
Abstract
Background:
Research has identified predictive factors for inpatient complications and short-term recovery following total knee arthroplasty (TKA) and total hip arthroplasty (THA). Predictors that may influence length of care in outpatient physical therapy (PT) have yet to be examined. Doing so may improve the quality and efficiency of PT care following TKA and THA.
Purpose:
The aim of this study was to determine factors associated with a higher utilization of outpatient PT visits for patients who have had primary THA or TKA.
Methods:
A retrospective cohort study was performed using a population of 5147 patients who underwent THA and TKA between January 2017 and October 2022. Demographic and clinical factors were analyzed to determine which factors influenced PT utilization.
Results:
Our multivariable linear regression model revealed that female sex, need for inpatient PT visits, and TKA as opposed to THA were significantly associated with an increase in outpatient PT visits. Older age, number of telerehabilitation visits, and history of depression were associated with fewer outpatient PT visits while accounting for all other variables.
Conclusions:
The results of this retrospective analysis may help to identify some potential factors including TKA vs THA, patient age, and a history of depression that can be evaluated prospectively in future studies to determine whether they predict subsequent outpatient PT utilization.
Keywords
Introduction
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) remain successful treatments for end-stage osteoarthritis (OA). Kremers et al [18] reported that 2.5 million and 4.7 million people underwent THA and TKA, respectively, between 1990 and 2010. Up to 700 000 TKAs may occur in the United States each year [23]. These numbers are expected to continue or increase as the population ages and younger populations seek out total joint arthroplasty (TJA) as a solution to pain and dysfunction, with projections of up to more than a 50% increase in the prevalence of these surgeries [18].
Often, patients who have undergone THA or TKA attend outpatient physical therapy (PT) for supervised guidance during recovery of movement and function. It has been reported that outpatient PT, following uniform procedures and care, shows only modest short-term benefit to those who underwent THA or TKA [2,8], with no difference in long-term outcomes when compared with those underwent THA or TKA but did not attend outpatient PT. In addition, Hamilton and colleagues reported data comparing TJA recipients identified as being at risk for a poor outcome [11]. One group received 18 outpatient PT visits and the other group received 1 at-home visit by a PT, in which they were instructed in self-directed care. After following the subjects for 52 weeks, the authors concluded that outpatient PT-led care was not superior to at-home self-directed care.
Despite this evidence suggesting that outpatient PT may have minimal benefits to those who have undergone TJA, a large percentage of postoperative patients receive PT services as part of their rehabilitation. However, the data on outpatient PT usage are small and heterogeneous. A systematic review reported that outpatient PT usage following THA or TKA ranged from 16.7% to 84.5% [15]. In addition, the authors stated that the definitions of PT and rehabilitation approaches varied greatly, as did the subjects included in each study and the length of each episode of care. This variability in PT practice and utilization necessitates further investigation to determine how to best serve individuals who have undergone TJA.
The differences in practice and utilization demonstrate a need to identify possible correlates or predictors for those who may benefit from outpatient PT or require a longer episode of care. Many studies have identified predictive factors for inpatient complications, short-term functional recovery, and risk of readmission [13,12,17,16,24]. Some of the common variables associated with short-term complications and recovery include age, sex, race, premorbid status, medical comorbidities, and socioeconomic status. It is unknown whether these factors predict outpatient PT use and long-term outcomes. Identifying predictors may assist health care providers in making clinical decisions surrounding immediate and long-term care both before and following a TJA. This information may help guide rehabilitation approaches and guidelines for more effective and efficient care. In addition, improved insurance coverage could be formulated based on predictive factors for patients recovering from a THA or TKA.
The purpose of this retrospective study was to examine the possible correlates of higher outpatient PT use following TKA or THA. Identifying both modifiable and non-modifiable preoperative factors associated with higher utilization can better inform postoperative rehabilitation considerations and approaches.
Methods
A retrospective cohort study was conducted of patients who underwent primary, unilateral TJA from a single orthopedic institution from January 2017 to October 2022. Individuals were excluded if they underwent revision surgery or bilateral TJA, were less than 18 years of age, or did not have outpatient PT at a location within our institution. The number of outpatient visits was calculated from the initial PT evaluation until the final visit documented in the electronic health record (EHR).
Demographic data including sex, body mass index (BMI), race, ethnicity, age, marital status, and history of chronic conditions including past medical history were collected and used to describe our sample and for analysis. Concomitant chronic medical conditions included diabetes mellitus (DM), cancer, and heart disease. Additional clinical data were also collected. The Risk-Assessment Prediction Tool (RAPT) was scored and used to predict patient discharge disposition. Patient Health Questionnaire 2 (PHQ-2), surgery year, the occurrence of surgical or hospital complication diagnoses, preoperative and postoperative patient reported outcome measures (PROMs) including PROMIS-10 Mental/Physical and lower extremity functional scale (LEFS), number of inpatient PT visits, inpatient and outpatient payor group, whether or not the patient chose to receive postoperative PT at a Hospital for Special Surgery (HSS) rehabilitation location, the number of outpatient PT visits, and whether or not the patient chose to receive telehealth in-home visits from our institution’s telemedicine platform (HSS@Home).
A total of 5147 patients, 2769 (54%) TKAs and 2378 (46%) THAs, were included for analysis between January 1, 2017 and October 27, 2022. Descriptive statistics for patient characteristics are presented in Supplemental Table 1 for TKAs and Supplemental Table 2 for THAs. Mean age of the study population was 65.6 years (range = 18-93 years). Mean age of TKA and THA patients was 66.8 and 64.1 years, respectively. Females made up 63% of the overall, TKA, and THA study populations. Mean BMI of the overall study population was 29.4 (30.7 TKA and 27.7 THA). Mean RAPT score was 9.4 overall with TKA patients averaging 9.3 and THA patients averaging 9.5 indicating low risk for a need for inpatient rehabilitation. Most patients were discharged to their home in the 5-year time period (93% overall; 91% TKA; 95% THA). The mean number of outpatient PT visits was 11.5 for the overall study population (13.4 TKA, 9.4 THA).
Statistical Analysis
Descriptive statistics of the study population were summarized using means and standard deviations for continuous variables and frequencies, as well as percentages for discrete variables. Independent samples t-tests and 1-way analysis of variance (ANOVA) were used to compare the association between the mean number of outpatient PT visits and the independent variables. Independent variables found to be statistically significantly related to outpatient PT visits were considered as candidate variables for analysis in a multivariable linear regression model. These candidate variables were then assessed for redundancy. Variables that were found to be highly correlated had the extraneous variable removed from the regression models to improve efficiency and provide more precise estimates of the parameter estimates for the outcome of outpatient visits. A linear mixed model was used to report the mean scores reported the change for Medicare patients in the 3 PROMs (PROMIS-10 Mental/Physical and LEFS) from preoperative to postoperative. All analyses were performed using SPSS version 26.0 (IBM Corp.).
Results
Comparative analysis of the study population can be found in Supplemental Table 3. Overall, TKA patients averaged a higher number of outpatient PT visits compared with THA patients (13.4 vs 9.4, P < .001). Significant differences in mean outpatient visits were found between several patient factors including sex, age group, BMI group, and certain comorbidities. Overall, women had a higher number of visits, on average, than men (11.9 vs 10.9, P < .001). In addition, outpatient PT use in number of visits was higher for women than men regardless of procedure: TKA (13.7 vs 12.8, P = .003) or THA (9.7 vs 8.8, P = .001). As age increased, overall outpatient PT use decreased (P = .012). This same pattern was observed in TKA patients, with outpatient visits decreasing by age. However, for THA patients, patients 80 years and older averaged a higher number of visits when compared with all other age groups (P = .036). In the overall population, patients who underwent computer-assisted surgery, were seen by an inpatient occupational therapist (OT), reported a history of depression, and were on Medicare had lower mean outpatient visits. In TKA patients, patients discharged to a rehabilitation or specialized facility, had a reported history of depression and diabetes, and were on Medicare also had a lower number of PT visits on average. For THA cases, patients who were not seen by an inpatient OT, were on Medicare, and had a history of cancer all had a lower mean number of outpatient visits.
Table 1 displays the coefficients (β), standard errors (SE), t values, and P values for each independent variable included in the model. The coefficients represent the change in the dependent variable associated with a 1-unit change in the corresponding independent variable, holding all other variables constant. Results from the multivariable regression model found several factors associated with the number of outpatient PT visits. For the overall study cohort, older age (P = .044), THA procedure (P < .001), and a self-reported history of depression (P < .001) were all significantly associated with a decreased number of outpatient PT visits. Females (P = .003) had a higher number of inpatient PT visits (P = .012) and females were associated with an increased number of visits after adjusting for all other variables in the model. In TKA cases, older age (β = −0.15, P = .004), higher BMI (β = −0.13, P = .022), and history of depression (β = −2.97, P = .003) were associated with decreased number of outpatient visits, whereas a higher number of inpatient PT visits were associated with an increased number of outpatient visits (β = 0.28, P = .009). In THA cases, females (β = 1.65, P = .006) and non-White patients (β = 1.62, P = .035) were significantly associated with increased outpatient PT visits. For THA cases, patients reporting a history of depression were also significantly associated with fewer visits after controlling for all other variables in the model (β = −1.69, P = .050). In all models, patients with Medicare coverage were not associated with outpatient PT utilization when compared with patients with commercial insurance.
Results from the multivariable regression model.
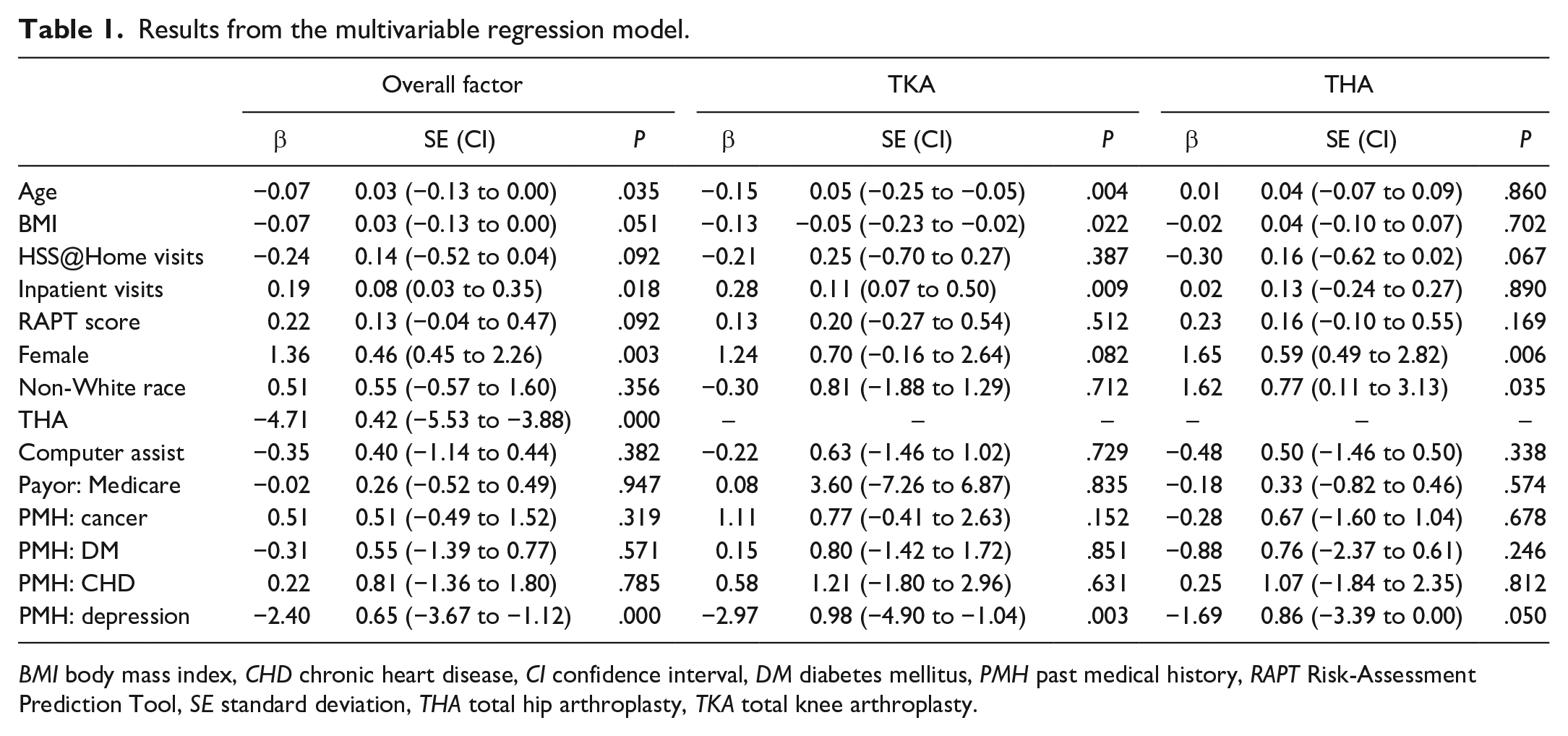
BMI body mass index, CHD chronic heart disease, CI confidence interval, DM diabetes mellitus, PMH past medical history, RAPT Risk-Assessment Prediction Tool, SE standard deviation, THA total hip arthroplasty, TKA total knee arthroplasty.
Mean improvement in PROMIS-10 Mental and Physical Health scores and LEFS for THA was found to be higher among THA patients compared with TKA patients. However, significant changes in all PROMs were observed for TKA and THA patients (Figs. 1 and 2). In the linear mixed models, the change in the outcome scores was not affected by the number of outpatient PT visits. Parameter estimates are presented as unadjusted results.
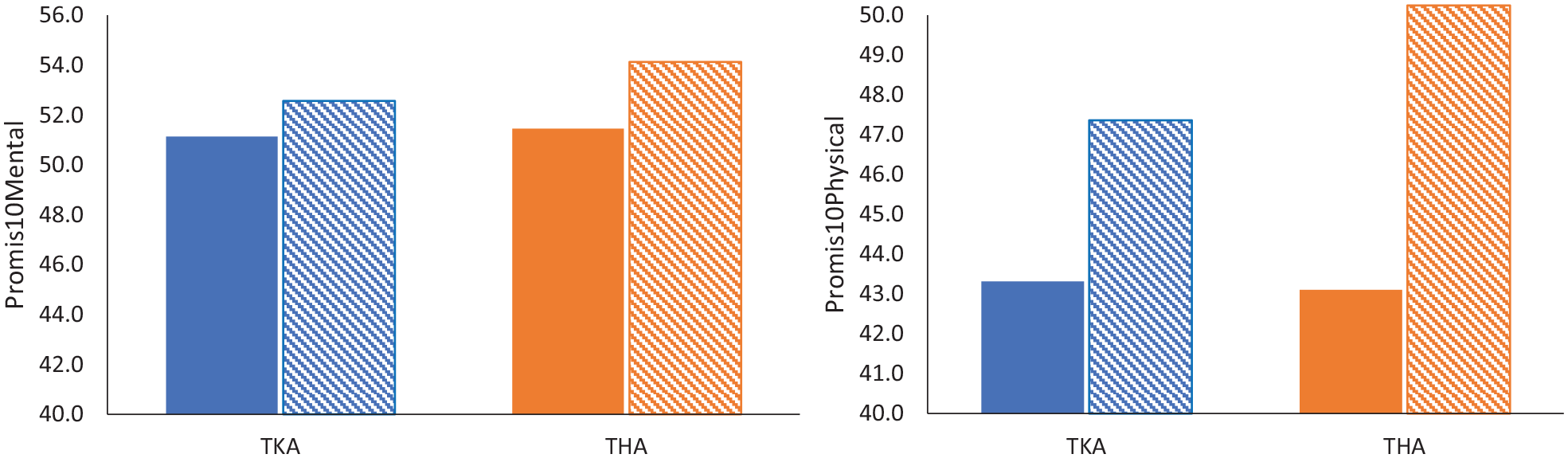
Preoperative and postoperative promis10 mental and physical health scores for TKA and THA. THA total hip arthroplasty, TKA total knee arthroplasty.
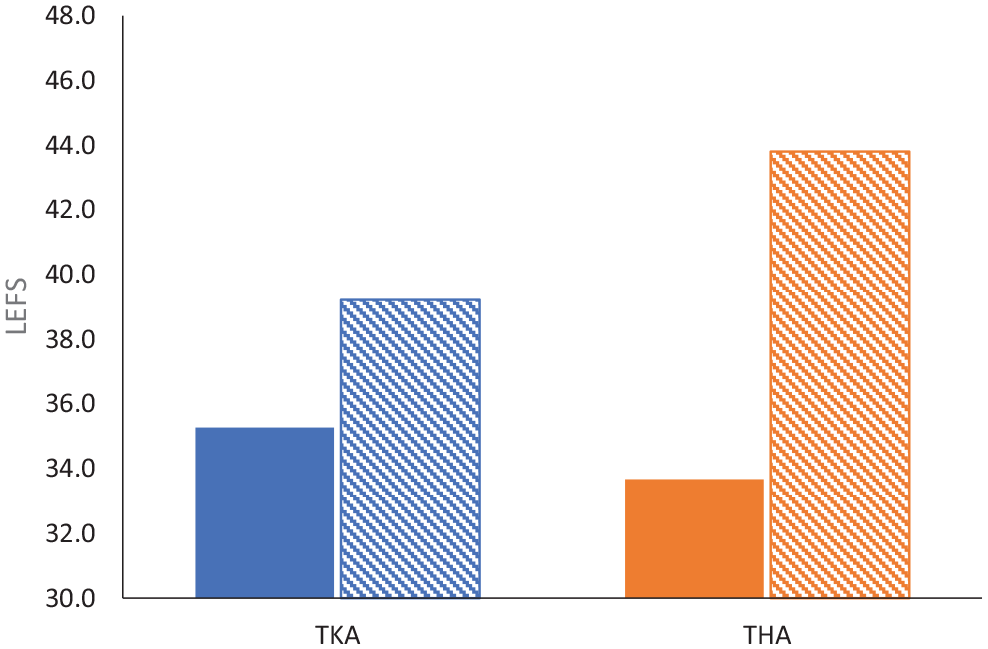
Preoperative and postoperative lower extremity functional scale (LEFS) scores for TKA and THA. THA total hip arthroplasty, TKA total knee arthroplasty.
Discussion
The findings of this 5-year retrospective analysis identified several factors that were associated with higher or lower outpatient PT usage in patients who had undergone TKA or THA. The THA or TKA patients in this cohort used an average of 11.5 ± 7.2 outpatient PT visits. These findings are consistent with recent studies that have analyzed PT utilization following TJA, which has been reported to be an average of 12 outpatient visits [4,5,14,19,20,21]. Among the factors analyzed, being female, being non-White, having had a higher number of inpatient PT visits, and having undergone TKA were associated with higher PT utilization, accounting for up to 4 additional outpatient PT visits. These findings are consistent with what has been found to be associated with inpatient complications, short-term functional recovery, and a risk of readmission [13,12,17,16,24]. Several factors were similarly identified as being associated with a lower number of outpatient PT visits. Among these factors, individuals who underwent TKA and THA with a history of depression used an average of almost 3 and 2 fewer visits, respectively.
Our study has potential limitations. Although sociodemographic factors such as age, race, and sex have been found to be associated with poorer outcomes and health care disparities [17,16,26,25,22], a clinically meaningful relationship between age and race and outpatient PT use was not found in this study. Future analyses should factor socioeconomic variables such as income and employment status as these may have implications on access to health care services, which, in turn, may impact the outcomes of outpatient PT and overall health care utilization. Several factors can account for these findings. One main limitation of this study is the lack of generalizability of the results due to sampling. Most individuals included in this analysis were White (78%), female (63%), and insured under Medicare or commercial insurance (95%). Access to care and other social determinants of health are associated with health disparities [1,3,9]. The lack of representation from varying socioeconomic and racial demographics in this study’s data prevents any conclusions on outpatient PT utilization in those from uninsured or otherwise underserved communities. Significant improvements in the LEFS and PROMIS 10 Mental and Physical Health were observed in both THA and TKA groups between the preoperative and postoperative periods. Due to inconsistencies in collection and completion of PROMs throughout the episode of care, conclusions could not be drawn on long-term outcomes and total PT utilization at the end of care. A future analysis investigating associations between PROMs and outpatient PT utilization could identify whether a relationship exists between the number of PT visits and outcomes. These results could be useful in informing guideline development and implementing policies related to third-party payors.
Contrary to current literature [6,7], medical comorbidities such as cardiovascular disease, cancer, and other chronic diseases were not found to be associated with a clinically significant difference in utilization. These findings may be explained by the lack of generalizability of the characteristics of the participants included in this analysis. Premorbid functional status, medical comorbidities, age, sex, and TKA have previously been shown to be associated with longer inpatient recovery. However, very little is known of the impact that these factors might have on long-term outcomes or health care utilization [7,18,19]. This study’s results may help to identify potential preoperative targets to improve the efficiency and delivery of outpatient PT services for individuals undergoing THA or TKA.
Variability in practice, PT utilization, and heterogeneity of outcomes in people who have undergone THA or TKA have been recognized and have resulted in efforts to improve the standards of care [10]. Our facility implements clinical rehabilitation guidelines with the aim of reducing variability in practice, providing criteria-based phase progressions, and criteria for discharge to avoid over utilization of outpatient visits. The results of this analysis highlight some factors which may identify those individuals who may require more outpatient PT utilization following TJA. What impact the differences in PT use have on clinical outcomes is unknown and should be further explored. The results of this analysis highlight areas of future research that can be conducted to evaluate the effectiveness of preoperative intervention on outpatient PT utilization, long-term outcomes, and potentially influence policy that informs third-party payor decisions regarding postoperative PT care.
In conclusion, the results of this retrospective analysis suggest the factors that should be evaluated prospectively in future studies to determine whether they impact subsequent outpatient PT use following TKA or THA.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231210556 – Supplemental material for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-1-hss-10.1177_15563316231210556 for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study by Curtis Wu, Ashleigh McAdam, Scott Siverling, Joseph Nguyen and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231210556 – Supplemental material for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-2-hss-10.1177_15563316231210556 for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study by Curtis Wu, Ashleigh McAdam, Scott Siverling, Joseph Nguyen and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231210556 – Supplemental material for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-3-hss-10.1177_15563316231210556 for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study by Curtis Wu, Ashleigh McAdam, Scott Siverling, Joseph Nguyen and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231210556 – Supplemental material for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-4-hss-10.1177_15563316231210556 for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study by Curtis Wu, Ashleigh McAdam, Scott Siverling, Joseph Nguyen and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231210556 – Supplemental material for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-5-hss-10.1177_15563316231210556 for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study by Curtis Wu, Ashleigh McAdam, Scott Siverling, Joseph Nguyen and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231210556 – Supplemental material for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-docx-6-hss-10.1177_15563316231210556 for Factors Associated With Higher Utilization of Outpatient Physical Therapy for Patients Who Have Undergone Primary Total Joint Arthroplasty: A Retrospective Cohort Study by Curtis Wu, Ashleigh McAdam, Scott Siverling, Joseph Nguyen and Danielle Edwards in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level IV, retrospective cohort study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.