
Abstract
Background/purpose
In the current study, our aim was to compare the efficacy and biocompatibility of teicoplanin-loaded and vancomycin-and-gentamicin-loaded articulating spacers used in two-stage revision arthroplasty for eradication of periprosthetic knee joint infection.
Methods
In the current retrospective cohort study, there were 24 patients who were given 2 g or less antibiotics per 40 g of cement in the low-dose teicoplanin group, and 20 patients who were given a total of 3.6 g or more antibiotics per 40 g of cement in the high-dose vancomycin and gentamicin group. Two groups were compared statistically.
Results
There was no statistically significant difference in the treatment failure between the two groups (p = 0.488). No statistically significant differences were found in spacer fracture rates between the two groups (p = 0.802).
Conclusion
The current study has demonstrated that low-dose teicoplanin protocol is as effective and safe as high-dose vancomycin and gentamycin protocol.
Introduction
Deep infection remains one of the most challenging complications following total joint replacement. 1 Although multiple strategies have been used to treat knee periprosthetic joint infection (PJI), the two-stage exchange arthroplasty remains the current gold standard of care. 2 Using a temporary antibiotic-loaded cement spacer (ALCS) in the first stage allows early knee joint activity, a shorter hospital stay, and potentially a decreased rate of reinfection. 3
In clinical applications, the most important requirements of ALCS are its mechanical properties, releasability, and the efficacy of loaded antibiotics. 4 Although there is no current consensus on the ideal antibiotic to be used within a spacer, because of their broad spectrum, efficacy, mechanical properties, and their systemic safety, aminoglycosides (e.g. gentamicin) and glycopeptides (e.g. vancomycin, teicoplanin) are the antibiotic formulations most commonly loaded into acrylic bone cement. 5 Unfortunately, the ideal amount of antibiotics to be used for spacer impregnation also has not been defined. 6
Vancomycin-loaded bone cement has become one of the most commonly used ALCSs in both prophylactic and therapeutic treatment of PJIs, especially for gram-positive pathogen infections. 7 Gentamicin is a widely used antibiotic in combination with vancomycin because of its gram-negative efficiency. Gentamicin also has some advantages like concentration-dependent bactericidal activity, thermal stability, and high water solubility. 8 Thus, bone cement spacers including gentamicin and vancomycin combination are also preferred in the treatment of PJI.
Teicoplanin is another commonly used antibiotic for preparing ALCS. It is an effective antibiotic against gram-positive pathogens 9 and it does not change the biocompatibility of bone cement. 10 Several recent studies have indicated that ALCSs that contain teicoplanin are more effective than ALCSs that contain vancomycin.9–11
Low-dose teicoplanin (LDT) loaded or high-dose vancomycin and gentamicin combination (HDVG) loaded ALCSs are the protocols used in our clinic. To our knowledge, so far no study has evaluated the efficiency of LDT-loaded ALCS against HDVG-loaded ALCSs. In our study, our aim was to compare the in vivo efficacy of these spacers in terms of biocompatibility and antimicrobial efficacy of bone cement.
Materials and methods
This study was conducted in accordance with the Helsinki Declaration Principles after the approval of the IRB (Institutional Review Board). A retrospective search was performed using the online database of our hospital for the records between 2005 and 2018. The Workgroup of the Musculoskeletal Infection Society infection criteria was used to diagnose PJI. 12 There were 61 patients who were treated with two-stage revision surgery with the diagnosis of PJI of the knee. Inclusion criteria were the PJIs of the knee treated with either LDT or HDVG-loaded ALCSs with an articulation. Exclusion criteria included ALCSs with any other type of antibiotic combinations with different dose regimens, patients with a follow-up period of less than two years after implantation of the last articulating ALCS, and patients without an antibiogram. Ultimately, 44 patients were included in the study.
The first stage of the two-stage arthroplasty protocol included surgical debridement and removal of all implants and cement. Synovial fluid samples and periprosthetic soft tissue with inflammatory changes were collected for microbiological and histopathological examination. Antibiotic-loaded cement was prepared by manual mixing based on the preference of surgeon and placed in the articular space. Simplex (Stryker, Kalamazoo, MI, USA) was the preferred brand. After obtaining the culture results, intravenous antibiotic therapy according to culture antibiogram was rearranged and continued for six weeks. Some patients needed more than one debridement with revision of the cement spacer before the second stage operation due to persistent infection findings. The second stage of revision was performed in all patients after achieving normal ESR (erythrocyte sedimentation rate) and CRP (C-reactive protein) values.
In the current study, patients were divided into two groups as those who were applied LDT-loaded ALCSs and those who were applied HDVG-loaded ALCSs. There is no consensus on how much antibiotic should be in the low-dose or high-dose antibiotic-loaded spacer in the literature. In Jiranek et al.'s study, a low-dose ALCS, defined as 1 g or less of powdered antibiotic per 40 g of bone cement. 13 Penner et al. mentioned that higher antibiotic doses; at least 3.6 g of antibiotic per 40 g of acrylic cement. 14 In another study, 1 or 2 grams of antibiotic powder per batch of bone cement (40 g of polymer and 20 mL of monomer liquid) were considered a low dose with mechanical properties that are still intact. 4 In the current study, 24 patients who were given 2 g or less antibiotics per 40 g of cement were included in the first group (LDT group), and 20 patients who were given a total of 3.6 g or more antibiotics per 40 g of cement were included in the second group (HDVG group).
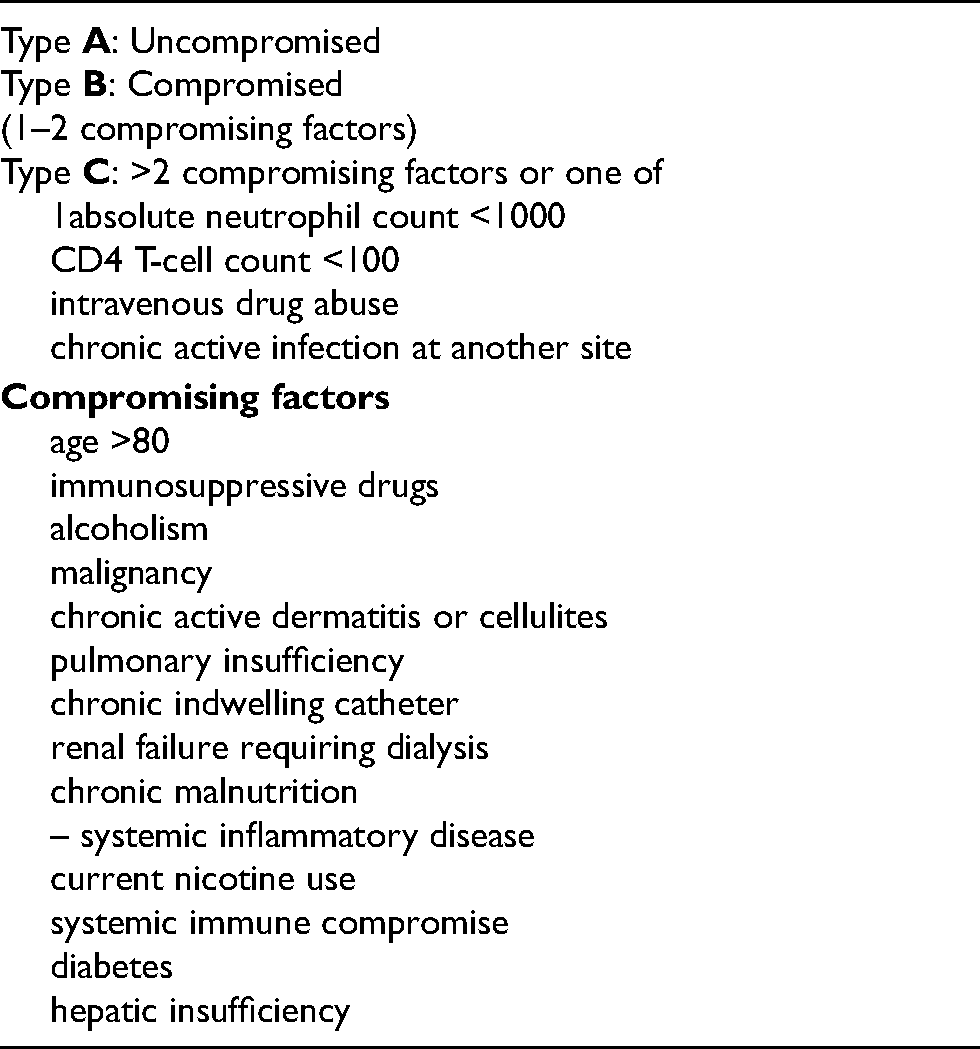
The total follow-up periods of the patients and the time from the first spacer application to the final treatment, the number of spacer replacement operations for each patient, the number of spacer fracture for each patient, the presence of sinus, and the antibiogram results of these patients were analyzed retrospectively. The systemic host grade of the McPherson classification was used for the evaluation of the patients’ immunologic status (Table 1). 15 All patients were Type 4 (late chronic infection - after 4 weeks) according to Tsukayama et al.'s 16 classification for deep PJIs.
Mcpherson's systemic host grading system [11].
After the second stage operation, the patients were followed up on the 2nd, 4th, 12th and 24th week postoperatively and then annually for clinical evaluation and serological tests including ESR and CRP. A successful treatment of infection was considered in the setting of normalized CRP and ESR findings and the absence of clinical signs of inflammation.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, NY, USA) software. Descriptive statistics were calculated as appropriate for the variables. A chi-squared test and Fisher's exact test was used as appropriate for the analysis of the categorical data and observations with a p value of 0.05 or less were considered significant.
Results
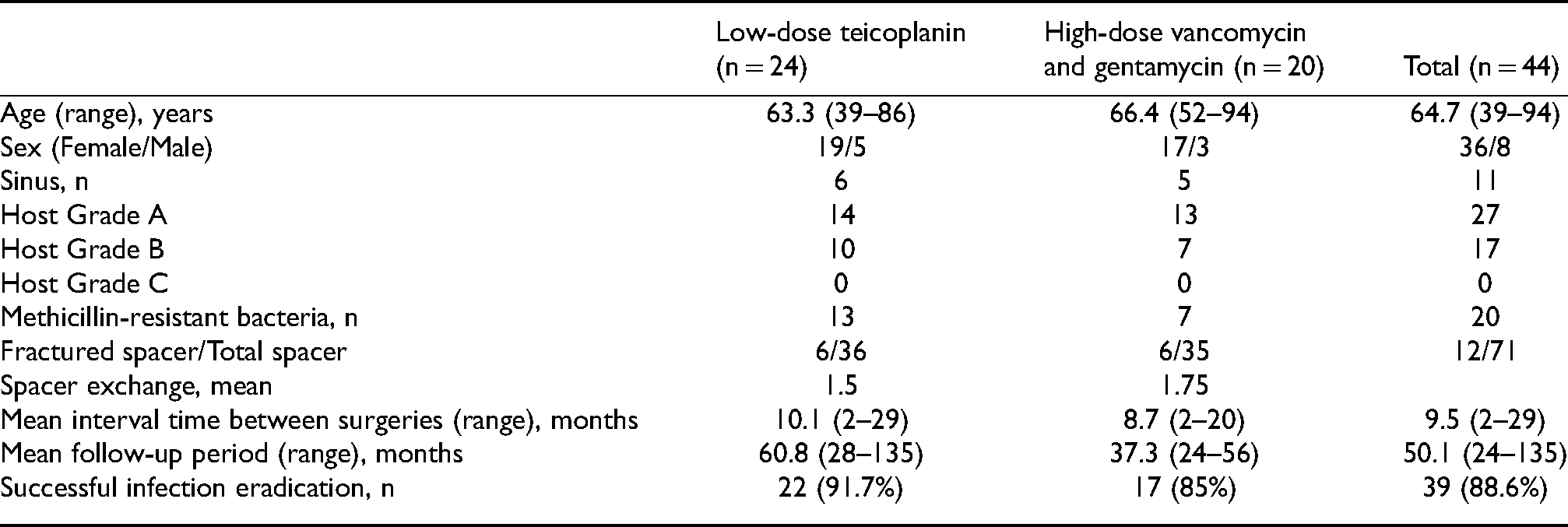
The two groups’ features; age, sex, sinus, host grade, 15 number of antibiotic-resistant microorganisms, number of spacer fractures, number of spacer exchanges, mean interval time, and mean follow-up time were compared in Table 2. The overall successful infection eradication was 88.6% (39 of 44 patients). One of the two treatment failures in the LDT group and one of the three failures in the HDVG group were treated with arthrodesis. One of the two patients in the LDT group and two of the three patients in the HDVG group were managed with chronic antibiotic suppression after the second stage revision operation.
Features of LDT and HDVG groups.
In the LDT group, the spacer contained an average of 1.7 g (range: 1.5 to 2 g) teicoplanin per 40 g bone cement, while in the HDVG group, it contained an average of 3.9 g (range: 3.6 to 5.5 g) vancomycin and 1.1 g (range: 1 to 2 g) gentamicin per 40 g bone cement. Systemic toxicity or hypersensitivity due to antibiotics was not observed in any of the patients included in the study.
Staphylococcus epidermidis was the most common isolated bacterium in both groups. In the LDT and HDVG group there were two (8.3%) and 10 (50%) culture-negative cases, respectively. The distribution of microbiological species between the LDT and HDVG protocols can be seen in Table 3.
Microbiological profiles of the patients.
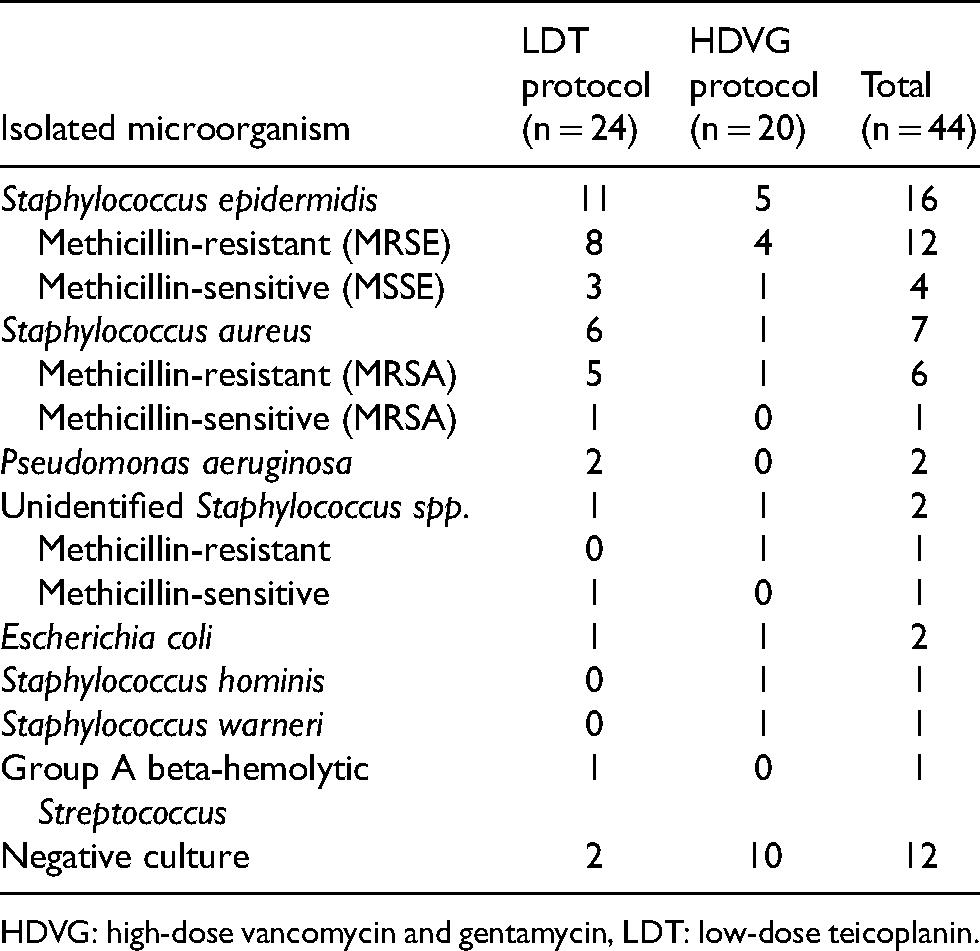
HDVG: high-dose vancomycin and gentamycin, LDT: low-dose teicoplanin.
Treatment failure was seen in two patients (8.3%) in the LDT group and in three patients (15%) in the HDVG group. According to Fisher's exact test, no statistically significant differences in the failure rates were detected between the two groups (p = 0.488).
There were 10 patients in the LDT group and seven patients in the HDVG group who were McPherson systemic host grade B. Treatment failure was seen in one patient (10%) in the LDT group and two patients (28.6%) in the HDVG group. According to Fisher's exact test, no statistically significant differences in the treatment failure rates were detected in terms of host grade B between the two groups (p = 0.323).
The LDT group had 13 methicillin-resistant-bacteria-isolated patients and the HDVG group had seven. Treatment failure was observed in two patients (15.4%) in the LDT and one patient (14.3%) in the HDVG group. There was no statistically significant difference in the treatment failure between the two treatment protocols in patients infected by resistant bacteria (Fisher's exact test, p = 0.948).
There were six patients with sinus in the LDT group and five in the HDVG group. No treatment failures were observed in the LDT group (0%), whereas two patients (40%) in the HDVG group had it. There was no statistically significant difference in terms of treatment failure between the two treatment protocols in patients with sinus (Fisher's exact test, p = 0.087).
In total, 36 antibiotic spacers were applied to 24 patients in the LDT group and 35 spacers to 20 patients in the HDVG group. There were six spacer fractures in in the LDT group (16.7%) and six in the HDVG group (17.1%). According to Fisher's exact test, no statistically significant differences were found in spacer fracture rates between the two groups (p = 0.802).
Discussion
The two-stage revision with the implantation of an articulating antibiotic spacer has been the gold standard for the treatment of PJI. 2 The main advantage of this technique is that local antibiotics reach concentrations that systemic treatment cannot reach. 17 Many different antibiotic loading ratios from low to high concentrations have been previously studied. 18 For example, Hart and Jones used 1 gram of vancomycin per cement pack, 19 Stevens et al. incorporated 3.6 g tobramycin and 3 g vancomycin, 20 and Haddad et al. used 2.4 to 3.6 g tobramycin and 1 to 1.5 g vancomycin. 21 Unfortunately, there is no current consensus on the ideal antibiotic loading to be used within a spacer. While the addition of high antibiotic concentrations is generally thought to correlate with high antibiotic elution, previous studies have shown that this is not always true. 22 However, the most appropriate antibiotics to be added to a cement spacer remains a matter of debate. 23 In the current study, the spacer contained an average of 1.7 g of teicoplanin per 40 g bone cement in the LDT group, while in the HDVG group, it contained an average of 3.9 g vancomycin and 1.1 g gentamicin per 40 g bone cement.
The use of a glycopeptide and aminoglycoside is particularly attractive for bone cement because of the potential antibiotic synergism against resistant gram-positive bacteria and its ability to disrupt the bacterial growth on the cement's surface. 24 In our clinic, two separate protocols containing glycopeptides, LDT- and HDVG-loaded ALCSs, are often preferred. Although the combination of vancomycin and gentamicin-loaded ALCS is a widely used treatment for PJI of the knee, there is an increasing number of studies in the literature showing the high efficacy of teicoplanin-loaded ALCSs.9,11,25 There is no previously reported comparative study examining clinical outcomes using high-dose vancomycin and gentamicin combination (HDVG) loaded and low-dose teicoplanin (LDT) loaded cement spacers.
In the current study, the infection eradication rate of LDT and HDVG groups were 91.7% and 85% respectively, with an overall infection eradication rate of 88.6%. All infection eradication rates were comparable to the rates reported in other studies. Most previous studies in the literature reported good outcomes, with success rates ranging from 88.3% to 100.0%.19,26,27 Treatment failure was observed in two of the 24 patients (8.3%) in the LDT group and in three of the 20 patients (15%) in the HDVG group. According to our results and those from the literature, both treatment protocols have been found successful. Although the LDT protocol seems more successful in terms of infection eradication, it was not statistically superior to the HDVG protocol (p = 0.488).
In the current study, there were no significant differences in the rates of reinfection between the LDT and HDVG groups in terms of host grade (p = 0.323). To our knowledge, the McPherson systemic host grade classification system was previously used in two studies for comparing the ALCS protocols.28,29 However, in both studies, different protocols from the current study were compared.
Bejon et al. have found teicoplanin-impregnated cement effective for methicillin-resistant strains with high rates of infection eradication (91.6%). 25 Chang et al. have found a better antibacterial effect and longer inhibitory periods against MSSA, MRSA, and VISA with teicoplanin-loaded cements than cements loaded with the same dose of vancomycin in their in vitro study. 9 In the current study, treatment failure was seen in two of the 13 methicillin-resistant-bacteria-isolated patients (15.4%) in the LDT group and in one of the seven patients (14.3%) in the HDVG group. Considering the results of the study, it cannot be said that one of the two protocols is statistically superior in terms of effectiveness on methicillin-resistant bacteria (p = 0.948). It should be mentioned that the treatment of LDT group seems to be more difficult than HDVG group because there are 13 drug resistance bacteria isolated patients in 24 patients of LDT group (54%), and 6 patients in 20 patients of HDVG group (30%).
The presence of sinus is considered a factor that makes treatment difficult in PJI of the knee. Infection treatment was unsuccessful in two of the 11 patients (18.2%) with sinus. Although two patients with treatment failure were from the HDVG group, there was no statistically significant difference in terms of treatment success between the two protocols (p = 0.087). However, we should state that the number of patients is not enough to make a sufficient statistical evaluation.
Spacer fracture is one of the important parameters used when comparing ALCSs. High doses of antibiotics in bone cement have been shown to significantly reduce the mechanical strength of the cement, 13 because an increase in porosity causes a net loss in load-carrying capacity per cross sectional area and forms stress concentration sites, typically reducing the mechanical properties of the cement. 26 Chang et al. found no significant differences in the ultimate compressive strength between the cement samples loaded with different types of low-dose antibiotics (40 g PMMA loaded with 1 g antibiotics). 11 Although spacer fractures are expected to be more in the HDVG group, no statistically significant difference was found between the two protocols in terms of spacer fracture in our study (p = 0.802). When the radiographs of the spacers were examined retrospectively, we saw that the fractures were usually at the most loaded part of the femoral component. In many patients with spacer fractures, the inferior part of the spacers, which was exposed to the greater load, was thinner than the others (Figures 1 and 2). The weakness of this area can be considered as an independent factor that may explain the lack of statistical difference in terms of spacer fractures between the two groups.

A spacer fracture from LDT group.

A spacer fracture from HDVG group.
The high dose of antibiotics in the HDVG protocol, the synergistic effect of vancomycin and gentamicin, and the gram-negative activity of gentamicin in addition to the gram-positive activity of vancomycin makes us consider that HDVG protocol should be more successful than the LDT protocol. Although there has been an increasing bacterial resistance in PJIs of the hip and knee against gentamicin, 27 it has been shown that the ALCSs containing gentamicin has much longer release durations (ten days) than vancomycin and teicoplanin (two days each). 11 This feature of gentamicin also provides an important advantage to the HDVG protocol. Although the results seem better in the LDT group, no statistically significant difference was found between the two groups in terms of treatment success in our study. Four gram-negative bacteria were isolated in the LDT group and one in the HDVG group. Treatment success was also achieved in the patients with the LDT protocol although it contains teicoplanin, which has no gram-negative antibacterial activity. Thorough debridement before spacer implantation in PJIs of the knee and administration of intravenous antibiotics effective against microorganisms isolated in the intraoperative cultures are important factors that increase the success of the treatment. In fact, sufficient debridement and administration of appropriate antibiotic treatment in the postoperative period may have contributed to the absence of a difference between both protocols.
There were some limitations to our study. The first one was the inherent limitations of a retrospective design. The second one was the use of varying antibiotic regimes and doses used in the postoperative period, and the differences in the interval between the first and second surgeries among the groups. Non-selective use of the spacer, regardless of the susceptibility profile of the infecting bacteria and insufficient sample size were other limitations. Finally, the decreased statistical power because of low sample size may be considered as a limiting factor.
The current study has demonstrated that low-dose teicoplanin protocol is as effective and safe as high-dose vancomycin and gentamycin protocol used for two-stage revision with the implantation of an articulating antibiotic spacer for PJI. In conclusion, using low-dose teicoplanin-impregnated cement can be an alternative for patients suffering from PJI of the knee instead of vancomycin and gentamicin combination-impregnated cement.
Footnotes
Conflict of Interest (CoI) statements
Osman Çimen, Ali Öner, Alper Köksal, Ferdi Dırvar, Muhammed Mert, Mümine Nursu Şahin, Deniz Kargın declares that they have no conflict of interest
We declare that the material contained in the manuscript hasta not been previously published and is not being concurrently submitted elsewhere.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.