
Abstract
Purpose
To assess health literacy (HL) of patients with total knee arthroplasty (TKA) and evaluate its impact on patient reported outcome measures (PROMs) as well as investigating outcome differences in inpatient and outpatient rehabilitation.
Methods
In this study, HL and PROMs of older patients were assessed preoperatively (T0) and after 3 (T1), 6 (T2), and 12 (T3) months. HL was assessed with the short form of the European HL Questionnaire; pain scores, functional restrictions, and activity levels with standardized PROMs.
Results
Limited HL was observed in 70.6% of patients at T0. HL improved from baseline to follow-ups (p < 0.001). There was no impact of HL on PROMs. Pain scores were higher in patients undergoing outpatient rehabilitation (p = 0.022). No differences were found between the rehabilitation settings for the other outcomes.
Conclusion
The study shows that limited HL is prevalent in patients with scheduled TKA. Rehabilitation seems to have a positive effect on increasing HL.
Introduction
Patient education in the context of rehabilitation after knee arthroplasty focuses on relearning movement patterns with the new joint, integrating health-promoting behaviours into everyday life and changing harmful behaviours. 1 Information, instruction and counselling are intended to strengthen the patient's competence in everyday life. Health literacy is seen as a key competence to understand information provided by healthcare professionals and to be able to apply it individually to one's own situation. 2
However, research has shown that patients often have difficulties in understanding instructions and information they receive from healthcare professionals.3–6 An important goal of an empowering patient education programme is to promote patients’ health literacy to enable effective self-management throughout the rehabilitation process and beyond. 7 Limited health literacy is a growing public health problem globally. 8 More than half of the European population has limited health literacy. 9 Comparable results can be found in the USA 10 or in Canada. 11 Health literacy is understood as the cognitive and social skills as well as the motivation to access, understand and thus use relevant health information to maintain and improve one's own health and quality of life. 12
Poor health literacy is associated with several negative health-related outcomes, such as increased hospitalization, 13 lower preventive behaviour, 14 poorer adherence to medical treatments, 15 and higher mortality. 13 Health literate people, on the other hand, take a more active role in the treatment and care process, are able to make informed health decisions and have higher chances of achieving better health-related outcomes. 2 Low health literacy has been observed in people with generally poor health, low socioeconomic status, low education levels, intellectual disability, and older age.9,16
For surgical procedures such as total knee arthroplasty (TKA), health literacy includes patients’ understanding of their health status, the procedures and postoperative treatment plans. 17 Postoperatively and throughout the course of orthopaedic rehabilitation, patients receive health information and instructions for rehabilitation that are essential for effective self-management and can prevent complications. 18
Rehabilitation after knee arthroplasty can be provided on an inpatient or outpatient setting. 1 Several studies have demonstrated significant cost reductions in favour of outpatient rehabilitation programmes.19–21 Due to improved surgical outcomes, 22 discharge to inpatient rehabilitation facilities has decreased in recent years. 23 In outpatient programmes, new skills learned in patient education can be applied directly in everyday life. However, this means that health literacy is increasingly important for effective self-management. 24 In terms of clinical outcomes, there is no consistent evidence comparing inpatient and outpatient rehabilitation after knee arthroplasty to date. 25
The aim of this study was to assess health literacy of patients undergoing TKA and to observe its development during orthopaedic rehabilitation. Furthermore, associations between health literacy and clinical outcomes as well as outcome differences between an inpatient and an outpatient setting were to be investigated.
The guiding research questions were as follows:
How does the health literacy of older adults with TKA evolve throughout a rehabilitation period of one year? How does health literacy affect clinical outcomes of rehabilitation following TKA? What are the outcome differences between inpatient and outpatient rehabilitation?
Methods
Study design
In this prospective observational study, we repeatedly assessed the health literacy of patients with TKA in a region in the west of Austria using the validated German-language HLS-EU-Q16 questionnaire and various patient-reported outcome measures (PROMs). The follow-ups were conducted between 2019 and 2021.
Setting and participants
The study was conducted in a private orthopaedic practice. Patients were admitted to the practice preoperatively for a preliminary medical consultation and were informed about the study verbally and in writing. Eligible patients were enrolled in the study after providing written informed consent. Patients over 50 years of age with scheduled knee arthroplasty were included. Patients under 50 years of age, those unable to complete a questionnaire independently, and secondary and revision arthroplasty were excluded. Postoperative orthopaedic rehabilitation was provided at various inpatient or outpatient rehabilitation facilities on discharge from the hospital where the patients underwent surgery. Total recruitment period of the study participants was thirteen months (from May 2019 to May 2020). The sample was a non-probabilistic convenience sample.
Data collection
Data collection on health literacy and clinical outcomes was conducted using paper-based self-report questionnaires. Baseline data were collected before surgery (T0), follow-up data were collected three months (T1), six months (T2) and twelve months (T3) afterwards. Figure 1 illustrates the process of the observational study based on a flow diagram. All data collection in the study was conducted in the orthopaedic practice. At T1, participants had completed an inpatient or outpatient rehabilitation programme. The study authors had no influence on the patients’ decision for inpatient or outpatient rehabilitation, so there was no random allocation. Questionnaires were used at each follow-up time point to record whether the participants had completed a rehabilitation programme in the last three months and whether this was carried out on an inpatient or outpatient setting.
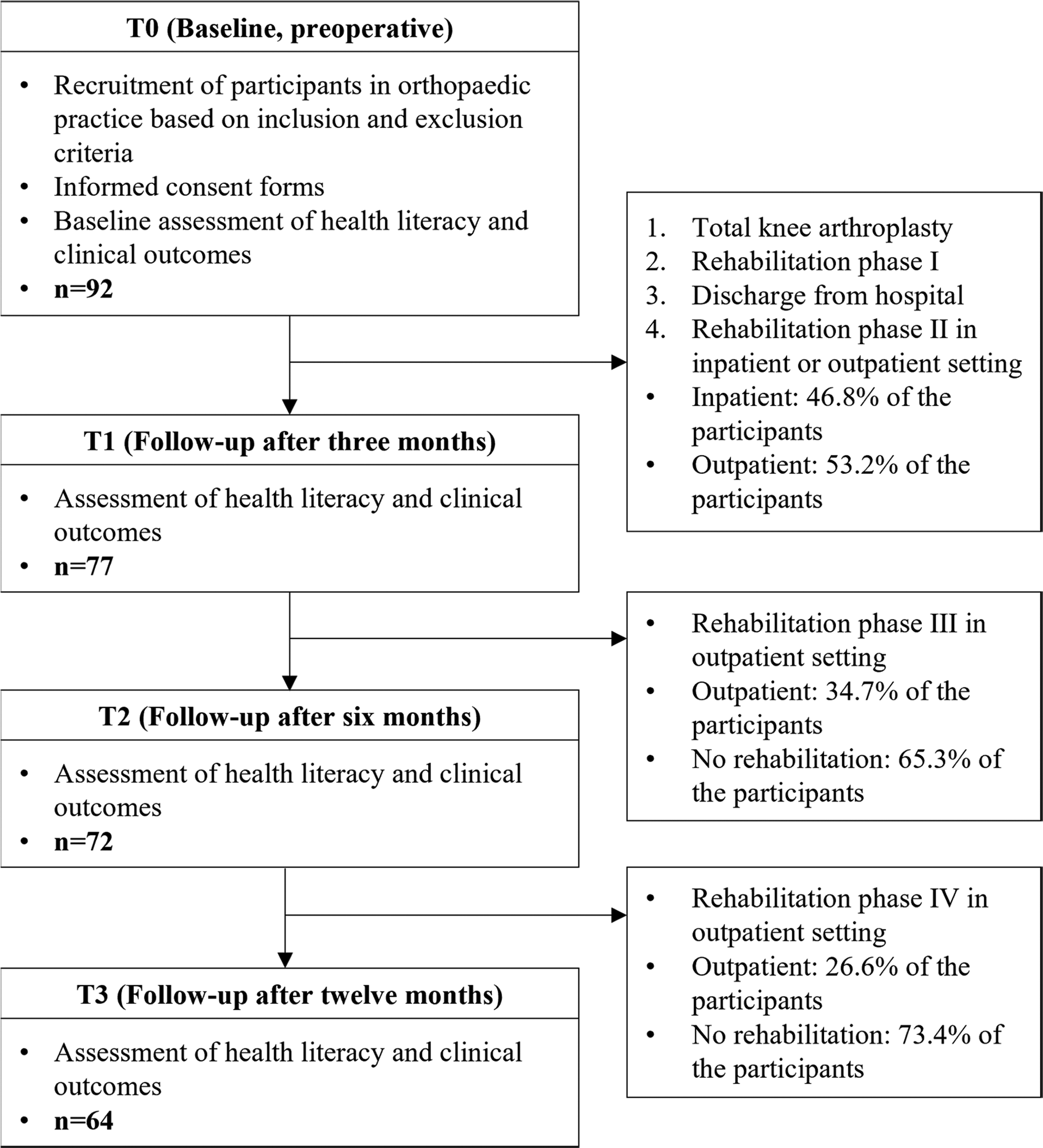
Flow diagram of the longitudinal observational study.
Assessment of health literacy and clinical outcomes
Health literacy was assessed with the validated German-language short form of the European Health Literacy Questionnaire (HLS-EU-Q16). 26 The questionnaire was developed as part of the European Health Literacy Survey to measure the comprehensive concept of health literacy. 9 The questionnaire aims to assess the four dimensions of health literacy (access, understanding, appraisal and application of health information) in the dimensions of health care, disease prevention and health promotion. 26 Due to the limited practicability of the long version with 47 items and an average completion time of about 10 min, the European Health Literacy Consortium developed the short form HLS-EU-Q16. The questionnaire represents all essential dimensions of the underlying health literacy model in a balanced way, as shown by the results of face and content validity. 27 The HLS-EU-Q16 has very good internal consistency (Cronbach's α = 0.90). 28 All items are formulated as questions and are answered by self-assessment of the respective item content on a four-point Likert scale from very easy to very difficult. 29 The scale score is calculated as a total score and varies from 0 to 16 points. The level of health literacy was defined as inadequate (0–8 points), problematic (9–12 points) and adequate (13–16 points) health literacy, whereby problematic and inadequate health literacy are summarized under limited health literacy. 28
Clinical outcomes were collected using PROMs. PROMs, commonly used in orthopaedics, focus on physical and functional aspects of patients such as pain, mobility, joint function, and activities of daily living. 30 In this study, PROMS were used to assess pain, functional restrictions, and physical activity. Pain status was assessed using a visual analogue scale (VAS). The VAS is a single-item scale that assesses the degree of pain using 11 points. The extreme points represent “no pain” and “severe pain”. The score given is quantified using a defined scale of 0 to 10 points. 31
Functional limitations were assessed using the Oxford Knee Score (OKS). The OKS questionnaire is a PROM consisting of 12 questions covering the physical function and pain subscales of total knee replacement patients. The German version of the OKS is considered a valid and reliable instrument. 32 Each question is scored on a scale from 1 to 5, with 1 being the worst and 5 the best The total score is the sum of all questions and ranges from 12 to 60, with higher scores representing better results.
Patients’ activity levels were assessed using the Tegner Activity Scale (TAS), which includes 11 differently weighted activity levels that measure the physical activity of patients with knee joint structure disorders. The activity levels are presented as scores and range from 0 to 10 points. Zero points describe the lowest physical activity, while 10 points represent the highest physical activity. The psychometric properties of the German version, especially content validity and discriminant validity, correspond to those of the English original, which classify the scale as a valid and reliable instrument and is recommended as a gold standard. 33
All PROMs were recorded as separate scores using a paper-based questionnaire (VAS score: 0–10 points; OKS score: 12–60 points; TAS score: 0–10 points). The patients’ health literacy (HLS-EU-Q16 score: 0–16 points) and the rehabilitation setting (inpatient or outpatient) were recorded with a second paper-based questionnaire.
Statistical analyses
Results are presented as absolute and percentage frequencies (n, %), means and standard deviations (M ± SD) (Table 1) and graphically using boxplots (Figure 3). Differences in health literacy at baseline and follow-ups were assessed using the Friedman test with Dunn-Bonferroni post hoc test For the analysis of differences in clinical outcomes in relation to health literacy levels, the three-month follow-up data (after rehabilitation phase II) were used. For this purpose, the sample was divided into three subgroups representing participants with adequate, problematic, and inadequate health literacy. The differences between these subgroups were calculated for each PROM using the Kruskal-Wallis test To investigate outcome differences in relation to the rehabilitation settings (rehabilitation phase II), subgroup analyses for inpatient and outpatient rehabilitation settings were conducted using the Mann-Whitney U test A p-value of ≤ 0.05 was considered statistically significant. The statistical analyses were performed using IBM® SPSS® Statistics software version 25.0.
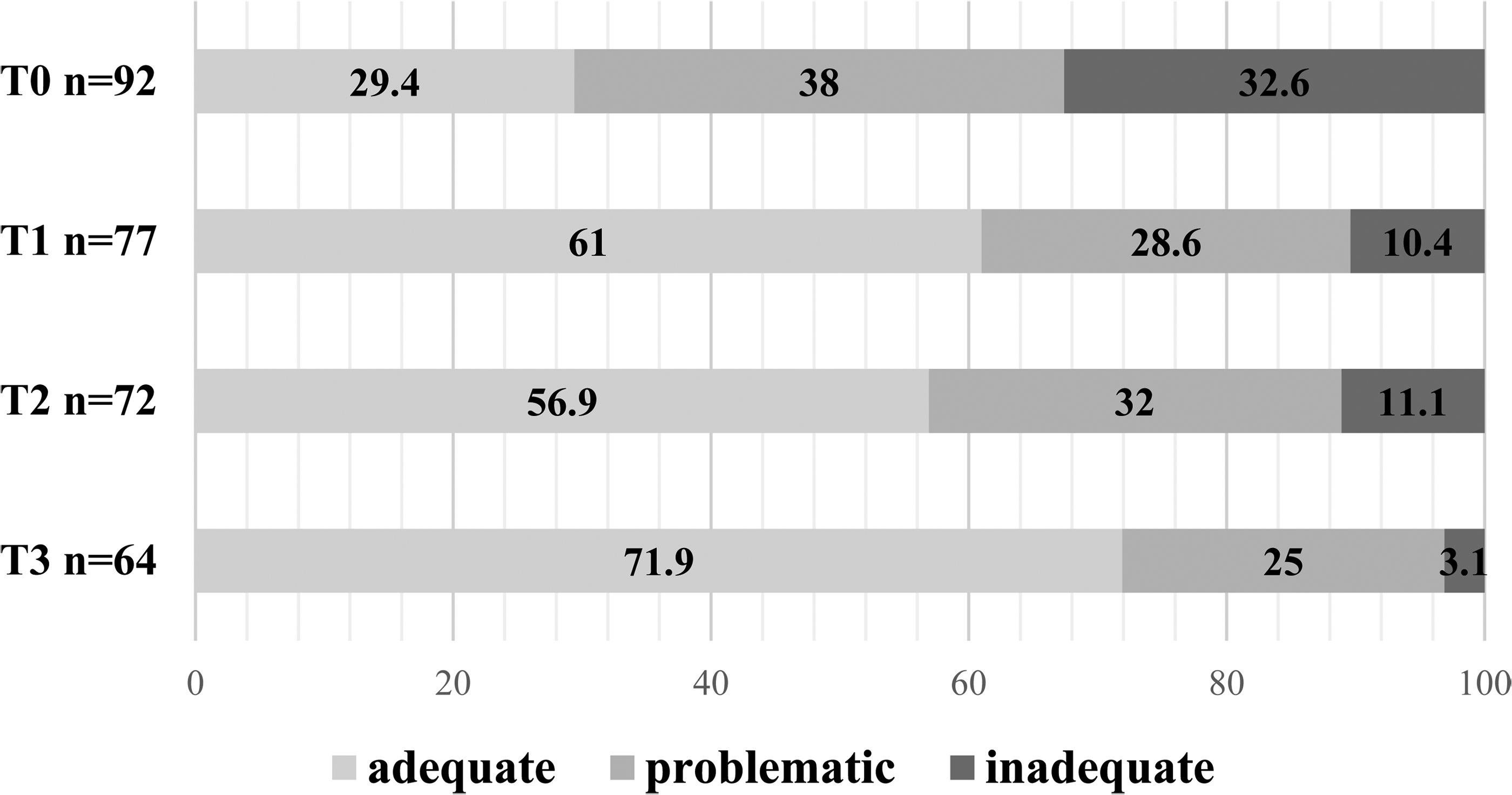
Changes in health literacy levels during the course of rehabilitation.
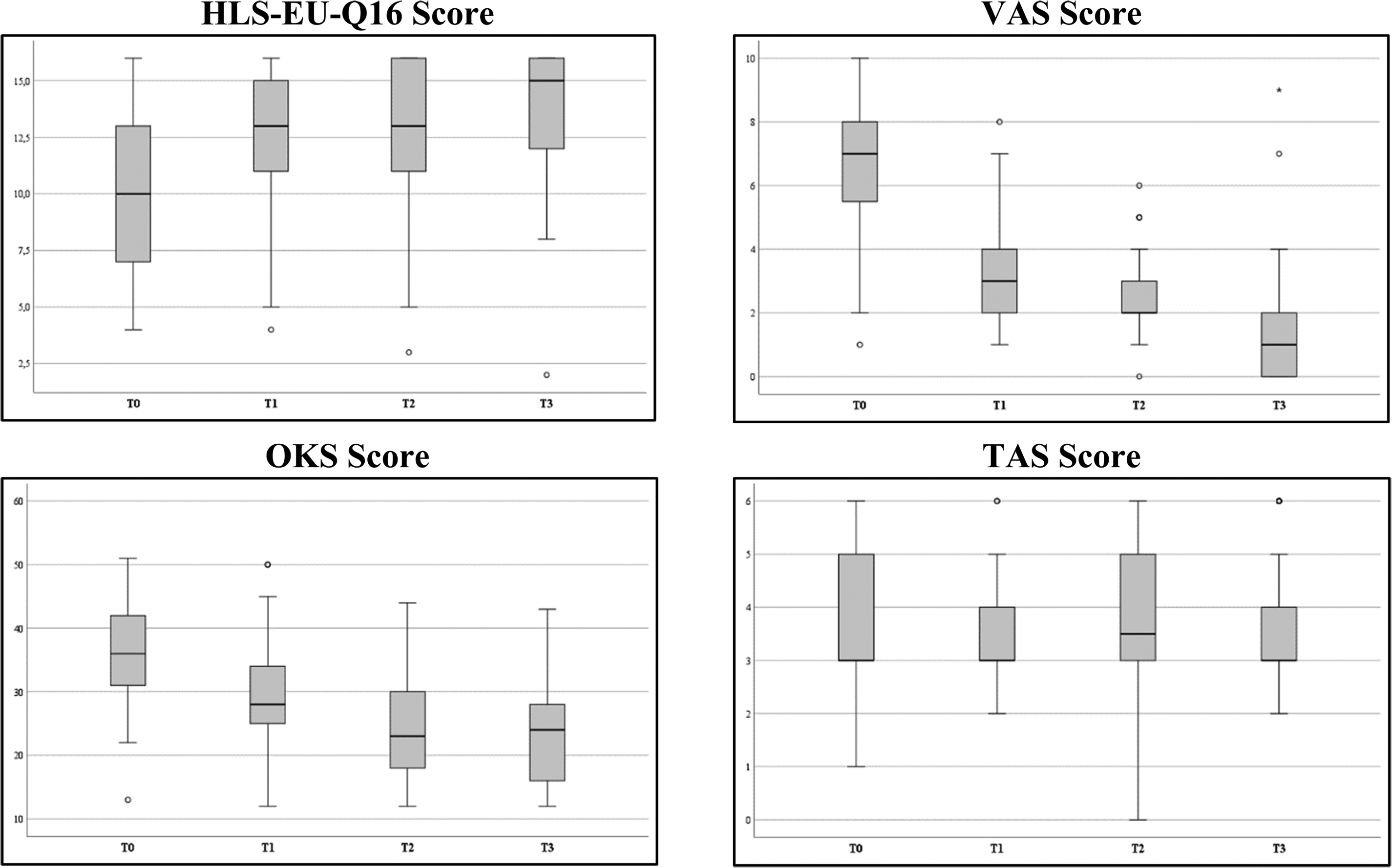
Trends in health literacy (HLS-EU-Q16), pain (VAS), physical restrictions (OKS) and physical activity (TAS) in the course of rehabilitation over one year (T0–T3).
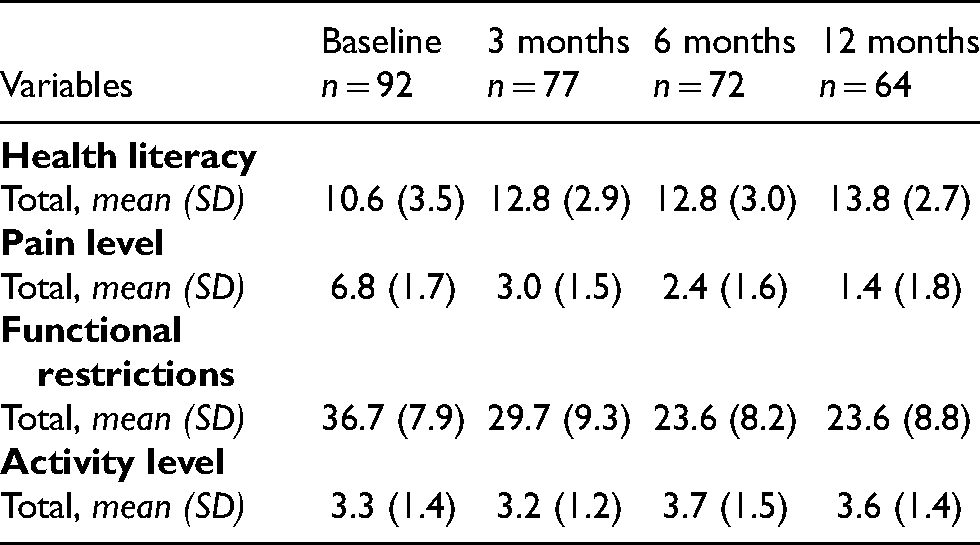
Descriptive data of health literacy and clinical outcomes (PROMs) at baseline and follow-ups.
Results
Participants
The study cohort consisted of 92 patients with scheduled TKA, the majority were men (n = 56; 60.9%), and their mean age was 67.9 (±10.3) years. The mean age of women was 72.0 (±6.4) years. Seventy-seven patients (83.7%) completed a rehabilitation programme between T0 and T1 (46.8% inpatient and 53.2% outpatient rehabilitation). Between T1 and T2, 34.7% completed further outpatient rehabilitation (phase III), while 65.3% did not take up additional phase III rehabilitation. Between T2 and T3, 26.6% received further rehabilitation services. At T1, 15 patients were lost to follow-up, at T2 another five patients and at T3 another eight patients. No reasons were stated for dropping out of the study.
Health literacy and clinical outcomes
Preoperatively, 29.4% of the patients had adequate health literacy. In contrast, 70.6% had limited health literacy. After rehabilitation phase II, 61% of the patients had adequate health literacy. This distribution remained stable at T2 and improved again at T3. Figure 2 shows the health literacy levels of the participants at all four time points.
Health literacy improved significantly in the average HLS-EU Q16 score with a small effect size from T0 to T1 (p < 0,001, r = 0,1), from T0 to T2 (p < 0,001, r = 0,1), and from T0 to T3 (p < 0,001, r = 0,2). The average scale scores of health literacy and clinical outcomes at all four time points are shown in Table 1. The first column lists the variables health literacy and PROMs. The other columns contain the data collected at the four time points.
The boxplots in Figure 3 depict the distribution of the data graphically for a simplified representation based on a five-number summary (“minimum”, first quartile, median, third quartile and “maximum”). For each variable, four boxplots are presented (one per time point) to illustrate the trend over time.
Impact of health literacy on clinical outcomes
To analyse associations between health literacy and clinical outcomes (pain scores, functional restrictions, and physical activity) after rehabilitation phase II, three subgroups were formed based on health literacy levels (adequate, problematic, and inadequate). Clinical outcomes improved equally in all groups regardless of health literacy level. There was no statistically significant difference in pain scores between health literacy subgroups (χ2(2) = 1.126, p = 0.570), with a mean rank pain score of 37.04 for adequate health literacy level, 41.33 for problematic health literacy level and 44.50 for inadequate health literacy level. No statistically significant difference was found in functional restrictions between the different health literacy levels (χ2 (2) = 1.068, p = 0.586), with a mean rank OKS of 36.91 for adequate health literacy level, 42.04 for problematic health literacy level and 43.00 for inadequate health literacy level. There was also no statistically significant difference in patients’ activity levels between health literacy levels (χ2(2) = 2.361, p = 0.307), with a mean rank Tegner Activity level of 37.47 for adequate health literacy level, 38.65 for problematic health literacy level and 50.43 for inadequate health literacy level.
Outcomes in different rehabilitation settings
Differences in PROMs and health literacy were examined in relation to inpatient and outpatient phase II rehabilitation. Results showed that participants in outpatient rehabilitation had significantly higher pain scores than participants in inpatient rehabilitation (Z (noutpatient = 41, ninpatient = 36) = −2.29, p = 0.022, r = 0,3). No differences could be found in the outcomes of functional restrictions, physical activity, and health literacy between the rehabilitation settings.
Discussion and conclusion
Discussion
The aim of this study was to assess health literacy of older adults with scheduled TKA preoperatively and in the further course of rehabilitation. In addition, potential effects of poor health literacy on clinical outcomes as well as the influence of the rehabilitation setting were to be demonstrated. The study results indicate that, on average, patients show problematic health literacy preoperatively. Following rehabilitation, health literacy improved significantly and remained largely stable in the further course of rehabilitation. Concerning the clinical outcomes, no differences could be found depending on health literacy levels. A comparison of inpatient and outpatient rehabilitation showed that the patients experienced significantly less pain after inpatient rehabilitation. There were no significant differences in the other outcomes in the setting comparison.
Development of health literacy throughout the rehabilitation period
Strengthening patients’ health literacy is an important goal of rehabilitation after TKA.2 This should be done through patient educational measures. 34 However, studies have shown that for patients educational content is often difficult to understand. 35 Especially people with limited health literacy have problems understanding health information and applying it situationally in everyday life. 18 The present study demonstrated that health literacy of patients with TKA was lowest preoperatively, increased significantly at three months follow-up (after phase II rehabilitation) and did not change significantly on average after six months. At the one-year follow-up, patients recorded a renewed increase in health literacy by one score point on average, although this was not a statistically significant improvement. Even though the average health literacy score increased from 10.6 (± 3.5) to 12.8 (± 2.9), the improved average score was merely at the threshold for adequate health literacy. This significant health literacy increase is thus only of minor relevance for practice (low effect size, r = 0.1). Subgroup analyses in relation to gender showed that on average women's health literacy improved slightly more, although their baseline score was already marginally higher. In a study by Cosic et al. an orthopaedic patient group showed limited health literacy, which did not significantly improve at follow-up. 8
In a more detailed data analysis, we examined the variation of individual items in the HLS-EU-Q16 from T0 to T1. Presumably, not all items of the scale are addressed in orthopaedic rehabilitation in the context of educational measures, but there are nevertheless items in this questionnaire that are relevant for the target group. For example, item 3 “understand what your doctor says to you” changed significantly from T0 to T1 (p < 0.001). Item 16 “judge which everyday behaviour is related to your health” also improved significantly (p = 0.010). The improvement in these items is probably due to the educational measures during orthopaedic rehabilitation, although causal conclusions are not permissible based on our study design.
To improve patients’ health literacy, patient education is crucial. 2 Patient education aims to develop skills to make informed health-related decisions that enable health-promoting measures to maintain or improve quality of life in the long term. 36 In rehabilitation, both frontal and interactive educational methods are used to promote patients’ cognition, motivation, emotion, and behaviour. The central elements of patient education in the context of rehabilitation are information about the disease and the therapy, training in self-observation and self-treatment, but also motivational strategies for lifestyle changes. 36 In addition to active patient participation, everyday information, practical exercises, motivation, and personal responsibility are essential for a good comprehensibility of the training content and the development of competencies. 37
Relationship between health literacy and clinical outcomes
The impact of low health literacy on health-related outcomes can be far-reaching. 13 The results of an observational study by Hälleberg Nyman et al. suggest that poor health literacy in patients undergoing day surgery is associated with worse postoperative recovery and lower health-related quality of life. 38 However, in the present observational study, no differences in clinical outcomes were found in relation to patients’ health literacy. Participants with inadequate health literacy did not differ significantly from those with problematic or adequate health literacy in terms of pain status, functional restrictions, or physical activity. Nevertheless, a representative study from Germany (n = 4845) found that limited health literacy, assessed with the HLS-EU-Q16, is associated with poorer physical health, lower physical activity, and unfavourable health behaviour. 26 Due to the small non-probabilistic convenience sample in the present study, negative effects of low health literacy on clinical outcomes cannot be ruled out. Also, effects of health literacy on other relevant patient outcomes, such as health-related quality of life or self-management skills, are still unknown in patients with TKA.
Inpatient versus outpatient rehabilitation
A comparison of inpatient and outpatient phase II rehabilitation indicated a significant difference in pain status. Participants in outpatient rehabilitation had higher pain scores compared to those in inpatient rehabilitation. No differences were observed in health literacy, functional restrictions, and physical activity. Due to the small sample size in the present study and the unequal, non-random distribution of patients between inpatient and outpatient settings, this result should be interpreted with caution. Nevertheless, it could be assumed that due to the 24-h care by health professionals in inpatient rehabilitation, the pain status of the patients is assessed more frequently and thus interventions are carried out more quickly. However, there is no scientific evidence for this explanation.
Published research results do not provide consistent evidence of outcome-related benefits depending on different rehabilitation settings. Some studies demonstrated improved health outcomes in outpatient rehabilitation,21,39,40 but most studies did not find significant differences.41–44 A systematic review indicates that there is no scientific evidence comparing the effectiveness of inpatient rehabilitation with outpatient rehabilitation in older people after total hip arthroplasty in the post-discharge period. 25 In the present observational study, participants completed different inpatient or outpatient rehabilitation programmes. Thus, a detailed insight into the specific interventions in the context of patient education was not provided. Further research should compare the differences of patient education interventions in inpatient and outpatient rehabilitation settings using controlled intervention studies. In this context, it would be valuable to investigate the effectiveness of health literacy interventions such as the teach-back technique.
Strengths and limitations
The longitudinal observational study provides valuable insights into the health literacy and its course of this target group. So far, health literacy research internationally, but especially in German-speaking countries, has been largely limited to cross-sectional surveys, which has not enabled the detection of developments over time.45–48 Until now there is limited evidence on health literacy among orthopaedic patient groups.
However, the generalisability of the results is strongly limited due to the selected sample. Participants were recruited from a private orthopaedic practice. Privately insured patients are not representative from a socio-economic perspective, as they usually have higher levels of education, which in turn is associated with increased health literacy. 18 Furthermore, only patients who were able to complete the questionnaires independently were included in the study. This may have led to the exclusion of people with generally low health literacy, such as those with intellectual disabilities. Therefore, it can be assumed that the situation in the general population is more problematic than our results show.
Conclusion
The study results indicate that health literacy of older adults with planned TKA needs improvement. Inpatient and outpatient rehabilitation programmes seem to enhance health literacy, even if this effect is minor. Impacts of limited health literacy on clinical outcomes could not be observed in this study. However, associations with other relevant patient-oriented outcomes are unknown for this target group. Patients who followed inpatient rehabilitation reported less pain than those after outpatient rehabilitation, which could indicate improved pain management in inpatient rehabilitation. Further research should evaluate the comprehensibility and motivational enhancement of patient education interventions as a key tool to improve health literacy in the context of rehabilitation after joint arthroplasty. Based on this, target group-specific interventions to strengthen health literacy in orthopaedic rehabilitation could be further developed and improved. In addition, the hitherto unknown educational competence of caregivers in the rehabilitation sector should be investigated to gain a more detailed insight into this core competence, to identify possible needs and to align training programmes accordingly. Routine assessment of clinical outcomes has been part of professional, interdisciplinary treatment of orthopaedic patients for years. We recommend routine health literacy assessments as an important part of treatment evaluation and as an evaluation of the effectiveness and comprehensibility of educational rehabilitation interventions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics committee approval and informed consent
Ethical approval for the study was obtained from the Regional Ethics Committee of the Medical University of Innsbruck (No. ECS-1057/2019). All patients who participated in the study gave their written informed consent.
Funding
The study was funded by the Tyrolean Science Fund (GZ: UNI-0404/2342). The funder was not involved in any part of the study or in the writing of the manuscript and had no part in the decision to submit the manuscript for publication.