
Abstract
Background/purpose:
Sarcopenia is a predictor of fall, which is a leading cause of fragility hip fractures (FHF). Dual energy X-ray absorptiometry (DXA) is a costly measurement method for sarcopenia. Rehabilitation and prognosis can be determined by early functional outcomes. Meanwhile, 1-year mortality of FHF patients is high.
Aims:
(i) To report the prevalence of sarcopenia. (ii) To investigate the relationships of sarcopenia, premorbid factors, early functional outcomes and 1-year mortality in Hong Kong Chinese FHF patients.
Methods:
FHF patients admitted to Queen Elizabeth Hospital in Hong Kong from April 2016 to March 2017 were reviewed, including outcomes of relative appendicular skeletal muscle mass index (RASM), handgrip strength (HGS), New Mobility Score (NMS), Modified Functional Ambulation Classification (MFAC), Modified Barthel Index (MBI), Cumulated Ambulation Score (CAS), Elderly Mobility Scale (EMS) and 1-year mortality.
Results:
One hundred sixty nine FHF patients, aged 82.68 ± 7.32 years, were reviewed. Prevalence of sarcopenia in male and female were 71.4% and 37.7%, respectively. RASM was correlated with HGS of both dominant (r = 0.366, p < 0.001) and non-dominant side (r = 0.383, p < 0.001), NMS (rs = 0.239, p < 0.001), MFAC (rs = 0.192, p = 0.013), MBI (rs = 0.182, p = 0.018) and CAS (rs = 0.183, p = 0.019). RASM was not significantly correlated with EMS-1 (rs = 0.050, p = 0.525) and EMS-DC (rs = 0.092, p = 0.249). There was significant correlation between Sarcopenia and EMS-DC (rrb = −0.226, p = 0.004). Sarcopenia was marginally not associated with 1-year mortality (χ 2 = 3.745, p = 0.053). One-year mortality of FHF patients with Sarcopenia and without Sarcopenia were 16.5% and 7.1%, respectively. FHF patients with Sarcopenia were not statistically significant to be more likely to face mortality within 1 year (R 2 = 0.030, OR = 2.638, p = 0.060).
Conclusions:
Prevalence of sarcopenia was high in FHF patients and RASM was correlated with HGS and NMS, which can be easily administered as screening tools. Sarcopenia was correlated with early functional outcome but not with 1-year mortality. Early detection of Sarcopenia is crucial for early implementation of rehabilitation and treatment.
Introduction
Sarcopenia is a geriatric syndrome, characterized by age-related decline in skeletal muscle mass as well as muscle function (defined by muscle strength or physical performance). 1 It is a component of frailty associated with multiple co-morbidities, 2 lowered quality of life and functional capacity, 3 negative metabolic impacts, impaired cardiopulmonary fitness, 4 falls, 5 subsequent disabilities, or even mortality in elderly. 6 Additionally, association between sarcopenia and functional decline is significant, especially in men. 7 Sarcopenia is possibly one of the predictors for fall and subsequent osteoporotic hip fracture, 8 contributing to a higher health-care expenditure and economic burden in the society. 9
Diagnosis of sarcopenia
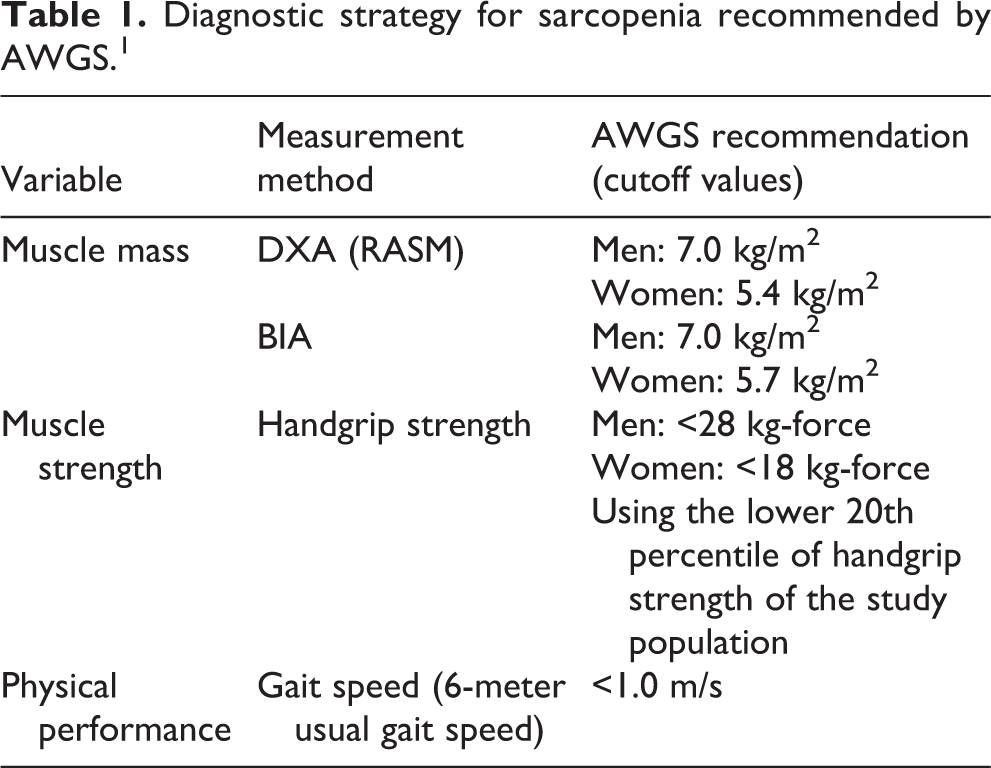
The diagnosis of sarcopenia was previously based on measuring body composition by bio-impedance analysis, dual energy X-ray absorptiometry (DXA), computed tomography, and magnetic resonance imaging. 10 In 2019, Asian Working Group for Sarcopenia (AWGS) updated the diagnostic strategy for sarcopenia in Asian population with defined cut-off values. 1 It composes of three main criteria including muscle mass, muscle strength and physical performance (Table 1). It is recommended to measure both muscle strength and physical performance as screening tests by assessing handgrip strength and gait speed respectively, 1 followed by measuring muscle mass only when either one or both are below the cut-off values. In this study, AWGS definition for sarcopenia was adopted.
Diagnostic strategy for sarcopenia recommended by AWGS. 1
Prevalence of sarcopenia
As reported in a study from Taiwan, the prevalence of sarcopenia was 10.8% in male and 3.7% in female in community-dwelling Chinese adults aged 65 years or above. 11 Yet, the impact of sarcopenia on osteoporotic fractures was seldom reported. In Japan, a study reported patients with hip fracture had a higher prevalence of sarcopenia and lower leg muscle mass than patients without hip fractures, implying that sarcopenia might be a risk factor for hip fractures. 12 Prevalence of sarcopenia is 81.1% for men and 44.7% for women in the target patient group review in this study. 12
Sarcopenia and hip fracture
Sarcopenia is one of the crucial problems in aged people. Muscle mass and strength are important to maintain the motor function in elderly. Sarcopenia is shown to be a significant predictor of fall-related injuries, leading to fragility fractures and subsequent hospital admissions. 12 Hip fracture is the most common fragility fracture of elder patients after fall. It causes disability, decrease in functional independence, mortality and significant healthcare burden.
According to the statistics retrieved from the Clinical Data Analysis and Reporting System (CDARS) under Hospital Authority in Hong Kong, the number of patient episodes headcounts of admission to acute hospitals under Hospital Authority with principle diagnosis of hip fracture exceeded 6500 each year from 2014 to 2018 (Figure 1). Among all acute hospitals retrieved, Queen Elizabeth Hospital (QEH) accounted for 12.1% in the past 5 years. More importantly, prevalence of sarcopenia in patients with hip fracture in Hong Kong is shown to be alarmingly high, which are 73.6% and 67.6% for men and women respectively as reported from a local study in 2016. 13 According to the available data in QEH in fiscal year 2018–2019, it is estimated that 97.4% of patients admitted with hip fracture were ambulatory, with Modified Functional Ambulation Classification (MFAC) categorized ≥III. Yet, the impact of sarcopenia to our patients was not studied previously.
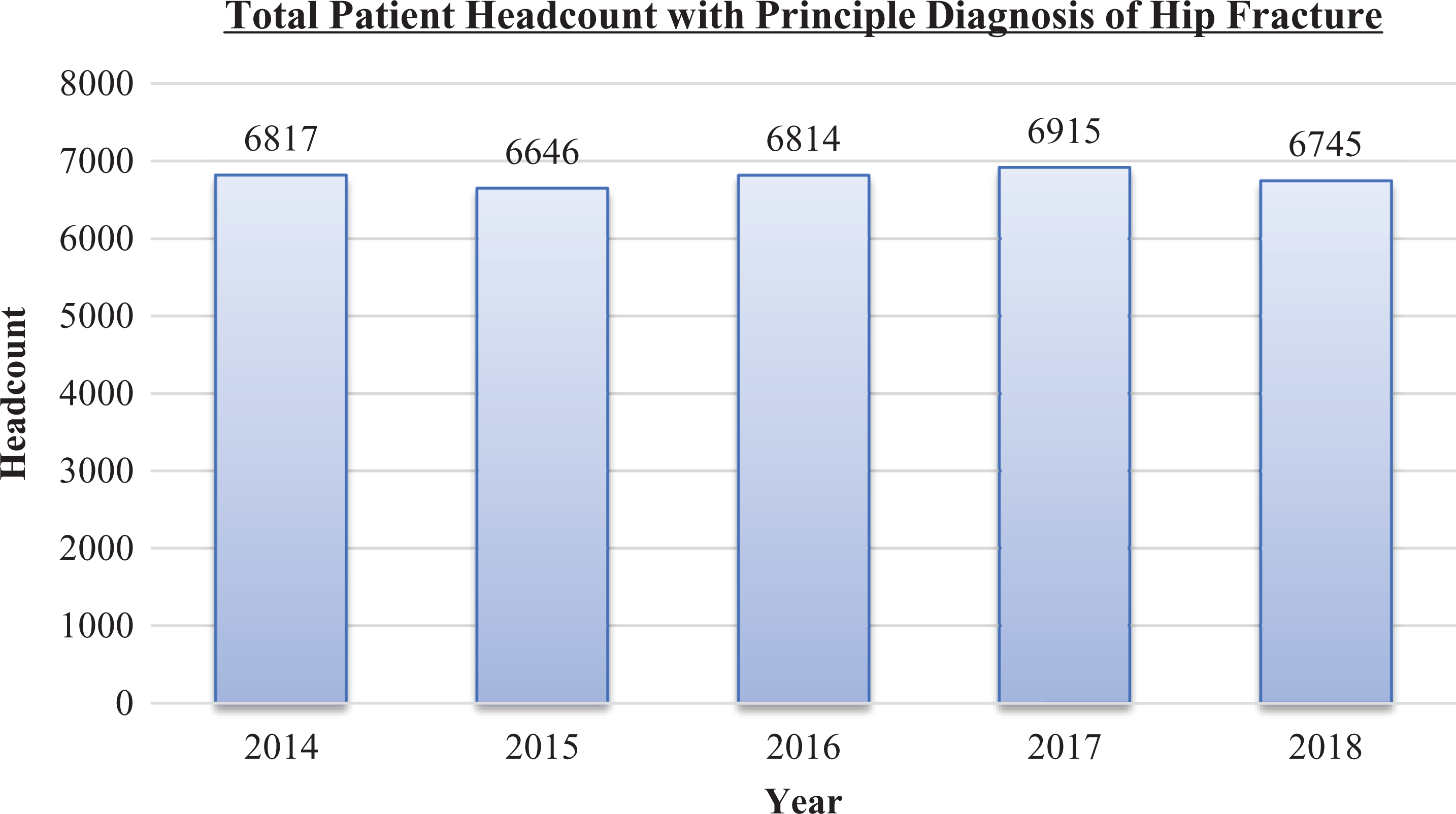
Total patient headcount of admission to acute hospitals under hospital authority with principle diagnosis of hip fracture from 2014 to 2018 (data retrieved from CDARS, hospital authority on 3 June 2019).
Sarcopenia, muscle strength and physical performance
DXA is a validated but relatively costly measurement method for sarcopenia. It measures relative appendicular skeletal muscle mass index (RASM). Recent literatures have shown positive relationships among sarcopenia, muscle mass and muscle strength. However, there were limited studies on physical performance for sarcopenic individuals. One local study demonstrated that RASM was correlated with handgrip strength (HGS), body weight, and body mass index (BMI). 13 Nevertheless, the time interval between fall and DXA measurement was 14 days in average. Besides, it was an unblinded study for the assessors with no standardized assessment procedures. 13 More importantly, physical performance factors were not studied.
Gait speed is an established measurement method for physical performance, 1 but there are limited studies investigating the correlation of sarcopenia with physical performance. Limited studies were done to study the correlation between sarcopenia and different factors, including muscle mass, muscle strength and physical performance in Hong Kong Chinese fragility hip fracture (FHF) patients. 1,10 In this study, both pre-operative and post-operative mobility outcome measures were adopted into research as physical performance. The result of the present study may be a pivotal piece of information that facilitate the potential development of more cost-effective diagnostic and preventive measures for hip-fractured patients in the foreseeable future.
Rehabilitation, prognosis and mortality of patients with hip fracture
Hip fracture is mostly treated operatively, followed by rehabilitation to enhance functional recovery and decrease complications. Rehabilitation plan and prognosis can be determined by early functional outcome. Meanwhile, 1-year mortality of hip fracture patients is high, approximately 18% in Hong Kong. 14 Numerous factors are shown to be significant prognostic predictors; however, limited studies have investigated the contribution of sarcopenia on functional outcome and 1-year mortality.
Objectives of this study
The objectives of this study are (i) to report the prevalence of sarcopenia; (ii) to investigate the correlation of sarcopenia and different factors; and (iii) to investigate the relationship among sarcopenia, early functional outcome and 1-year mortality in Hong Kong Chinese geriatric ambulatory patients with hip fracture.
Methods
Study design
This was a retrospective observational study. Ethical approval was obtained from the Kowloon Central Cluster/Kowloon East Cluster Research Ethics Committee/Institutional Review Board.
Subjects
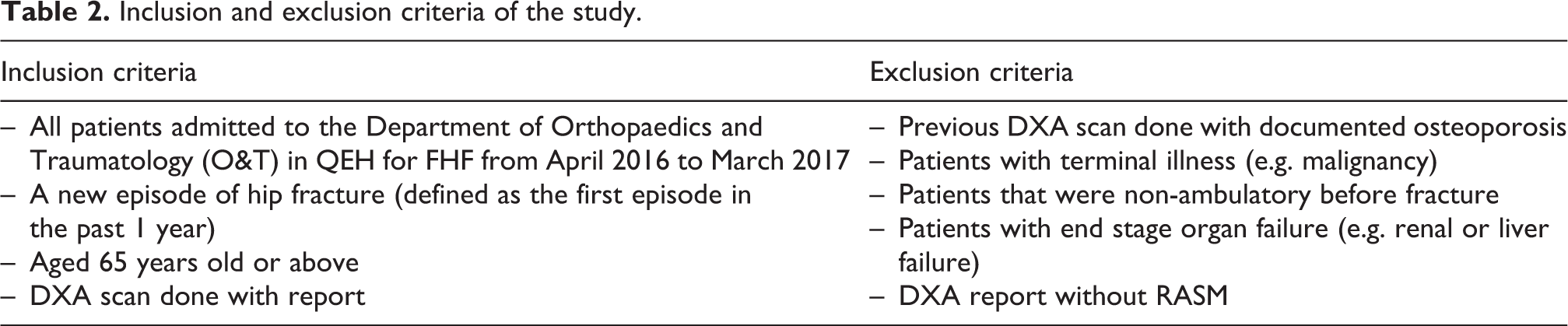
All patients aged 65 years or above with principal diagnosis of hip fracture admitted to QEH in Hong Kong from April 2016 to March 2017, fulfilling the inclusion and exclusion criteria (Table 2) were recruited. All subjects were assessed by orthopaedic surgeons and physiotherapists on admission. Usual assessments and interventions were provided under the treatment protocol in QEH with patients’ informed consent. Personal demographics and measurement data were retrieved (Figure 2).
Inclusion and exclusion criteria of the study.
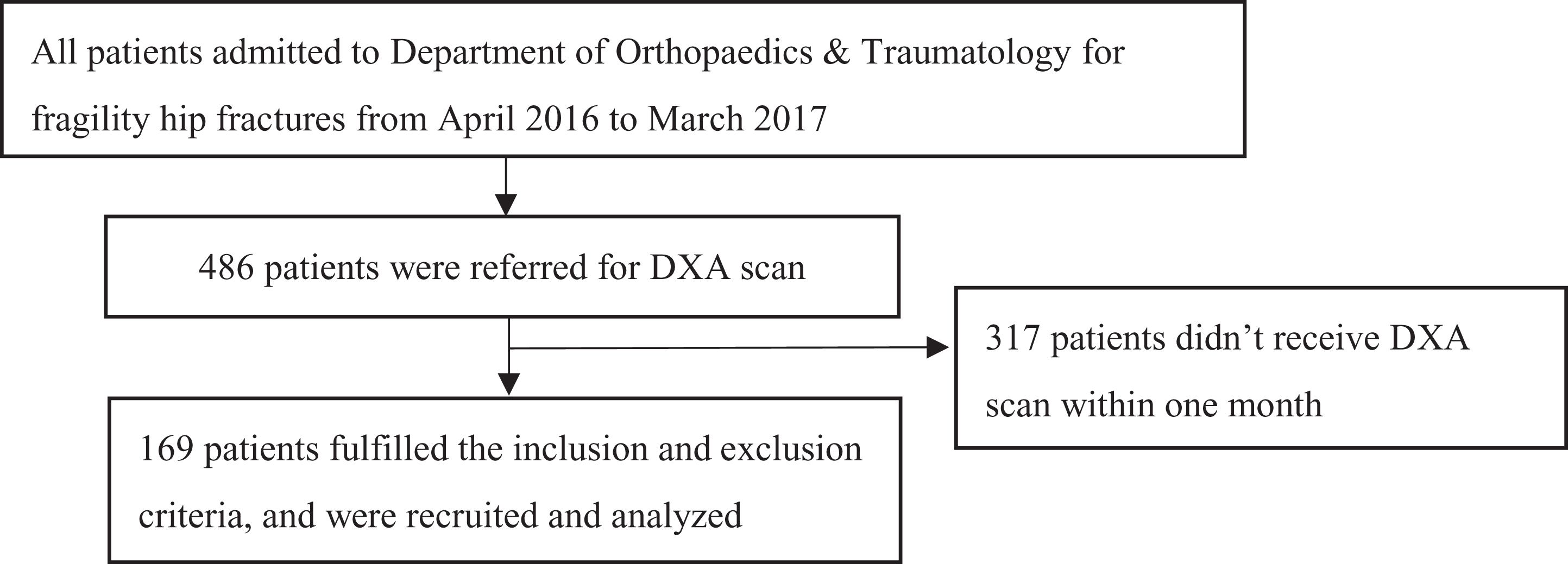
Flowchart of subject recruitment.
Physiotherapists from QEH specialized in O&T were responsible for subject recruitment, data retrieval, data analysis and follow-up of the subjects.
Outcome measures
Muscle mass
DXA scan was performed for each subject after admission for assessing body composition, 1 especially for the appendicular and whole lean body mass. Relative appendicular skeletal muscle mass index (RASM) was calculated by normalizing the sum of lean muscle mass in upper and lower limbs divided by square of body height. According to AWGS recommendation, the cutoff value for RASM are 7.0 and 5.4 kg/m 2 in men and women, respectively. 10
Muscle strength
Physiotherapists assessed the muscle strength of the patients by using Jamar dynamometer to measure HGS, which is a reliable method, 15 within first week after admission. The measurement procedure was based on the standard protocol recommended by the American Society of Hand Therapists, using the second position of the Jamar dynamometer. The subject was instructed to squeeze the handle maximally and sustain for 3–5 s in sitting with shoulder adducted and neutrally rotated, elbow flexed at 90°, forearm in mid-prone and wrist in neutral to 30° extension, with neutral radioulnar deviation. Three successive measurements were taken for each dominant and non-dominant hand with a rest of 15–20 s between measurements. The maximum readings for both hands were recorded. Patient with unknown hand dominance was assumed to be right-hand-dominant. According to AWGS recommendation, the cutoff values are 28 kg-force for men and 18 kg-force for women. 1
Physical performance
Several outcome measures were used to evaluate the physical performance of the subjects, both in pre-fracture and post-operation phases.
Pre-morbid mobility status
New mobility score (NMS)
NMS is a reliable, valid and easily applicable test, which can reveal the pre-morbid functional performance of patients with hip fracture. 16 It is a composite score to measure the subject’s ability to perform indoor walking, outdoor walking and shopping in pre-fracture status. Each item scored on a 4-point Likert scale and the total score ranges from 0 to 9. 16
Modified functional ambulation classification
MFAC is another reliable and valid assessment tool to categorize the functional ambulation status of patients with hip fracture. 17 It is a 7-point Likert scale, ranging from I to VII. It evaluates the ambulation level of the subjects before hip fracture.
Modified barthel index
Modified barthel index (MBI) was used to measure the level of functional and physical performance of subjects. 18 It is a 10-item performance-based assessment consisting of five responsive scales that evaluates functional activities, personal care and mobility of subjects. The total score ranges from 0 to 100.
Post-operative mobility status
Cumulated ambulation score
Cumulated ambulation score (CAS) is a valid score to predict short-term functional and mobility outcome of patients after hip fracture operation. 19 It was assessed on the first three post-operative days, with a cumulated score ranging from 0 (totally dependent) to 18 (fully mobile). 19
Elderly mobility scale
Elderly mobility scale (EMS) was used to measure the functional and physical performance of the subjects. 20 It is a 7-item-performance-based test including tasks on transfer, gait and balance, which are essential for basic ambulation and daily activities, with a total score ranging from 0 to 20. Moreover, it is a well-validated and useful measurement tool to assess the physical performance of patients in hospital setting. 20 EMS was recorded at the time of first walk (EMS-1) and discharge (EMS-DC) from acute hospital.
One-year mortality
One-year mortality was used to assess the long-term prognosis and outcome of the subjects. It was retrieved from the electronic platform, Clinical Management System (CMS), of the Hospital Authority of Hong Kong.
Statistics
Prevalence of sarcopenia was reported according to the AWGS definition by analyzing RASM and HGS. Correlation between RASM and HGS, NMS, MFAC, MBI and CAS was investigated by Pearson’s correlation and Spearman correlation analysis. Correlation between Sarcopenia and EMS was evaluated by rank-biserial correlation analysis. Correlation between Sarcopenia and 1-year-Mortality was evaluated by Pearson’s Chi-square test. Prediction model of 1-year mortality was evaluated using logistic regression analysis. All analysis was two-tailed and the level of significance alpha-value was set at 0.05 for statistical analysis.
Results
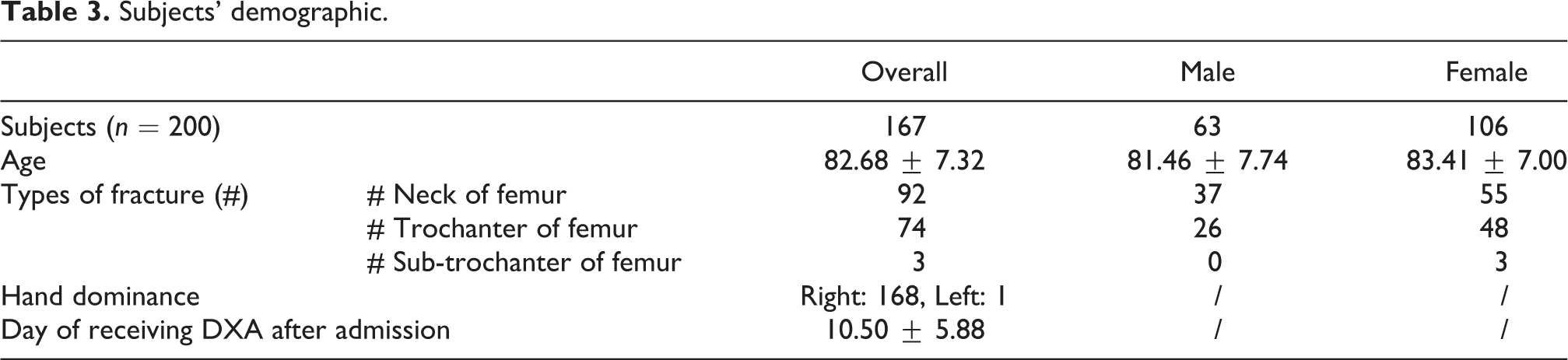
One hundred sixty nine patients (63 males, 106 females) were reviewed. Their mean age was 82.68 ± 7.32 years old. Subjects’ demographic is shown in Table 3. Different outcome measures in all subjects are shown in Table 4.
Subjects’ demographic.
Different outcome measures in all subjects, male subjects and female subjects.
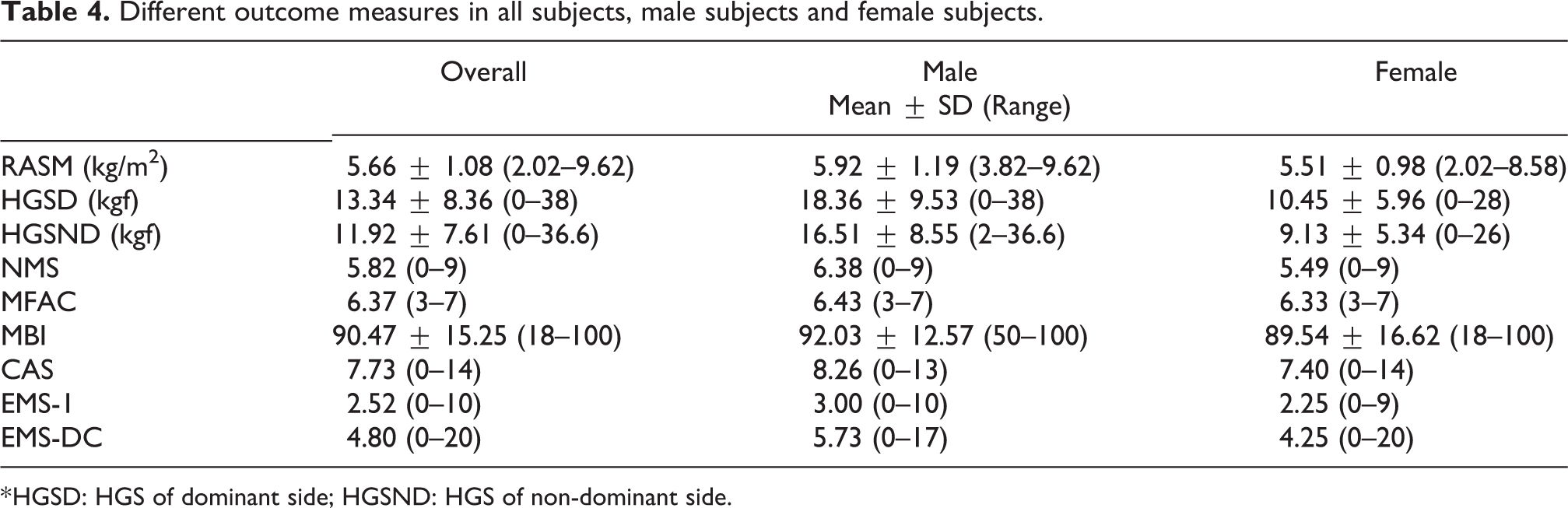
* HGSD: HGS of dominant side; HGSND: HGS of non-dominant side.
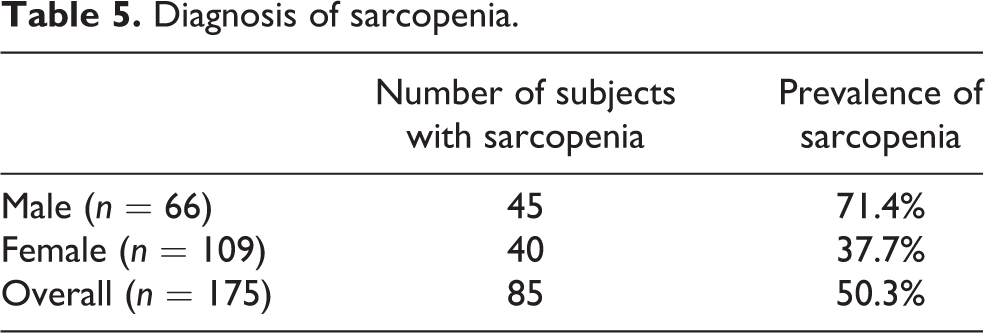
In this study, the prevalence of sarcopenia in male and female were 71.4% and 37.7%, respectively (Table 5). RASM was significantly correlated with different pre-morbid outcomes, including HGS of both dominant (r = 0.366, p < 0.001) and non-dominant side (r = 0.383, p < 0.001) with moderate relationship, NMS (rs = 0.239, p < 0.001), MFAC (rs = 0.192, p = 0.013) and MBI (rs = 0.182, p = 0.018) with weak relationship (Table 6). RASM was also significantly correlated with CAS (rs = 0.183, p = 0.019) but with weak relationship. RASM was not significantly correlated with EMS-1 (rs = 0.050, p = 0.525) and EMS-DC (rs = 0.092, p = 0.249).
Diagnosis of sarcopenia.
Correlation of RASM and different outcome measures.
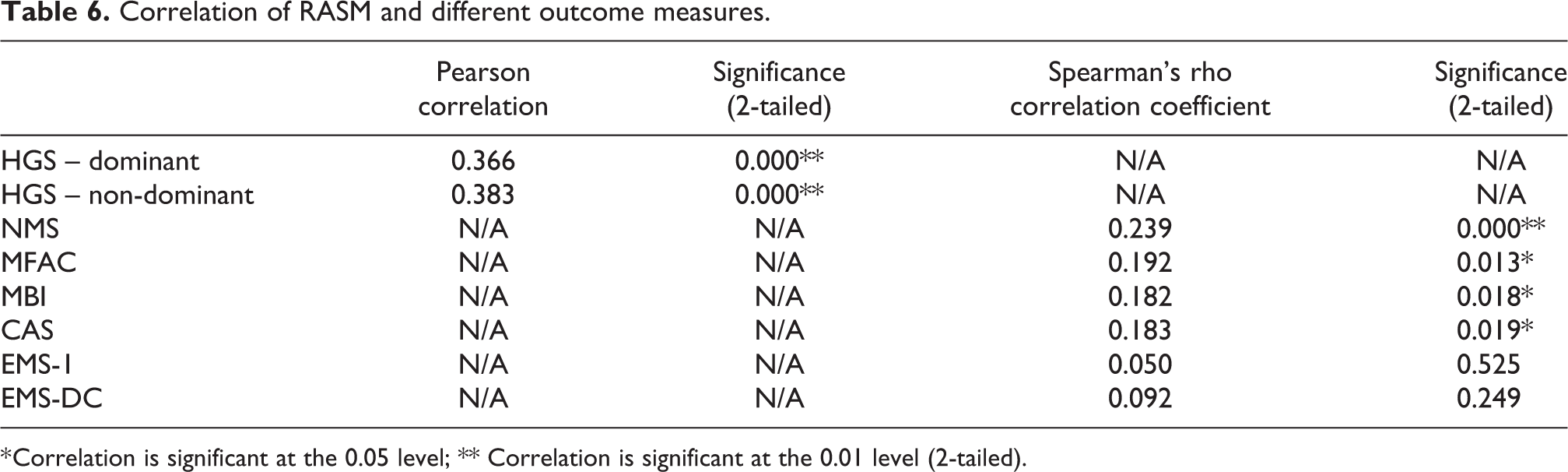
* Correlation is significant at the 0.05 level; ** Correlation is significant at the 0.01 level (2-tailed).
There was significant correlation between Sarcopenia and EMS-DC (rrb = −0.226, p = 0.004), but not between Sarcopenia and EMS-1 (rrb = −0.079, p = 0.321). One-year mortality rate was 11.8%. Sarcopenia was marginally not associated with 1-year mortality (χ 2 = 3.745, p = 0.053). One-year mortality rate of patients with Sarcopenia and without Sarcopenia was 16.5% and 7.1%, respectively. However, patients with Sarcopenia were not statistically significant to be more likely to face mortality within 1 year (R 2 = 0.030, OR = 2.638, p = 0.060).
Discussion
Prevalence of sarcopenia
According to the AWGS criteria, the prevalence of sarcopenia in community-dwelling Chinese elderly in male and female was 10.8% and 3.7%, respectively. 11 In our study, prevalence of sarcopenia in Hong Kong Chinese FHF patients for male and female were 71.4% and 37.7%, respectively, which were similar to previous local study. 13 Thus, there is a significantly higher proportion of FHF patients than community-dwelling elderly sustaining sarcopenia. Sarcopenia is associated with osteoporosis in patients with hip fracture. 8 Loss of muscle strength is related to loss of muscle mass, 21 which may result in fall and subsequent fragility fracture in elderly. 22 Primary prevention is more important than secondary prevention. Regular body check and screening of sarcopenia should be implemented in local community-dwelling elderly to minimize the healthcare expenditure and economic burdens. 23 Regular exercise comprising of muscle strengthening and resistance training program should be promoted.
In addition, it is consistent that the prevalence of sarcopenia in male is higher than that in female in Asian population. 3,7,12,13 It is known that there is a larger proportion of female elderly suffering from osteoporosis than male elderly. 24 Post-menopausal hormonal changes would lead to loss in bone mineral density. There is a higher risk that fragility fracture is resulted from osteoporosis. 25 Sarcopenia can be one of the essential risk factors leading to fall in ambulatory geriatric population. 26 However, it is not proven to cause fractures directly. Further studies are needed to illustrate the relationship of sarcopenia, fall and subsequent fractures. Nevertheless, difference in exercise habit in gender in Asian community is one of the potential factors associated with sarcopenia. 27 More importantly, male hypogonadism with lower testosterone level due to aging is common and can result in reduction of muscle mass and muscle strength. 28 Further studies are warranted.
Correlation with sarcopenia
RASM was shown to be positively correlated with handgrip strength (HGS) of both dominant and non-dominant side with moderate relationship, in which the correlation coefficient with RASM was 0.366 and 0.383, respectively. Loss of muscle mass and muscle strength with aging occur in a multifactorial basis. 29 Hence, sarcopenia is undoubtedly a multifactorial syndrome. 1,10 Handgrip strength isn’t the sole factor to be correlated with sarcopenia. Other measures on muscle strength, including isometric quadriceps strength, and physical performance should also be taken into account.
No previous literatures have investigated physical performance outcomes related to sarcopenia in geriatric patients with hip fracture. Our study is the first study to study the relationship of physical performance and sarcopenia in fragility hip fracture (FHF) population. Several physical performance measurement tools, namely NMS, MFAC, MBI and CAS, were shown to be statistically and positively correlated with sarcopenia, but with weak relationship. Pre-morbid MBI had a significant ceiling effect in the patients with hip fracture, with 41.4% of subjects scored full score. In contrast, NMS, MFAC and CAS consist of small range of score only, so there was a certain extent of limitation in discriminating subjects’ physical performance. Among these outcomes, NMS contributed to the highest and the most significant positive correlation (rs = 0.239, p < 0.001) with sarcopenia. NMS consisted of three questions scored on a 4-point Likert scale only. 16 It is easily administered and time-efficient.
Certainly, it is impossible to perform 6-minute-walk-test, Timed-Up-And-Go or gait speed test to assess the pre-morbid physical performance of the FHF patients. 1 Hence, being a physician or a physiotherapist, in order to estimate the extent of sarcopenia of the patients, it is crucial and applicable to use HGS measurement and NMS as the screening tool in FHF patients who admitted to hospital. As sarcopenia is associated with poorer functional outcomes and even higher mortality rate, 6 more intensive and focused training and intervention are possibly the preliminary measure to prevent other complications in FHF patients. 30
Functional outcome
This was the first study to establish the relationship between sarcopenia and functional outcome in FHF patients in Hong Kong. In this study, RASM was significantly correlated to CAS (rs = 0.183, p = 0.019) and sarcopenia was significantly correlated to EMS-DC (rrb = −0.226, p = 0.004), which revealed the mobility status during first three post-operative day and discharge, respectively. Undoubtedly, patients with sarcopenia are characterized by low muscle mass, low muscle strength and low physical performance. 10 As muscles are crucial in maintaining functional performance and preventing falls, decreased skeletal muscle mass diminishes activities in daily living and hence affects physical performance. 12,31 Apart from reduced motor capacity, weakened visual and vestibular skills in maintaining balance are also encountered in elderly with less active lifestyle. 32 Despite undergoing post-operative rehabilitation for sarcopenic patients, poorer functional outcomes were resulted and more time would be needed to develop adequate muscle strength and mass, and balance for normal daily functions when compared with those without sarcopenia.
Moreover, sarcopenia is independently associated with cognitive impairment, and declines in cognitive function can potentially transit to dementia. 33 Cognitively impaired patients may not be able to comply with exercise protocol or rehabilitation plan, leading to slower recovery. Besides, recent study proved that cognitive impairment is associated with mobility and functional performance. 34 With low baseline functional performance before suffering from hip fracture, longer rehabilitation period or hospitalization following hip fracture may be encountered. Thus, sarcopenic patients suffering from FHF exhibited decrements on functional tasks.
One-year mortality
To our knowledge, the present study was the first to explore the association between sarcopenia and 1-year mortality rate. We only found a marginally positive association between sarcopenia and 1-year mortality (χ 2 = 3.745, p = 0.053). In short, patients with sarcopenia possibly had a higher rate of decease within 1 year. Although there was no statistically significance, 1-year mortality rate of patients with sarcopenia (16.5%) was apparently higher than that of patients without sarcopenia (7.1%). Research reviewed that sarcopenic patients were prone to frail condition and poor general health. 12 Blood glycohaemoglobin in men was significantly higher and arterial stiffness was greater in women. 35 Moreover, low relative muscle mass was correlated with raised incidence of left ventricular diastolic dysfunction, indicated as the filling dysfunction of left ventricle, is one of the prediction of heart failure development. 36 Muscle dysfunction also doubled the risk of nosocomial infection as well as causing urinary disorder and diminishing swallowing function. 12 Unintentional weight loss resulting from rapid muscle loss with poor nutritional status was significantly associated with death. 37 Thus, sarcopenia diagnosis should be taken into account as a vital indicator of mortality. Further studies are warranted.
Limitation of study
Due to the limitation of study design, the data was retrieved retrospectively. There was no close monitoring or supervision on the assessment by different physicians and physiotherapists. Moreover, there was possible bias on different measurement tools due to lack of blinding of assessors. These may influence the accuracy of different measurement outcomes. In addition, there were potential bias in subject recruitment. 286 subjects were excluded as their DXA scan was not scheduled within one month to one year after admission due to long waiting list.
There were inevitable factors affecting the accuracy in reflecting subjects’ actual pre-morbid muscle mass, as DXA scan was ordered after sustaining a hip fracture and hospital admission. Period of immobilization varied among subjects. The longer the period of immobilization, the more severe the muscle atrophy. 38 In addition, period of awaiting DXA scan varied among subjects. In our study, the mean of day of receiving DXA after admission was only 10.50 ± 5.88, therefore, the potential muscle mass deterioration due to immobilization was minimized.
Meanwhile, all types of hip fractures were involved. Subjects with different types and extent of hip fracture would receive different kinds of operation or management, contributing to various post-operative physical performance. 39 Hip fracture is indeed a multifactorial problem. Psychosocial factors and cognitive function should be considered as confounding factors of the post-operative functional outcomes. 40,41
Conclusion
Prevalence of sarcopenia was high in Hong Kong Chinese FHF patients. RASM is positively correlated with HGS and NMS, which can be easily administered and possibly used as the screening tool of sarcopenia. Sarcopenia was also shown to be correlated with early functional outcome but not with 1-year mortality. Therefore, early detection of Sarcopenia is crucial for early implementation of appropriate rehabilitation and treatment.
Footnotes
Acknowledgements
Physiotherapy Department, Queen Elizabeth Hospital, and Department of Orthopaedics and Traumatology, Queen Elizabeth Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.