
Abstract
Background
Osteoporotic vertebral compression fractures constitute a major concern in elderly population who may not tolerate conservative treatment. Although percutaneous vertebroplasty is an alternative minimally invasive procedure that is commonly used nowadays, there is still debate about its efficacy. The study aim is to provide short term experience about efficacy of vertebroplasty for osteoporotic vertebral fractures.
Methods
Thirty five patients were treated by percutaneous vertebroplasty (the intervention group). The visual analog scale before the intervention (pre VAS), one week after the intervention (post VAS 1), at three months (post VAS 2) after the intervention were compared at each time point with the control group (35 patients). The oswestry disability index before (pre ODI) and three months after the procedure (post ODI) were assessed. The control group received the optimal medical treatment and a regular physiotherapy program for three months.
Results
Both conservative and vertebroplasty group showed significant improvement in the VAS/ODI with time. With vertebroplasty, the improvement is faster and statistically significant compared with conservative group. There were statistically significant differences between both groups concerning post VAS 1, post VAS 2 and post ODI as the P values were 0.00 in all relationships.
Conclusion
Patients with osteoporotic compression fractures who were treated with percutaneous vertebroplasty experienced considerable clinical improvement in comparison with those who received the conservative management.
Introduction
Osteoporotic vertebral compression fractures (OVCFs) are widespread in the geriatric population. 1 It is considered one of the important factors that affect the quality of life in the elderly with morbidity and mortality higher than hip fractures.2,3 The annual incidence of new vertebral fractures accounts for about 1.4 million fractures all over the world. 4 An estimated one quarter of the population above 50 years old will suffer a vertebral fracture throughout their lifetime. 5
In the past, conservative therapy was traditionally the standard treatment for OVCFs. It includes immobilization, pain killers, bracing and physical therapy. 6 Although natural healing occurs in most fractures, some patients will have persistent pain and disability and will require prolonged medical care. 7 Moreover, elderly population may not tolerate the conservative treatment. Considerable complications take place due to the long period of being bedridden such as bedsores, pneumonia, deep venous thrombosis (DVT) and urinary tract infection (UTI). 8
Nowadays, percutaneous vertebroplasty (PVP) is an alternative newer option. It is minimally invasive procedure that has been used worldwide for the treatment of symptomatic OVCFs. The procedure involves injection of poly-methyl-methacrylate (PMMA) bone cement into the vertebral body aiming at stabilizing the fracture and immediate improvement of pain. 9 It is an image guided technique that is usually done using fluoroscopy. As the majority of these patients are frail elderly postmenopausal women who may not tolerate general anesthesia and prone position, PVP can also be performed using local anesthesia. 10
However, injection of bone cement can also bring about complications such as cement leakage into the disc space, spinal canal, neural foramen, veins, lungs or soft tissues. 11 In the literature, PVP is occasionally associated with increased risk of adjacent new vertebral fractures in the follow up period. 12 It is still debatable if PVP has short and long term effects superior to conservative therapy.
The aim of this study is to present our short term experience employing PVP for the management of painful OVCFs and comparing it with the traditional conservative therapy. Efficacy, safety and technique would be reported
Material & methods
This was a prospective randomized controlled clinical trial of patients with painful OVCFs treated with PVP. The study included patients with one or two vertebral fractures due to primary or secondary osteoporosis. The level of the vertebral fracture was either thoracic or lumbar. The control group received a regular physical therapy program in addition to medical treatment for three months. The conservative therapy involved pain medication, osteoporosis medication, topical analgesics and bracing. The pain medications involved oral Diclofenac (75 mg BID) and Acetaminophen (1000 mg BID). The osteoporosis medication included bisphosphonates (Risedronate 35 mg weekly), Calcium (1000–1500 mg/d taken with meals) and vitamin D supplement (400–800 IU/d). After a short period of bed rest (seven days), the patients started a rehabilitation program. The physiotherapy program was done by well trained specialists in our hospital. The program included strengthening exercise, stabilization exercise, balance training, stretching, relaxation techniques and taping. Bracing was used to enhance pain control as patient is mobilized. Patients were diagnosed with painful OVCFs by clinical means, computed tomography (CT) and magnetic resonance imaging (MRI). The location of the pain should be consistent with anatomical site of the fracture in the MRI. The pain localization was limited to no more than one vertebral level. A metallic marker was helpful in some patients for better localization. The patient pain was not radicular. Bone marrow edema on MRI was present in all case and is considered an indication for PVP.
Primary hypothesis
Percutaneous injection of medical bone cement into a painful osteoporotic vertebral compression fracture will improve patient pain and functional disability.
Study population
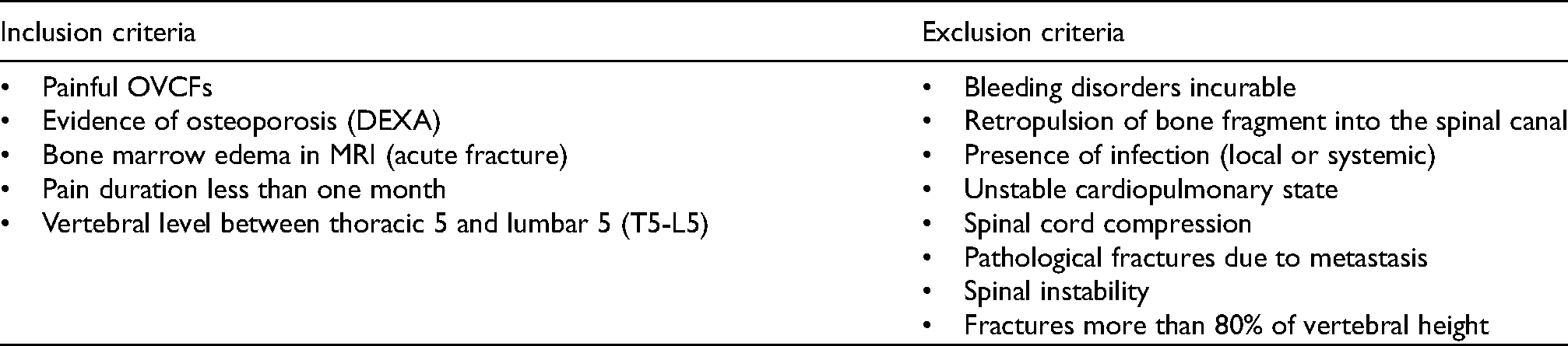
Two hundred out of 7220 patients with acute back pain were assessed for eligibility at our spine outpatient clinic between April 2017 and October 2019 based on the general inclusion and exclusion criteria set (Table 1). Seventy patients met the inclusion criteria and were included into the study. The study aim and design was approved by the medical and ethical committee of the neurosurgery department, faculty of medicine at our institute. Thirty five patients were treated with PVP. The other half was the control group. Randomization was done using random number table preferred by the statistician to determine to which group the patient was assigned. There is no source of any potential selection bias.
General inclusion and exclusion criteria set.
General demographic information, including age and sex, in addition to body weight, were obtained from patients questionnaires. Baseline outcome scores were obtained from each patient using visual analog scale (VAS) and Oswestry disability index (ODI). Two days before the procedure, the patient provided informed consent. A baseline clinical assessment was done. Blood samples were withdrawn to assess complete blood count, International Normalized Ratio (INR), liver and kidney functions, blood glucose to ensure that all values were within normal. Using dual energy X ray absorbiometry (DEXA), all patients had evidence of osteoporosis (values more than −2.5).
The procedure
PVP was done under general anesthesia using the transpedicular approach. The intervention was done with the patient in the prone position on a radiolucent operating table. The patient's back was prepared in a sterile technique and the target entry point was identified using C-arm fluoroscopic device. A 13-gauge trocar–cannula system was used. Bipedicular technique was used in all cases. The skin entry point was slightly lateral to the lateral pedicle edge (3:00 position on the left pedicle, 9:00 position on the right). These marks were identified after squaring the vertebra using fluoroscopy. The Jamshidi needle was advanced approximately 2/3 the way through the vertebral body (Figure 1). A mean volume of 3 ml of PMMA (Mendec spine kit with high barium content for opacification) was injected in each fractured vertebral body. Injection was stopped if the cement reached the posterior one quarter of the vertebral body or if any leak occurs. The whole procedure was done using fluoroscopy (image guided technique) (Figure 2). Analgesia was provided for all patients after the procedure according to the patient needs (Acetaminophen 1000 mg BID was used routinely for one week). Instructions were given to the patients to remain recumbent for two hours after the procedure. Clinical monitoring of neurological functions or any side effects was done. All patients were discharged at the same day of the procedure.
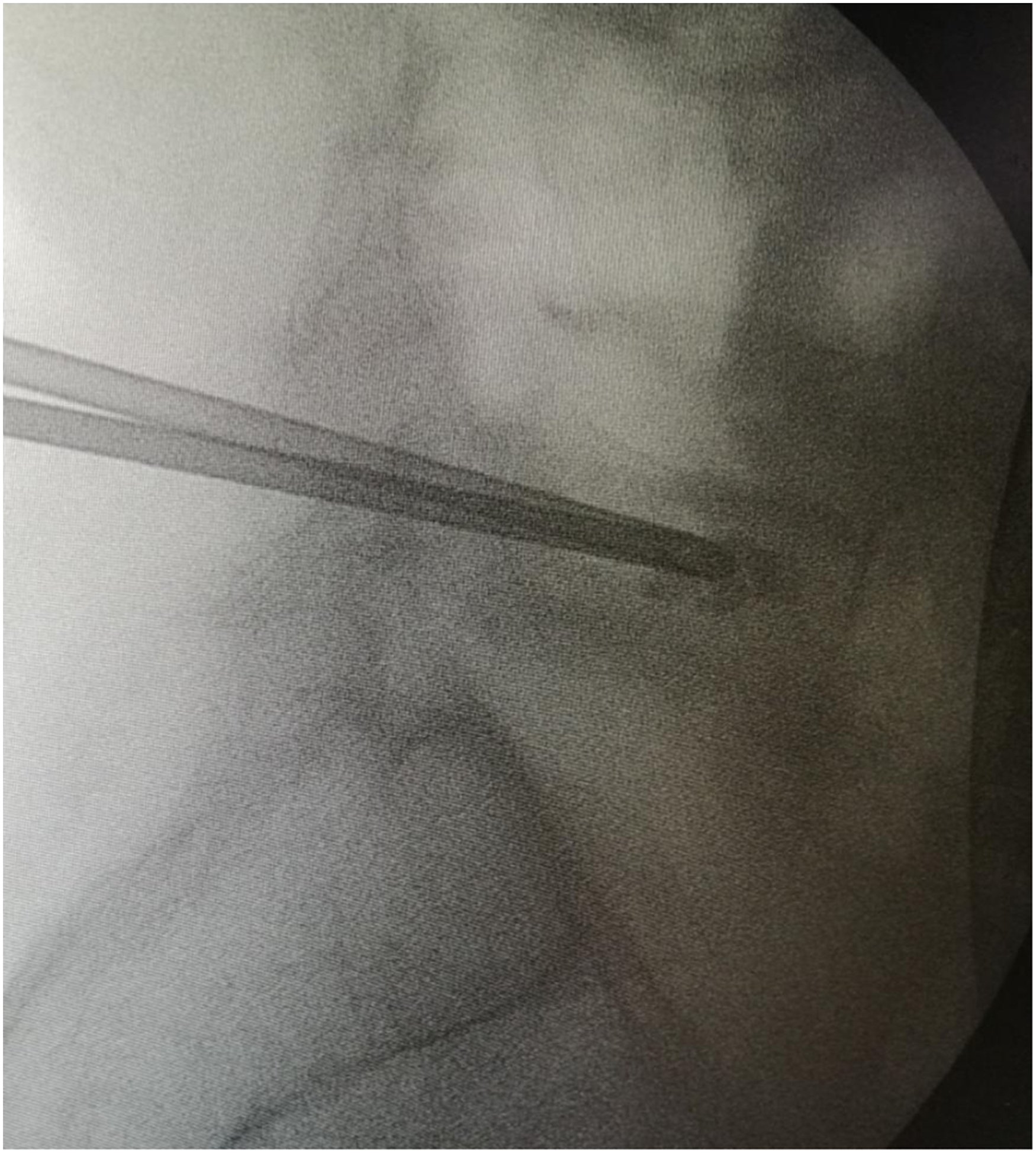
Lateral fluoroscopic view of the Jamshidi needles in L5 fracture.

Final fluoroscopic view of D12 and L1 vertebral fractures augmented with bone cement.
Follow-up questionnaires were then administered postoperatively.
Statistical analysis
Data were statistically described in terms of mean ± standard deviation (± SD), or frequencies (number of cases) and percentages when appropriate. Numerical data were tested for the normal assumption using Kolmogorov Smirnov test Comparison of numerical variables between the study groups was done using Student t test for independent samples. Within group comparison of numerical variables was done using paired t test For comparing categorical data, Chi-square (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5. Two sided P values less than 0.05 was considered statistically significant. All statistical calculations were done using computer program IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 22 for Microsoft Windows.
Outcome measures
Pain relief and improvement of functional disability were the primary outcomes. Pain relief was assessed by VAS. The results were analyzed at one week (post VAS 1) and three months (post VAS 2) of follow up. Functional disability was assessed using ODI and the results were analyzed 3 months after the procedure. The rate of new vertebral fractures after the procedure was considered the secondary outcome. Patients were considered a categorical success if they achieved improvement in the VAS and the ODI.
Results
Comparison between the PVP and the control groups concerning VAS and ODI before and after the procedure (Table 2).
Comparison between the PVP and the control groups concerning VAS and ODI before and after the procedure.
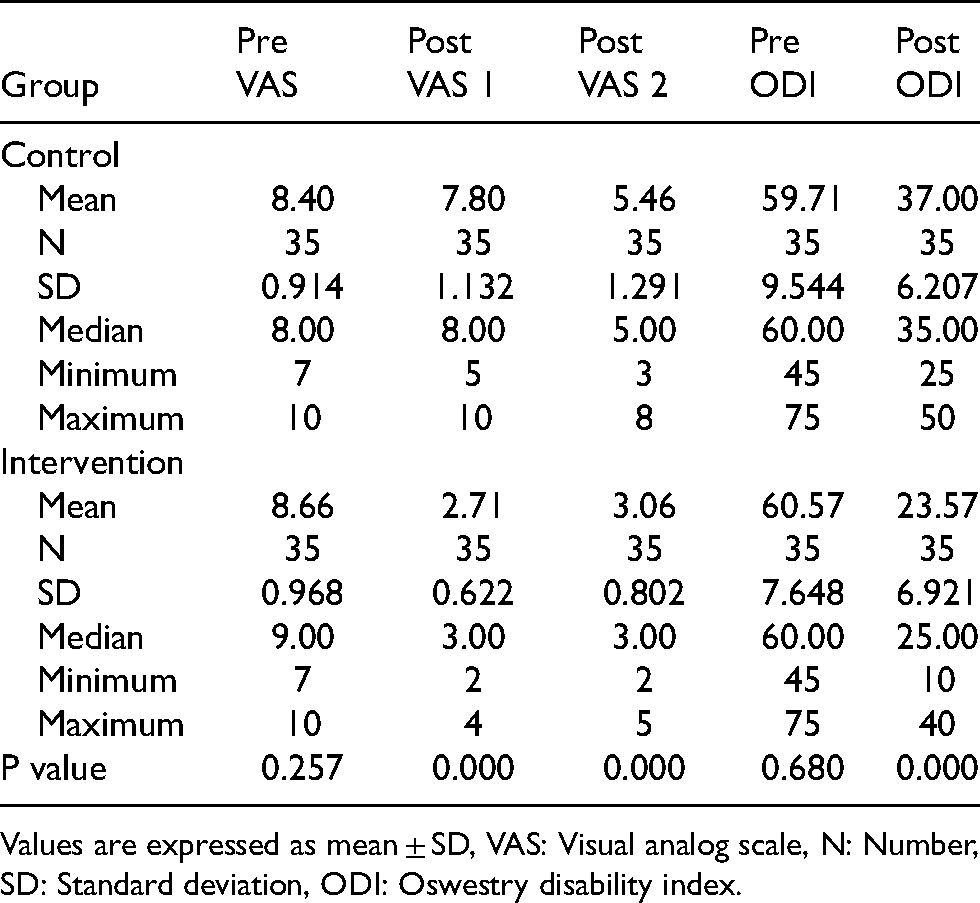
Values are expressed as mean ± SD, VAS: Visual analog scale, N: Number, SD: Standard deviation, ODI: Oswestry disability index.
Both conservative and vertebroplasty group showed significant improvement in the VAS/ODI with time. In the intervention group, the average pre VAS was 8.66. The average post VAS 1 was 2.71. The average post VAS 2 was 3.06. The average pre ODI was 60.57. The average post ODI was 23.57. Comparing between the intervention and control group for the post operative VAS and ODI, there were significant differences between both groups concerning post VAS 1, post VAS 2, post ODI as the P values were 0.00 (P values less than 0.05) in all relationships (Figures 3 and 4). There were no significant differences between both groups concerning the pre VAS and pre ODI as the P values were 0.257 and 0.680 respectively.
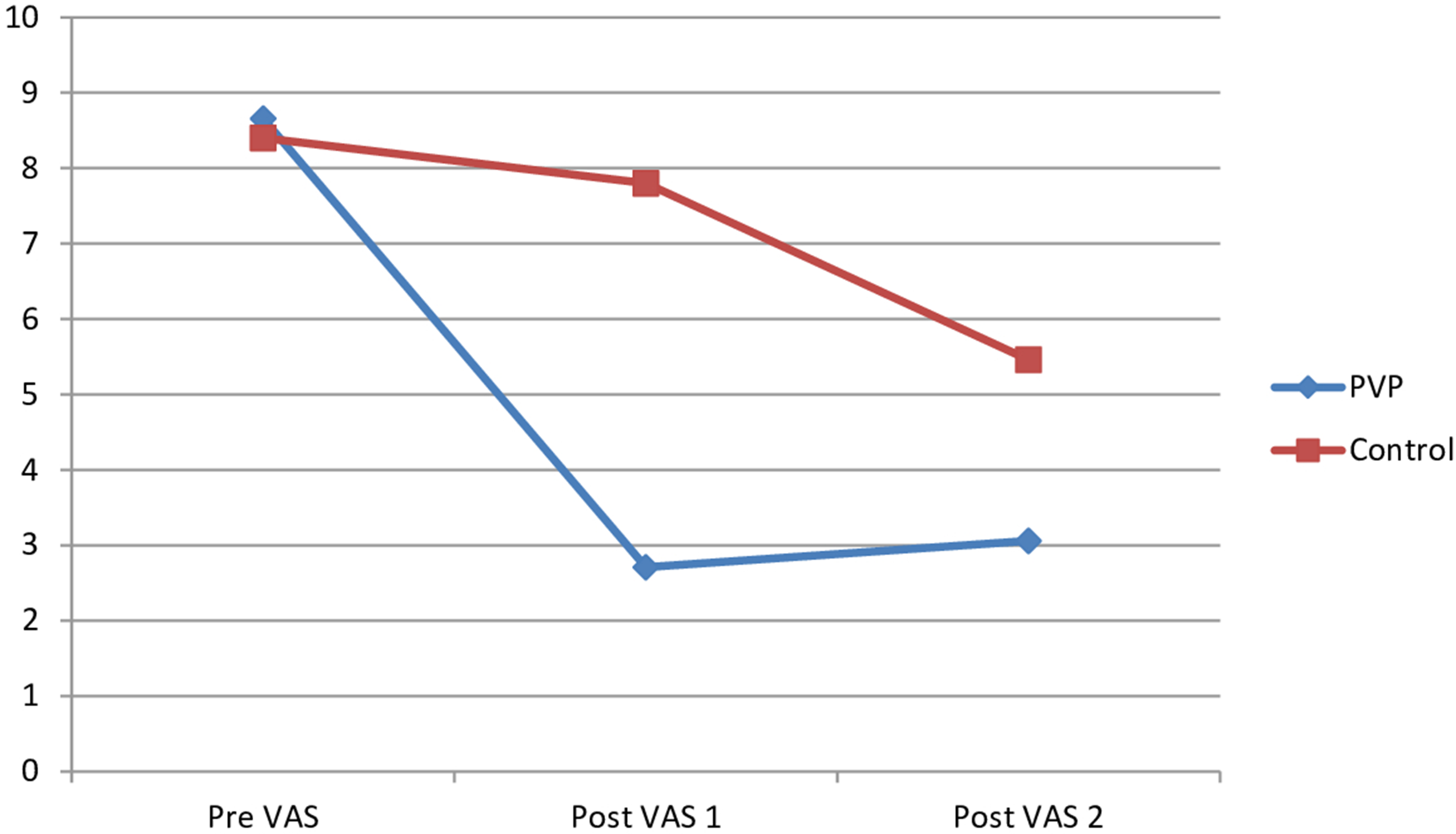
The changes in the visual analog scale in both groups.
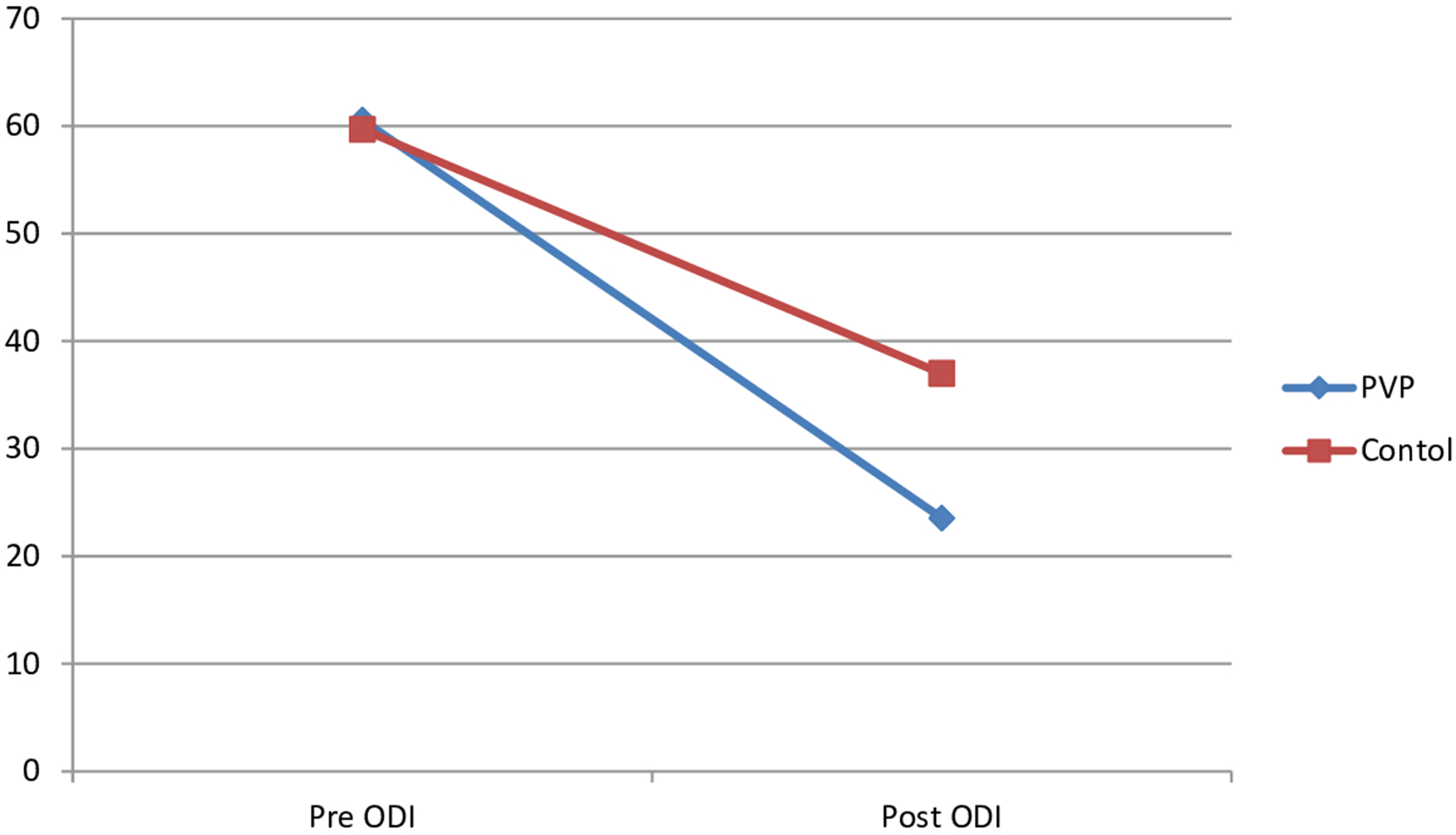
The changes in the Oswestry disability index in both groups.
Demographic characteristics of the patients in the intervention and control group [table 3]
In the intervention group, the average age was 67.20 years old. The average body weight was 60.49 kg. The number of females was 24 in the control group and 26 in the intervention group. The number of males was 11 in the control group and 9 in the intervention group. In the control group, the average age was 66.91 years old and the average body weight was 60.31 kg. There is no significant difference between the two groups concerning the age, sex and body weight as the P value was 0.555, 0.597 and 0.861 respectively.
Demographic characteristics of the patients in the intervention and control group.
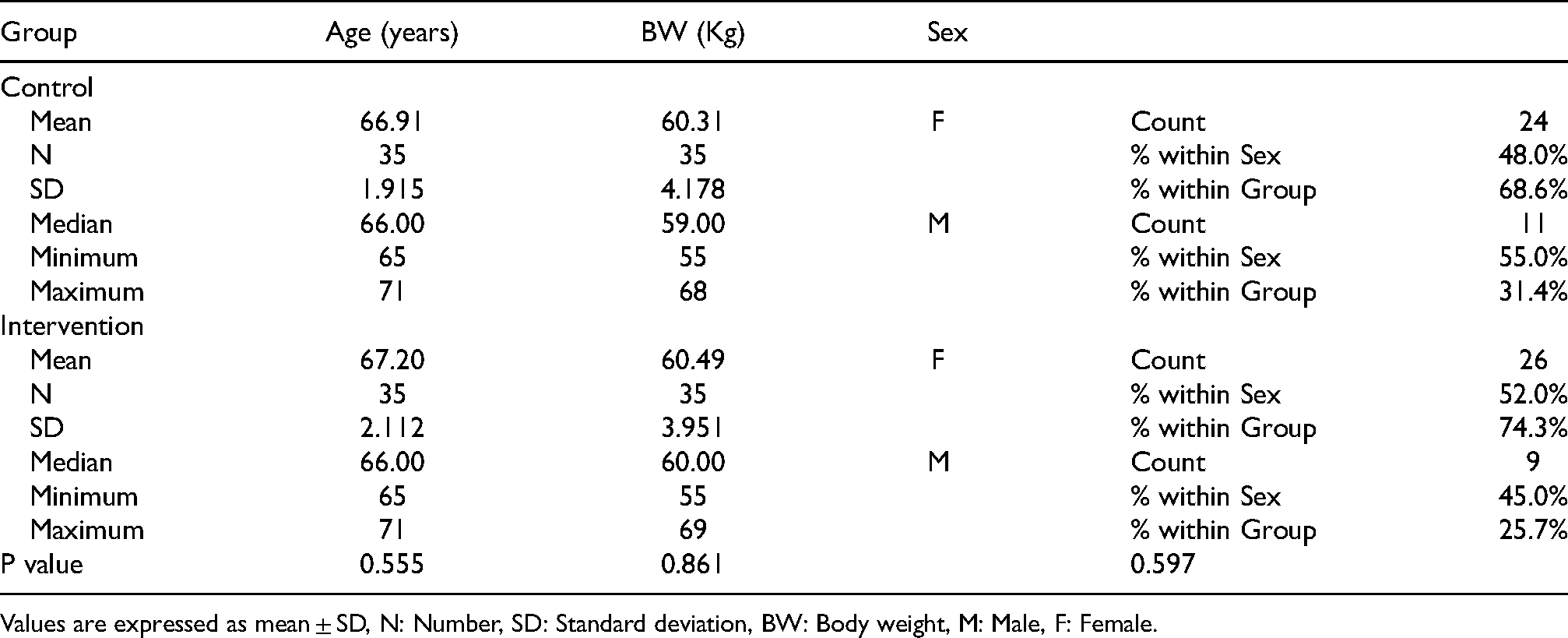
Values are expressed as mean ± SD, N: Number, SD: Standard deviation, BW: Body weight, M: Male, F: Female.
The number of thoracic spine fractures was 21 and 20 in the control and intervention groups respectively. The number of lumbar spine fractures was 14 and 15 in the control and intervention groups respectively. There is no significant difference between the two groups concerning the level of the procedure as the P value was 0.808. The average duration of symptoms before the procedure was 12.51 days.
In both intervention and control groups, all patients had severe back pain with VAS about 7 or more before treatment. Two patients in the PVP group had adjacent vertebral fractures during the study period and they were treated with repeat PVP. The post intervention VAS/ODI mentioned in our study also reflect the pain from the adjacent segment collapse and also the second PVP they received. There were no other complications (cement leakage, embolism, infection or neurological deficit) in the study. All patients within the intervention group had PVP within one month from the pain onset.
Discussion
Osteoporosis is more prevalent with increasing age of the population. It is considered a systemic disorder identified by decreased bone mass, micro architectural deterioration causing bone fragility. The fracture risk is increased especially in women. 13 OVCFs can lead to severe incapacitating back pain with resultant limited mobility and its associated complications. Conservative treatment may be sufficient in certain patients but many patients experience severe pain that seriously impact the patient quality of life. 14 Osteoporosis medications that aim at improving the bone marrow density are widely used in recent years. 15
Surgical treatment is rarely indicated in these elderly patients. This is due to the associated comorbidities and poor bone quality. 16 OVCFs have many potential consequences other than pain, limited mobility and narcotic addiction. These complications include urinary retention, kyphosis, insomnia, ileus and depression. 17 The real expenses resulting from this disorder are often underreported. Spine stabilization using PMMA has been previously done for metastatic disease. 18 The percutaneous injection of bone cement into partially collapsed vertebrae is performed with effective pain relief and very low incidence of complications. 19
Voormolen et al. showed that pain and mobility improvement after PVP is immediate. The improvement was significantly better than the optimal medical treatment in the short run. The study population involved eighteen patients in the PVP group and 16 patients in the control group. Scores in the PVP scores were affected by new occurrence of secondary vertebral fracture in two patients. VAS for severity of pain was assessed before, one day and two weeks after the treatment. Roland-Morris Disability (RMD) questionnaire scores and Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO) were assessed before and 2 weeks after beginning of treatment. All scores after PVP were significantly better than the scores during the medical treatment. 9
Blasco et al. conducted a randomized controlled study including 125 patients to show the efficacy of PVP versus conservative treatment. The VAS and quality of life parameters showed significant improvement in both groups but significant difference was present concerning VAS after 2 months of follow up. The improvement of Qualeffo (Quality of Life Questionnaire of the European Foundation for Osteoporosis) total score was significant after 6 months of follow up in the conservative group. Vertebral fractures had significant increased incidence in the PVP group. PVP was associated with rapid pain relief which had significant improvement in VAS after 2 months of follow up but it had increased incidence of secondary vertebral fractures. 20
A prospective study of 30 patients evaluating the PVP using fluoroscopic guidance was done. The mean age was 73.7 years. The VAS was assessed before and after the procedure. The VAS score was 8.91 + /− 1.82 before the procedure and it became 2.02 + /− 1.95 at follow up. The mean VAS score difference was statistically significant (P value > 0.001). One patient had epidural leak with no further complications and no intervention. 21
Mudano et al. 22 supposed that PVP increased the risk of secondary fractures. Researchers observed that injection of bone cement decreased the concavity of the vertebral endplate. In addition to 19% increase in vertebral body pressure, this leads to reduction of local spinal joints flexibility and the total load was elevated on adjacent vertebra by 17%. 23 Increased daily activities after PVP may also explain the excess stress on the adjacent vertebrae with increased risk of fractures. 24
Limitations
The follow up period in the intervention group wasn't long enough to assess late postoperative complications such as adjacent vertebral fractures.
Conclusions
Our study showed that PVP is highly effective and safe in the management of back pain due to OVCFs. It was associated with marked improvement of pain intensity and quality of life.
Authors' Statements
There were no conflicts of interest, and all the study processings are strictly adherent to the known ethical rules. There is no financial disclosure what so ever. The patients provided informed consent. The study aim and design was approved by the medical and ethical committee of the neurosurgery department at our institute.
We present our short term experience regarding the outcome of percutaneous vertebroplasty for patients with acute back pain due to acute osteoporotic vertebral compression fractures
Statement of authorship
The study idea, design, material selection, the procedures, and outcome assessment were all done by neurosurgery lecturer, Dr Mostafa Fekry. This manuscript has not been previously published, in whole or in part, or submitted elsewhere for review.
There were no conflicts of interest, and all the study processings were strictly adherent to the known ethical rules. There was no financial disclosure what so ever. The patients provided informed consent. The study aim and design was approved by the medical and ethical committee of the neurosurgery department, faculty of medicine at our institute.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.