
Abstract
Study Design
Retrospective chart review.
Objective
To evaluate the referral rate for long-term osteoporosis management following vertebral compression fracture treated by different specialties at a single academic institution.
Methods
Patients undergoing vertebral cement augmentation for painful osteoporotic compression fractures from 2009 to 2014 were identified. Medical records were reviewed to determine if the treating surgeon discussed and/or referred the patient for long-term osteoporosis management. Any referral for or mention of medical long-term osteoporosis management was counted as a positive response. Results were statistically analyzed with chi-square test.
Results
Two hundred fourteen patients underwent vertebral cement augmentation; 150 met inclusion criteria. Orthopedic surgeons treated 88 patients, neurosurgeons treated 39, and interventional radiology or pain management physicians treated 23. Orthopedic surgeons referred 82% of patients for osteoporosis management, neurosurgeons referred 36%, and interventional radiology/pain management referred 17%. The referral rate was significantly higher for orthopedic surgeons compared with either of the other two groups; there was no significant difference between neurosurgery and interventional radiology/pain management.
Conclusions
Among physicians who treat osteoporotic vertebral compression fractures, orthopedic surgeons more frequently address osteoporosis or refer patients for osteoporosis management compared with neurosurgeons and interventional radiologists or pain management physicians. The results of this study shed light on the disparity in how different specialties approach treatment of osteoporosis in patients with fractures painful enough to require surgery and highlight potential areas for improvement in osteoporosis awareness training.
Keywords
Introduction
The older population in the United States continues to grow rapidly. The United States Census Bureau reported that in 2012, ∼43 million individuals (13.7% of the population) were age 65 or older; by 2030, that number is projected to increase to almost 73 million (20.3%); and by 2050, it will reach nearly 84 million (20.9%). 1 Moreover, the percentage of “very elderly” (those over age 85) is projected to more than double from 1.9% in 2012 to 4.5% by 2050. Based on these forecasts, the number of osteoporosis-related fractures is also expected to increase. Fragility fractures, however, are not isolated events, but symptoms of an underlying disease process that predisposes patients to future injury. The most reliable predictor for future fragility fracture is a history of sustaining one. In many cases, the medical management of osteoporosis can prevent these injuries. 2 , 3
Initiatives such as the American Orthopaedic Association's “Own the Bone” program and similar international efforts (such as the International Osteoporosis Foundation's “Capture the Fracture”) have targeted orthopedic surgeons to raise awareness of the importance of establishing long-term medical management for osteoporosis in patients who present with fragility fractures. 4 , 5 These programs emphasize the value of establishing a fracture liaison service within an institution—a means by which patients with fragility fractures can be efficiently screened for osteoporosis and appropriate medical treatment can be initiated. 6 , 7 Indeed, referral to a fracture liaison service has been shown to decrease the risk of subsequent fragility fracture. 8 As a participating institution in “Own the Bone,” our facility instituted a fracture liaison service in October 2009. In addition to providing good patient care, recognition of osteoporosis as a contributing factor of a fracture also has medicolegal and financial (i.e., reimbursement) implications. 9 , 10 , 11
The most common fragility fractures are vertebral compression fractures. These injuries, however, are unique among fragility fractures as they are also frequently managed by physicians of specialties other than orthopedic surgery, including neurosurgery, pain management, and interventional radiology. These specialists are not the target of international osteoporosis awareness initiatives and do not surgically manage other osteoporosis-associated fractures. The purpose of this study was to evaluate the referral rate for long-term osteoporosis management following vertebral compression fracture among patients treated by different specialties at a single academic institution.
Materials and Methods
This study was approved by our Institutional Review Board. A retrospective chart review of all patients at a single academic hospital undergoing vertebral cement augmentation for painful osteoporotic compression fractures from March 2009 to March 2014 was conducted. Patients were identified by searching for American Medical Association Current Procedural Terminology codes for thoracic or lumbar vertebroplasty or kyphoplasty (22520, 22521, 22523, and 22524).12 Records were reviewed to determine the etiology of the patients’ fractures. The World Health Organization and the American Academy of Orthopaedic Surgeons definitions of “fragility fracture” as “a fracture by injury that would be insufficient to fracture normal bone”13 or “resulting from a fall from a standing height or less, or presenting in the absence of obvious trauma” 14 were used as guidelines. Patients who underwent the procedure for fractures of oncologic or traumatic etiology, as a component of revision spine surgery (e.g., augmenting pedicle screws), or who were already receiving long-term medical management of osteoporosis (other than dietary supplements of calcium or vitamin D) at the time of injury were excluded.
The medical records were reviewed to assess the specialty of the physician performing the procedure and to determine if the treating physician discussed and/or referred the patient for long-term osteoporosis management. Any referral for or mention of medical long-term osteoporosis management from the initial visit through the 90-day postoperative global period was counted as a positive response. Results were analyzed with chi-square test, and statistical significance was set at p < 0.05.
Results
A total of 214 patients underwent vertebral cement augmentation; 150 patients (76% women, average age 71.2 years) met the inclusion criteria (Fig. 1). Of those referred for osteoporosis management, 79% were women with an average age of 71.5 years (range 36 to 89 years); those not referred were 72% women with an average age of 70.7 years (range 41 to 100 years). This difference was not significant, nor was there a significant difference in age or gender between the groups based on treating physician specialty. Orthopedic surgeons treated 88 patients, neurosurgeons treated 39 patients, and either interventional radiology or pain management physicians treated 23 patients. The overall referral rate for osteoporosis management was 60% (90/150). Orthopedic surgeons had a referral rate of 82% (72/88), neurosurgeons had a referral rate of 36% (14/39), and interventional radiology/pain management physicians had a referral rate of 17% (4/23). The referral rate was significantly higher (p < 0.0001) for orthopedic surgeons compared with either of the other two groups; there was no significant difference between neurosurgery and interventional radiology/pain management (Fig. 2).
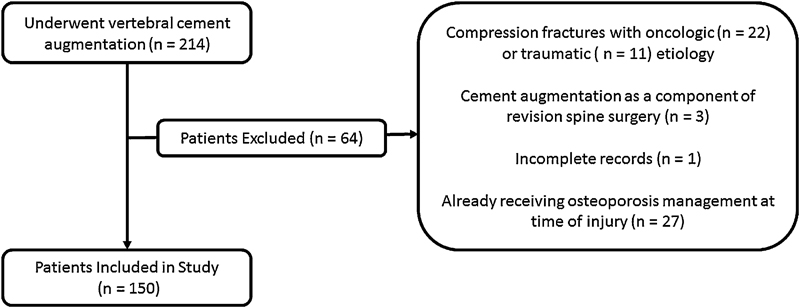
Application of exclusion criteria to sample population.
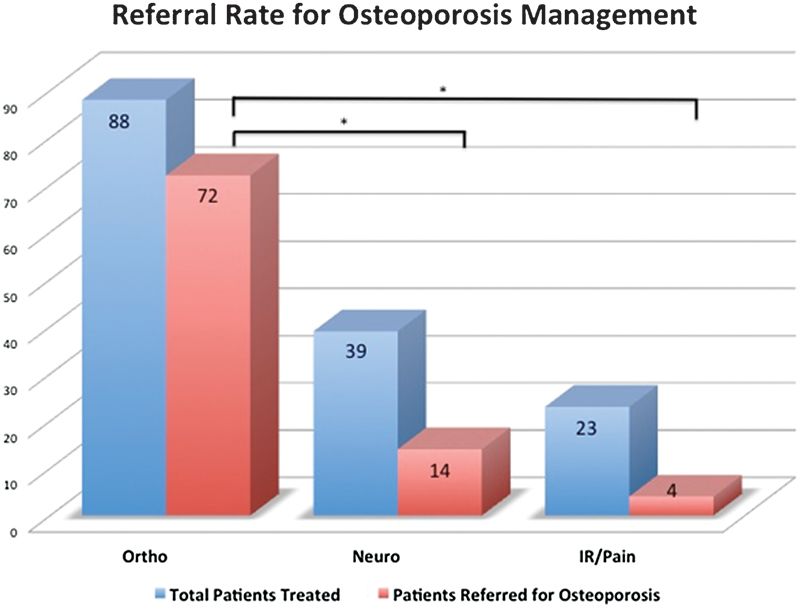
Osteoporosis referral rate based on surgeon specialty performing vertebral cement augmentation. *p < 0.0001. Abbreviations: Ortho, orthopedic surgery; Neuro, neurosurgery; IR/Pain, interventional radiology or pain management.
Discussion
Osteoporotic vertebral compression fractures are merely a symptom of an underlying metabolic bone disease, and referral for osteoporosis treatment should be standard practice when treating these injuries. Tosi et al reported that initiating the American Orthopaedic Association's “Own the Bone” program led to a significant improvement in patient education regarding osteoporosis (and the associated risks) and communication with the patients’ primary care providers. 4 In addition, Edwards et al found that early intervention following a fragility fracture (i.e., initiation of treatment during inpatient hospitalization) led to a significantly higher likelihood of osteoporosis management by the primary care provider (67% of patients at 6 months) compared with delayed intervention (i.e., sending a referral letter; 30%). Indeed, any intervention to evaluate or treat osteoporosis in patients sustaining fragility fractures significantly increased the likelihood of treatment compared with baseline at the time of the fracture (0%). 15 Clearly, the recognition of osteoporosis at the time a patient sustains a fragility fracture and appropriate referral improves the likelihood of osteoporosis treatment, which in turn can decrease the subsequent fracture risk.
Physicians also have incentives beyond good clinical practice to recognize osteoporosis. In addition to potential medicolegal implications, 9 , 10 failure to identify osteoporosis as a possible contributing factor to a fracture also has financial consequences for physicians in the United States. 11 The Centers for Medicare and Medicaid Services Physician Quality Reporting System criteria for 2015 specify that patients being treated for fragility fractures “should have documentation in the medical record of communication from the clinician treating the fracture to the clinician managing the patient's on-going medical care that the fracture occurred and that the patient was or should be tested or treated for osteoporosis.” 11 Failure to comply with this guideline can result in payment penalties to the treating physician. Per this guideline, the onus is on the treating physician to recognize the potential role of osteoporosis and act accordingly.
To our knowledge, our study represents the first report of the discrepancies between referral for osteoporosis treatment based on the specialty of the treating physician. Our results showed significant variation in the rate of osteoporosis referral following vertebral compression fractures depending on the specialty of the treating physician. Orthopedic surgeons had the highest referral rate, referring patients ∼2.3 times more frequently than neurosurgeons and 4.7 times more frequently than interventional radiologists and pain management physicians. This variation is particularly concerning given that our institution has a fracture liaison service.
Several studies have emphasized the importance of a fracture liaison service in treating patients with fragility fractures. Bogoch et al reported that 414 of 430 patients (96.3%) evaluated through their institution's fracture liaison service received appropriate evaluation of their osteoporosis. 16 The most common reason for not being evaluated was patient refusal (9/16), suggesting that the majority of patients identified through such a program would be amenable to evaluation and treatment. Huntjens et al recently presented the results of a prospective observational study of 3,322 patients who sustained fragility fractures, 1,412 of whom were evaluated at a facility with a fracture liaison service and 1,910 who were treated at a different facility without such a service. 8 Patients treated by the fracture liaison service demonstrated a 56% lower risk of subsequent nonvertebral fracture and a 35% lower mortality rate 2 years after injury than those who were not evaluated by the service.
Other studies have examined the variable attitudes of orthopedic surgeons in different countries regarding osteoporosis treatment. Bogoch and Snowden found that over 85% of Canadian orthopedic surgeons surveyed reported that they either refer for or initiate the workup for osteoporosis in patients treated for fragility fractures. 17 Dreinhöfer et al conducted an international survey of orthopedic surgeons and reported that although the majority of respondents in all countries (France, Germany, Italy, Spain, United Kingdom, and New Zealand) felt that the surgeon should identify and initiate osteoporosis treatment in these patients, there was variability between countries with respect to how patients were managed. 18 Whereas 80% of German and Italian surgeons would order a bone mineral density test themselves, most French, United Kingdom, and New Zealand surgeons would refer the patient to a primary provider or osteoporosis specialist. The study found a similar pattern in the willingness to prescribe osteoporosis medication. No studies to date have examined the attitudes or practice among physicians of different specialties who treat fragility fractures.
Although our study was not designed to assess the reasons for the discrepancy, it is possible that the disparity we noticed in referral rates may be due to a lack of comfort—or even a lack of awareness—in treating osteoporosis among neurosurgeons and interventionalists. As previously mentioned, osteoporosis advocacy programs are primarily aimed at orthopedic surgeons. In addition, many orthopedic surgeons who treat spinal fractures also treat fragility fractures of the extremities, which neurosurgeons and interventionalists do not. Moreover, orthopedic residency training includes formal education about bone metabolism and osteoporosis, something that is either not present or not emphasized in the training curriculum for neurosurgical residents or interventional pain specialists (e.g., radiology, anesthesiology, or physiatry). Therefore, multiple factors may have “primed” the orthopedic surgeons in our study, leading to a higher referral rate.
Our study has several limitations. This data only represents the referral patterns at a single academic institution, and the results may not be generalizable across all settings. Although a similar trend may exist elsewhere, a larger nationwide study would be needed to demonstrate this trend more conclusively. Although the results can only be used to institute policy and procedural changes at our own institution, the data suggests that further investigation into this referral pattern at other facilities is warranted and should be undertaken to ensure the appropriate patient care. Another limitation is that we only evaluated patients treated operatively, despite the fact that most osteoporotic compression fractures are treated nonoperatively. Although we suspect the trend would continue (or be even more pronounced) with the inclusion of nonoperatively treated fractures, we chose this approach for two reasons: first, these patients presumably represent the most symptomatic injuries, those with severe, unrelenting pain unresponsive to nonoperative treatment; second, the variety of terminology and diagnostic codes used for osteoporotic compression fractures (e.g., “thoracic fracture,” “compression fracture,” “lumbar fracture,” “pathologic vertebral fracture,” among others) makes it impractical to identify such patients in a retrospective chart review, as it would necessitate a radiographic review of virtually every thoracic or lumbar fracture (traumatic and pathologic) treated at our institution. Despite this limitation, we still identified a large number of patients who met our inclusion criteria. Finally, this study is retrospective. If, however, we were to conduct a prospective observational study, both the patients and the physicians would be aware of the study, introducing a degree of bias that might impact the referral rate for osteoporosis evaluation.
In conclusion, we found that, among physicians who treat osteoporotic vertebral compression fractures, orthopedic surgeons more frequently address osteoporosis or refer patients for osteoporosis management than neurosurgeons and interventional radiologists or pain management physicians. The results of this study shed light on the disparity in how different specialties approach the treatment of osteoporosis in patients with fractures painful enough to require surgery. Although larger studies are needed to confirm this trend on a national level, the results highlight potential areas for improvement in osteoporosis awareness training.
Disclosures
Scott D. Daffner, Personal stock and clinical trial: Pfizer; Personal stock: Amgen; Fellowship grant: AOSpine; Research grant: AO Foundation
Jonathan M. Karnes, Institutional research support: Amniox Medical, Inc.
Colleen M. Watkins, none