvic fracture and activation of trauma call. The average age is 11.6. The median injury severity score is 30.5, interquartile range 19 using the version modified by Baker et al. 8 Of these, 9 patients (64.3%) were partial responders or non-responders who underwent 3-in-1 management. Three patients (21.4%) were responders who underwent pelvic external fixation alone for management of unstable fracture pattern or pelvic asymmetry. Another two (14.3) had physiological derangement caused by associated injuries, with conservative management employed for stable pelvic fracture pattern. The survival rate at index hospital admission and at one year is 85.7% (n = 12). They were discharged home as their final outcome. Four to six weeks of external fixation was used as the definitive management of pelvic fracture in nine patients (64.2%). Open reduction and internal fixation (ORIF) combined with minimally invasive (3D-navigation guided) pelvic screw was used in 1 patient (7.1%).
8 patients (57.1%) sustained injury by falling from height, whereas 6 patients (42.9%) were involved in road traffic accidents. All of the patients had associated injury. Thoracic and extremity injuries were the most common (n = 9, 64.2%), followed by head injury (n = 8, 57.1%), vertebral injury (n = 5, 35.7%) and abdominal injury (n = 3, 21.4%) (Table 1). Using Tile classification of pelvic fracture, Tile B was the most common (n = 8, 57.1%), followed by Tile C (n = 6, 42.9%). Using the Torode and Zeig classification, type IV was the most common (n = 9, 64.2%), followed by type III (n = 5, 35.7%) (Table 2). Figures 8 and 9 illustrate a Tile C2 and Torode and Zeig Type IV pelvic fracture.
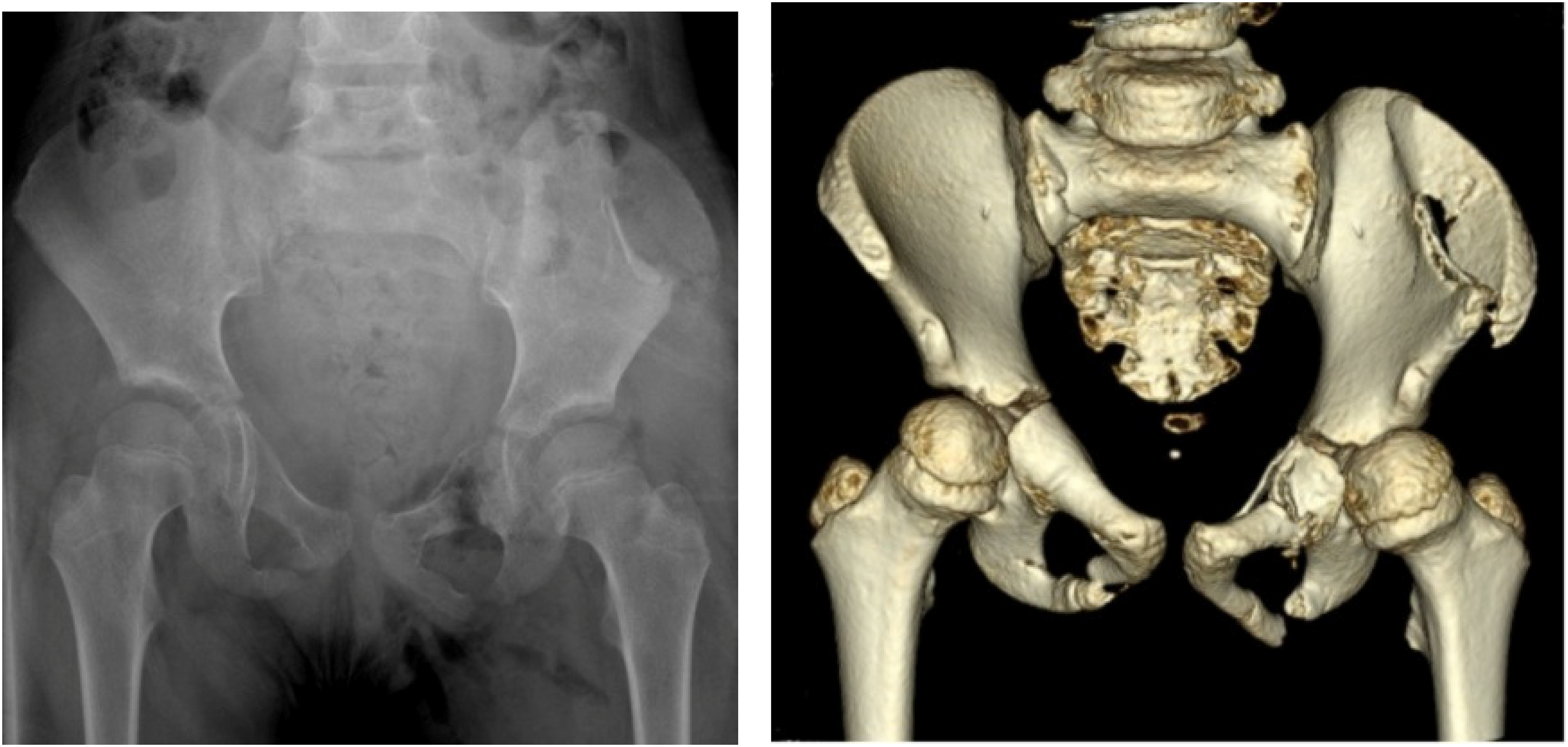
X-ray and CT pelvis of patient 4 showing Tile B3 and Torode and Zeig type IV pelvic fracture with hemodynamic instability. 3-in-1 protocol was implemented.
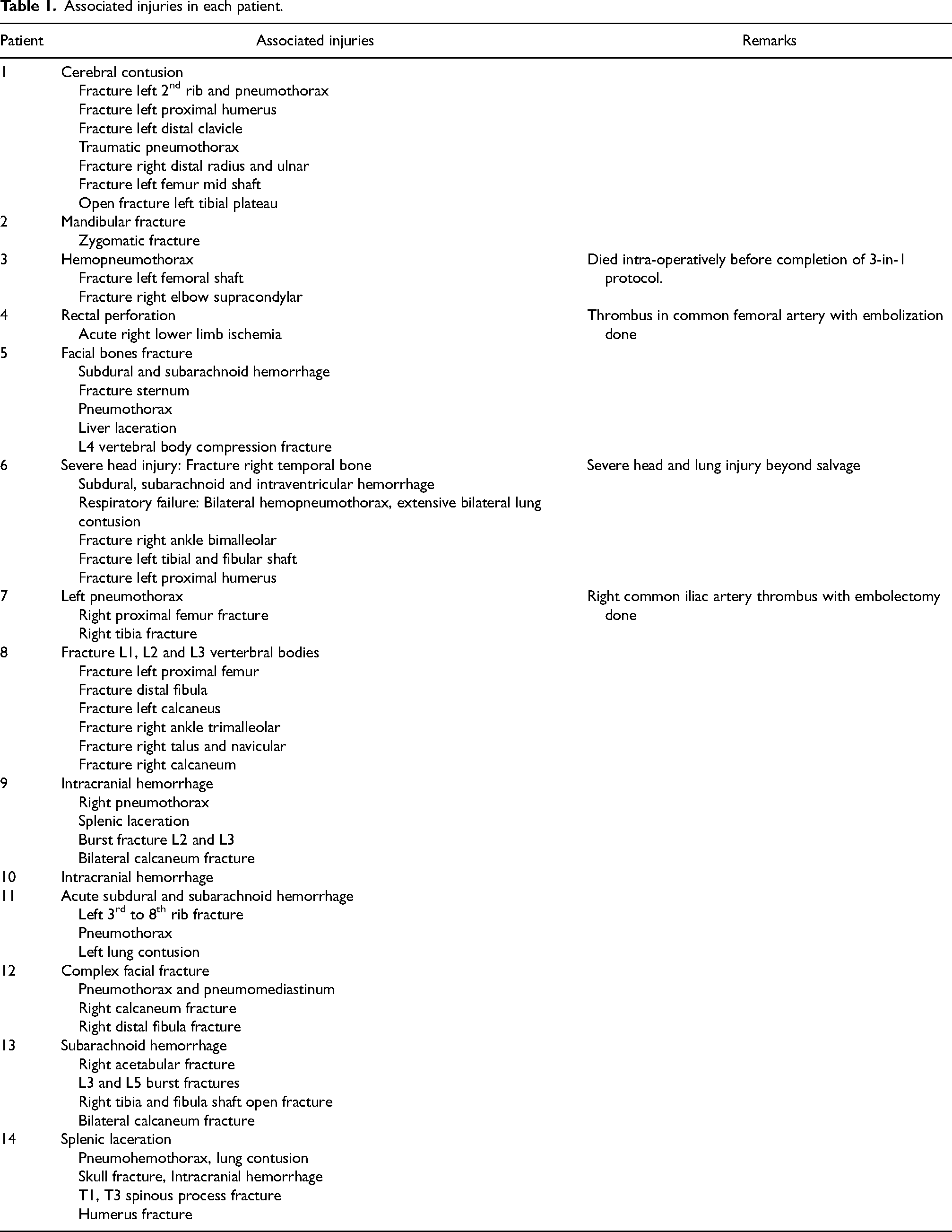
Associated injuries in each patient.
M: Male ; F: Female, MOI: mode of injury, ISS: Injury severity score, T&Z: Torode and Zeig classification O: Open ; C: closed. ORIF: Open reduction internal fixation ; MIS: Minimally invasive surgery.
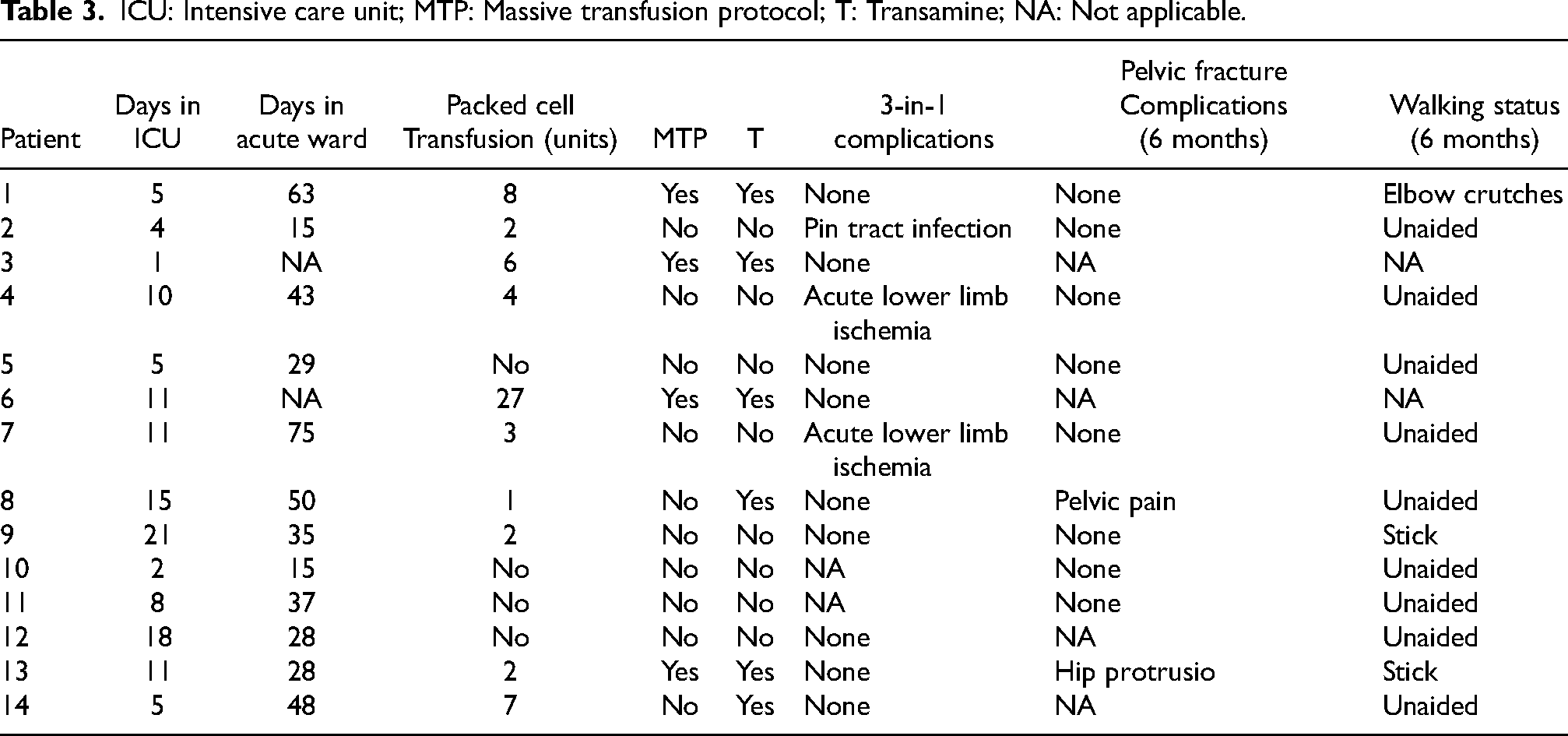
The median and interquartile range of ICU stay are 9 and 6 days, respectively. The median and interquartile range of acute ward stay are 36 and 21 days respectively. Packed cell transfusion was given in 10 patients (71.4%) and the average given in 24 h is 4.4 units. Massive transfusion protocol (MTP) was activated in 4 (28.5%) patients. Transamine was given in 6 patients (42.8%). One patient (7.1%) developed pelvic pin tract infection at post operative 6 weeks and the infection resolved after external fixator removal. Two patients (14.2%) developed acute lower limb ischemia which is from the same side as the angiogram arterial access at post operative day one. Both underwent embolectomy with no further complications. All survived cases have been followed in outpatient clinic for at least 6 months. All patients had pelvic fracture healed within 6 months. One patient (7.1%) with acetabular-pelvic fracture had gradual hip protrusion which became static at 6 months. One patient (7.1%) had pelvic pain. None of the patients had pelvic asymmetry, leg length discrepancy, or scoliosis. Nine patients (75%) walked unaided, while three (25%) walked with elbow crutches or stick, which are attributed to underlying calcaneum and tibia fracture (Table 3).
ICU: Intensive care unit; MTP: Massive transfusion protocol; T: Transamine; NA: Not applicable.
The first patient in the mortality group was a 10-years-old boy who had hemopneumothorax in addition to pelvic fracture. His ISS was 43. Three-in-one management was initiated. After external fixation was done, he was found to have progressive abdominal distension. Midline laparotomy was done after retroperitoneal packing showing rapid exsanguination through posterior peritoneum breach with intact visceral organs. He succumbed before the initiation of angiogram. The cause of death was rapid exsanguination from the pelvis and thorax.
The second patient was a 13-years-old boy who had significant intracranial bleeding, hemopneumothorax, splenic and liver laceration in addition to his pelvic fracture. His ISS was 66. Three-in-one management protocol was implemented. Right frontal and temporal lobectomy was done, but he eventually succumbed to an unsalvageable brain injury.
Discussion
As one of the major trauma centres in Hong Kong, the three-in-one protocol as described above has been developed since 2008 for the management of hemodynamically unstable pelvic fracture. The development of this protocol evolved from improved survival from 27% in phase I (1996–2001) with external fixation alone, to 57% in phase II (2002–June 2008) with added angio-embolization, and to 81% in 2015 when all three procedures were performed in our centre.1,9 We believe all the three procedures are tackling different bleeding sources within the pelvic cavity and are complementary and supplementary to each other.
In the paediatric population, the overall mortality rate has been quoted to be 8.6–25%10,11 and is comparable to the adult population. In our series with a higher rate of unstable pelvic fracture pattern (64.2% versus 34.8% Type IV Torode and Zeig fractures, 42% versus 14% Tile C fractures) and a higher mean ISS (31.6 versus 16.7) compared to previous studies, the mortality rate is 14.2%. 12 The severity of injury could also be reflected in the higher average of patients requiring blood transfusion (64.2% versus 34.1%) compared to previous studies.1
One patient (7.1%) had died as a direct result of pelvic fracture-induced exsanguinations (Patient 3), echoing the importance of the concept of retroperitoneal tamponade effect in pelvic fracture management. Another patient died from traumatic brain injury and intra-abdominal injuries (Patient 6).
It has been suggested that the mortality rate observed in the paediatric group is attributed to associated injuries, in particular traumatic brain injury and intra-abdominal injury, rather than the pelvic fracture itself. Postulations to explain this include the increased elasticity in the skeletally immature pelvis due to higher amount of cartilage and the open triradiate cartilage, smaller and less sclerotic vessels which are more capable of vasoconstriction, and higher rate of lateral compression injury. 13
Nevertheless, major pelvic fractures could produce significant hemorrhage, the risk of which increases with increasing instability of the pelvic ring.14,15 In our locality, where most residential areas are in the form of tall buildings, falling from height was the most common mechanism of injury. This is in contrast with previous series, which showed road traffic accident as the most common form of injury.1,16 This difference could explain a high rate of Tile C, Type IV Torode/Zeig and hemodynamically unstable fractures observed in our series.
The importance of controlling haemorrhage in a timely manner is not limited to direct deaths and multi-organ failure sequelae that occur from pelvic-related exsanguination. 17 The deadliest associated injury is traumatic brain injury 18 and there is evidence that its lethality is contributed significantly from concomitant blood loss from the pelvis, or any source for that matter.19,20
There are a few differences in the management of exsanguinating pelvic fracture in the paediatric population compared to adults. Firstly, the interpretation of haemodynamics is different due to different circulatory physiology in the paediatric population. The paediatric group have good physiological reserve, sustaining arterial pressure even with blood volume loss of 25% to 40%. This should be kept in mind when classifying children into responders, partial responders, and non-responders to fluid resuscitation. 21 Fluid resuscitation and vigilant interpretation of the vital signs as described above are varied according to age and body weight. In our study, massive transfusion protocol (MTP) was activated in 28.5% patients. However, 64.2% of patients were partial or non-responders with three-in-one protocol activation. In the latter group, packed red blood cell, fresh frozen plasma, and platelet were given to every patient, but MTP was activated only in some cases, particularly the non-responder group. Indeed, the activation and ratio of blood products of MTP in the paediatric group is less clearly defined compared to the adult counterpart. 22 However, it is important not to delay the release and transfusion of blood products. Future data to develop a targeted transfusion protocol with age stratification with an optimal blood products ratio would be beneficial in the paediatric group. Transamine is given early with a dose of 15 mg/kg for patients less than the age of 12, with a maximum dose of 1 g.
Secondly, adult pelvic binders may not fit paediatric patients. The standard pelvic binder fits a hip circumference of 81–129 cm. There are commercially available paediatric pelvic binders with half of the circumference. Based on our experience, T-pod pelvic binder was used in most cases in this series after trimming or folding the length of the binder before tightening. Nevertheless, in settings where an appropriate binder is not available, bed sheets with clamps which are readily available in any hospital setting could be used as an alternative. As long as timely application of the pelvic binder centred at the level of greater trochanter at appropriate tension is applied, it can serve to protect the precious first blood clots within the pelvic cavity. It is ideal to apply pelvic binder at the site of injury by trained personnel such as an ambulance man, before arrival to hospital.
Thirdly, the technical aspects differences for the three-in-one protocol. At our centre, Hoffmann II external fixator as described above is being used. At our centre, 5 mm Apex pins are commonly used in adult patients. This also applied to most patients in this series except for the 2-years-old child in which 4 mm pins were used (patient 7). Paediatric patients have smaller iliac crest bone with relatively thicker periosteum and are able to accommodate two to three 4 mm or 5 mm pins securely. The external fixator construct is similar to the adult counterpart. C-clamp is used generally at age 12 or above with an appropriate sized pelvis. The youngest patient who underwent C-clamp fixation in our study was 13 years old.
Both of the patients with lower limb ischemia after three-in-one procedure were found to have absent lower limb pulses on post-operative day 1 despite catheter sheath removal. Urgent embolectomy was done to retrieve clots from the common femoral artery in one patient and from the common iliac artery in another. 5Fr sheath was used for artery access in one patient and 4Fr in another. 4Fr catheter is preferred and the catheter sheath should be removed immediately post angiography to minimize the risk of thromboembolism. The relatively high rate of lower limb ischemia suggest that embolization should only be used in paediatric patients with obvious contrast extravasation instead of being used as a universal prophylactic procedure.
As shown in previous studies, concomitant injuries are very common and are frequently life threatening. In our series, all of the patients had associated injury. The commonest are thoracoabdominal injury, (n = 8, 67%), extremity fractures (n = 7, 58% and head injury (n = 6, 50%). This is in line with previous studies and emphasizes the importance to detect and treat these injuries according to priority.
The difference in the skeletally immature pelvis compared to an adult pelvis has significance in interpreting pelvic radiographs. The elastic pelvis is more likely to deform than fracture in trauma. The result is that pelvic radiographs may show only asymmetry rather than obvious fracture. In addition, as higher energy is needed to deform or fracture the pelvis, there is a higher rate of single-bone pelvic ring fractures, rather than the typical double break seen in adult pelvic fractures. 23 Hence, one should be alert to pelvic injury and also intra-abdominal injury in the setting of high-energy trauma even in the absence of major pelvic fracture. However, the assessment of hemodynamic status should be prioritized over pelvic fracture classification in the initial resuscitation.
There remains a lack of strong evidence to indicate fractures that should undergo surgical fixation, more so the definite type of fixation. Generally, there is an increasing trend for operative management of unstable pelvic fractures with asymmetries and displacements. Recent studies have shown that the fractured paediatric pelvis lack the ability to remodel, and will remain in the position it is displaced at. This would lead to complications like pelvic asymmetry, leg length discrepancy, chronic pain, scoliosis and limping.13,24 Implant choice and approach of fixation are varied, with external fixation being an appropriate choice for stabilization of the pelvis. 25
In our series, external fixation was used as the definitive management of pelvic fracture in 9 patients (64.2%). ORIF combined with minimally invasive pelvic screw was used in 1 patient (7.1%) with acetabular and pelvic fracture. In our series at 6 months follow up, one patient (7.1%) had pelvic pain, and 1 patient (7.1%) with acetabular pelvic fracture had hip protrusion. He was patient 13, a 17-years old boy who fell from height with a Risser stage 4 pelvis. He had a Tile C1 and Type IV Torode/Zeig pelvic fracture and underwent ORIF combined with minimally invasive pelvic screw fixation. Subsequent X-rays showed progressive hip protrusion which had stabilized (Figures 10 and 11).
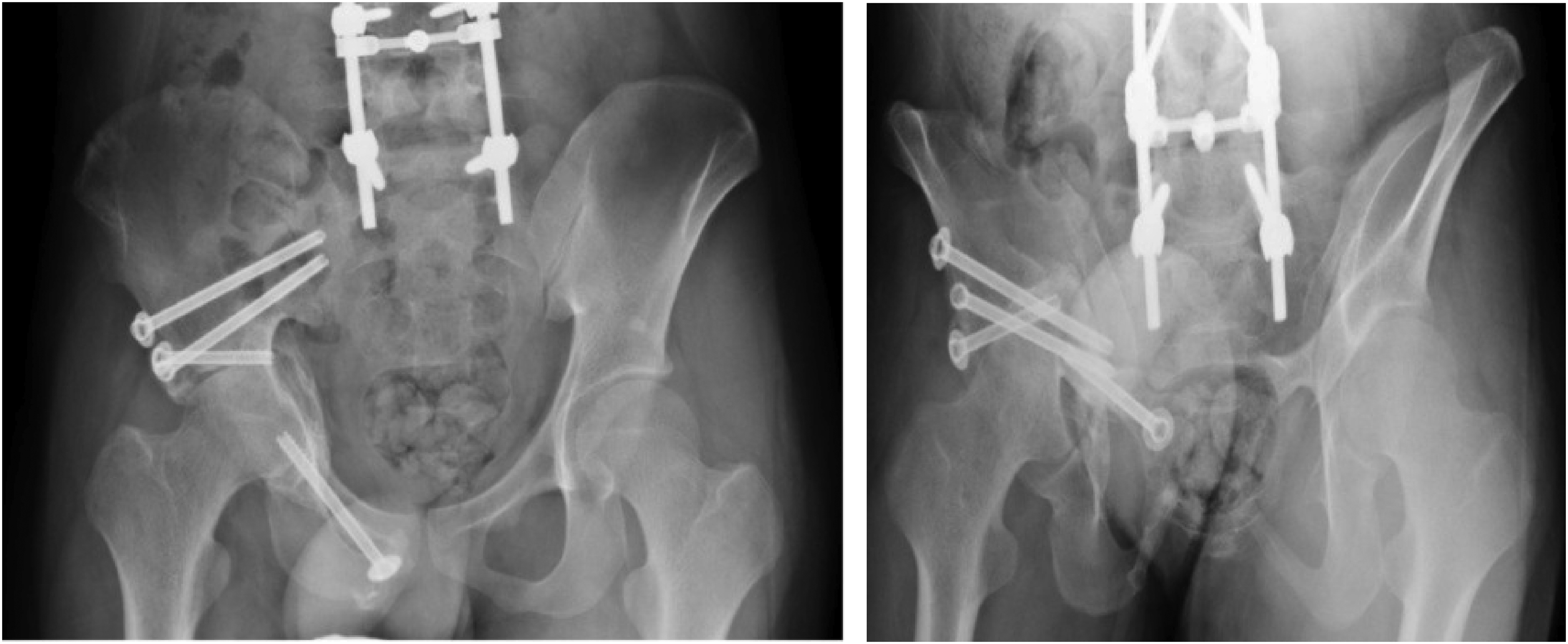
X-rays of patient 13 with right hip protrusion at 6 months after ORIF combined with 3D navigated screw fixation was done.
There are two limitations to this study. Firstly, there is no comparison of survival rate in paediatric patients before and after the implementation of three-in-one protocol. The comparison of survival rate to that of the adult group is not ideal as it is hypothesized that the extent and physiological response are different in the paediatric group, as described above. Secondly, the long-term functional outcome has not been included in this study. Indeed, more studies are needed to evaluate the indications, methods, and outcome of surgical fixation in paediatric pelvic fracture.
Conclusion
Three-in-one protocol for the management of hemodynamically unstable pelvic fracture is a fast and effective procedure to control exsanguination from the pelvis in the paediatric group, with a higher survival rate than the adult population. Technical differences in the paediatric group in particular the use of embolization is highlighted to reduce potential complications.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.