
Abstract
Objectives:
Bone lesions from multiple myeloma may lead to pathological fracture of the proximal femur, requiring either fixation or arthroplasty. Little is known about the impact of multiple myeloma on hip fracture care. We investigated whether the patients with multiple myeloma undergoing surgical treatment of hip fractures would be at increased risk for adverse outcomes versus patients who sustain a hip fracture without multiple myeloma.
Methods:
Using discharge records from the Nationwide Inpatient Sample (2002-2011), we identified 2 440 513 patients older than 50 years of age with surgically treated hip fractures. Of which, 4011 (0.2%) were found to have multiple myeloma. We compared perioperative outcomes between the patients with multiple myeloma and the nonmultiple myeloma patients using multivariable logistic regression modeling.
Results:
Patients with multiple myeloma were more likely to have several postoperative complications, such as in-hospital pneumonia (odds ratio [OR]: 1.31, 95% confidence interval [CI]: 1.14-1.51), sepsis (OR: 1.72, 95% CI: 1.32-2.25), surgical site infection (OR: 1.66, 95% CI: 1.38-2.00), and acute renal failure (OR: 1.28, 95% CI: 1.14-1.43). We found that myeloma was not associated with increased inpatient mortality, myocardial infarction, respiratory failure, thromboembolic events, or pulmonary embolism.
Conclusion:
Patients with multiple myeloma are at increased risk for immediate postoperative complications following surgical treatment of hip fractures including in-hospital pneumonia, surgical site infection, and acute renal failure but not hospital mortality, when compared to hip fracture patients without multiple myeloma. Perioperative management of hip fractures in patients with myeloma may be optimized by increased awareness of these risks in this subset of patients.
Introduction
Multiple myeloma is the most common primary malignancy of bone and commonly presents with bone pain, fatigue, pathologic fractures, and recurrent infections. 1 –3 In the past decade, substantial improvements (high-dose chemotherapy, autologous and allogeneic stem cell transplantation, and immunomodulatory drugs) have been made in the treatment of myeloma, and the number of myeloma cancer survivors is increasing. 4 –8 Hip fractures in patients with multiple myeloma require surgery that is often more extensive than a standard hip fracture. There may be multiple pathologic bone lesions that are typically treated with either a long-stem arthroplasty or a long intramedullary nail. 9 –11 Long devices could potentially increase the risk of embolic-related phenomena or intraoperative morbidity and mortality. 12 –15
Patients with a malignant diagnosis are at increased risk of postoperative complications. 1,8,16,17 The literature, however, is sparse in regard to in-hospital outcomes of patients with multiple myeloma undergoing surgical treatment of hip fractures.
Using a large health-care utilization database, we sought to characterize the relationship of multiple myeloma with major in-hospital complications, mortality, surgical site infection, thromboembolic events, prolonged length of stay, and nonroutine discharge following hip fractures. We hypothesize that the patients with multiple myeloma undergoing hip fracture surgery are at greater risk for early postoperative morbidity and mortality than patients undergoing hip fracture surgery without multiple myeloma.
Methods
Data Source and Study Design
We conducted a retrospective population-based analysis using 2002 to 2011 discharge records from the Nationwide Inpatient Sample (NIS), the largest all-payer inpatient database in the United States. 18 The NIS is compiled annually by the Agency for Healthcare Research and Quality and provides clinical and resource utilization information from over 1000 nonfederal short-term hospitals sampled to approximate a 20% stratified sample of the US community hospitals. Participating hospitals are sampled based on geographic region, location (urban/rural), ownership, teaching status, and bed size, with sampling probabilities proportional to the number of the US community hospitals in each stratum. Discharges are weighted based on the sampling scheme to ensure national representativeness. 19 For each NIS record, up to 15 procedures and 25 diagnoses (15 prior to 2009) are coded using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). This study was exempt from approval by our institutional review board, because the data are publicly available and deidentified.
Identification of Sample and Definitions
A cohort of patients with a primary ICD-9-CM diagnosis for proximal femur fracture (codes 820.0 and 820.1 for transcervical, 820.2 and 820.3 for peritrochanteric, and 820.8 and 820.9 for unspecified hip fractures) was generated. 20 We excluded patients who were younger than 50 years, had concurrent major trauma, or were transferred to another acute care hospital. 21 Among these patients, only those who underwent subsequent open reduction and internal fixation (ICD-9-CM codes 78.55, 79.15, 79.25, 79.35), total hip arthroplasty (81.51), or hemiarthroplasty (81.52) were included for further analysis. 22 To characterize the association of multiple myeloma with in-hospital outcomes, we identified patients with a diagnosis of multiple myeloma (ICD-9-CM 203.0x). 23
Demographic variables included age, sex, race/ethnicity (white, black, Hispanic, other, unknown), and primary health insurance (private, Medicare, Medicaid, other). On the basis of clinical plausibility and available evidence, we selected several comorbidities that are prevalent in elderly patients with chronic pain that could potentially act as confounders in the associations between multiple myeloma and postoperative outcomes: congestive heart failure, chronic lung disease, liver disease, renal failure, peripheral vascular disease, diabetes mellitus, depression, psychosis, opioid abuse, and alcohol abuse.
By use of ICD-9-CM diagnosis codes, we decided a priori to consider the following major in-hospital adverse events due to their incidence and impact in the perioperative hip fracture surgery setting 20,24 : pneumonia (481, 482.x, 483.x, 484.x, 485, 486, 997.31, 997.39), acute renal failure (584.x), surgical site infection (998.3, 998.5), pulmonary embolism (415.1, 415.11, 415.13, 415.19), deep venous thrombosis (DVT; 451.11, 451.19, 451.2, 451.81, 451.9, 453.40-2, 453.8-9), respiratory failure (518.4, 518.5, 514), myocardial infarction (410.xx), and sepsis (995.91, 995.92).
Statistical Analysis
We constructed multivariable logistic regression models to characterize the association of multiple myeloma with in-hospital mortality and adverse events. All covariates (baseline demographics, comorbidities, procedure type, and hospital characteristics) were defined a priori and entered into the models simultaneously, without further selection. 24 Variables with more than 5% missing values were assigned a missing indicator level. 25 Results were reported as odds ratios (ORs) with 95% confidence intervals (CIs). Statistical tests were 2 sided with P < .05 indicating statistical significance.
Results
Among 2 440 513 patients older than 50 years with surgically treated hip fractures, 4011 (0.2%) were identified as having multiple myeloma. Patients with multiple myeloma were more likely (P < .001) than patients without multiple myeloma to be younger (77.9 vs 80.7 years), male (40.9% vs 27.4%), and black (7.6% vs 2.9%). Patients with multiple myeloma were also more likely to undergo open reduction and internal fixation (63.7% vs 61.5%) and to be treated in urban teaching hospitals (Table 1).
Characteristics of the Study Population (NIS 2002-2011).
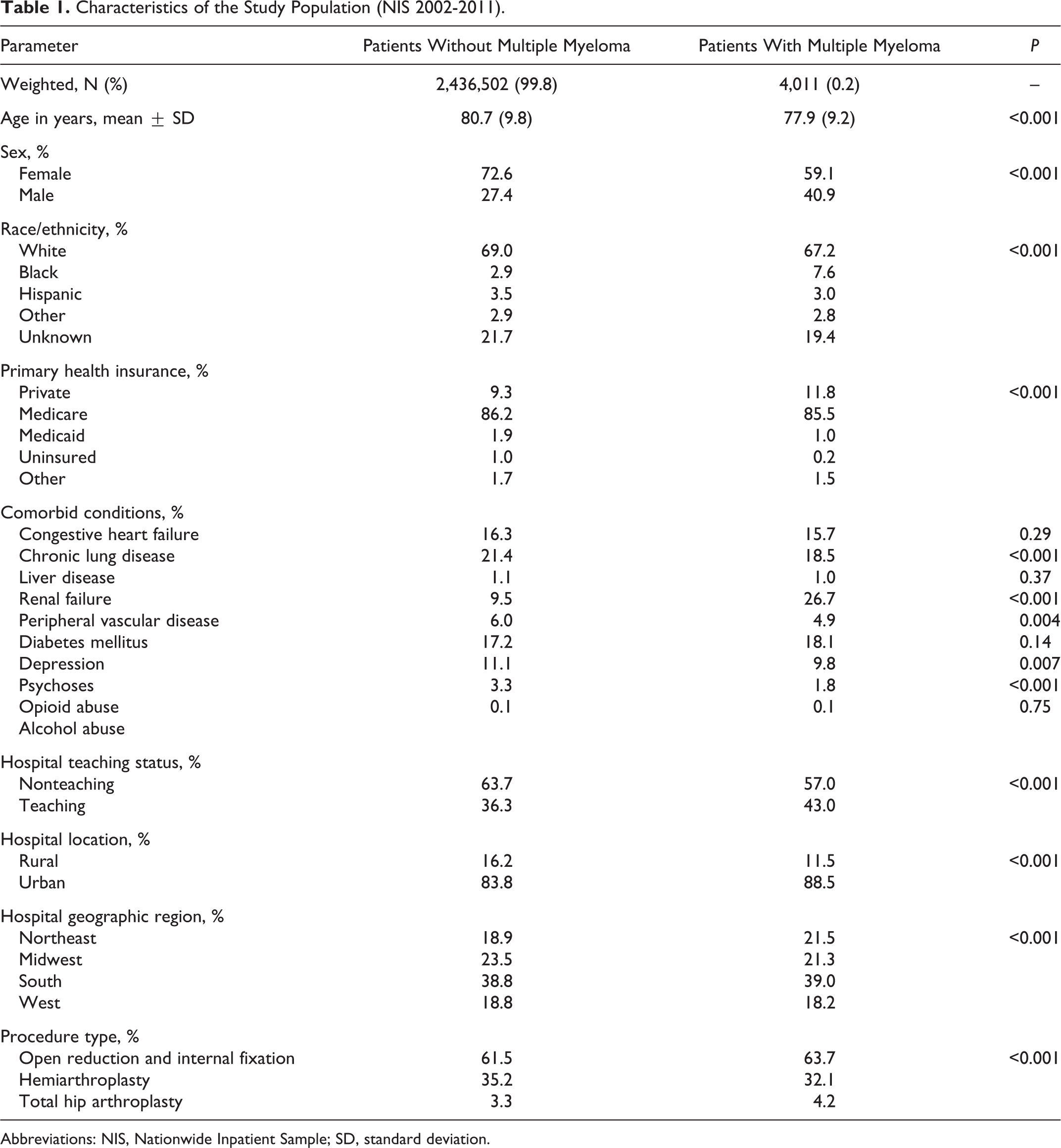
Abbreviations: NIS, Nationwide Inpatient Sample; SD, standard deviation.
After adjusting for demographics, comorbidities, procedure type, and hospital characteristics in multivariable modeling, a diagnosis of multiple myeloma was associated with a higher risk of in-hospital pneumonia (OR: 1.31, 95% CI: 1.14-1.51), sepsis (OR: 1.72, 95% CI: 1.32-2.25), surgical site infection (OR: 1.66, 95% CI: 1.38-2.00), and acute renal failure (OR: 1.28, 95% CI: 1.14-1.43; Figure 1). We found no association of multiple myeloma with inpatient mortality, DVT, and respiratory failure. Multiple myeloma was associated with a lower risk of acute myocardial infarction (OR: 0.69, 95% CI: 0.53-0.90) and pulmonary embolism (OR: 0.45, 95% CI: 0.25-0.83).

Comparison of major in-hospital adverse events between patients with multiple myeloma and patients without multiple myeloma
Discussion
Literature is limited on demographic data and outcomes of patients with multiple myeloma who are undergoing surgical treatment for hip fractures, and in this large Nationwide Inpatient Sample study, 4011 (0.2%) of 2 440 513 patients older than 50 years had diagnosis of multiple myeloma, which was consistent with reported epidemiologic studies of multiple myeloma in this population. 1 –3,26
Our study reports that these patients were more likely to be men, young, and black (P < .001), and these data are in agreement with previously reported demographic data of patients with multiple myeloma. 1,18 They were more likely to undergo internal fixation than arthroplasty in urban teaching centers, and our study findings of younger patients undergoing internal fixation for proximal femur fractures are consistent with previously reported findings. 21,27,28
Due to the immunosuppression associated with the disease and immunosuppressive therapies, patients with myeloma are at increased risk for infection. 1,8,17 This may provide an explanation for our findings that patients with myeloma had significantly higher surgical site infection than its matched cohort in our study. Renal insufficiency is one of the hallmarks of the disease and a diagnostic criterion for symptomatic myeloma. 1,3,7,17 Twenty-seven percent of the patients with multiple myeloma were previously diagnosed with renal failure in our study, and this likely contributed to a significantly number of patients with myeloma developing acute renal failure after hip fracture surgery.
Nonmyeloma patients had higher association with chronic lung disease (see Table 1), however, we were surprised to find that patients with myeloma were at increased risk of developing in-hospital pneumonia. One possible explanation is that a higher number of patients with myeloma were treated with internal fixation rather than arthroplasty, and this may have complicated immediate weight bearing or early immobilization protocol. 27,29 We found no association of multiple myeloma with inpatient mortality and respiratory failure.
Previous studies have shown that patients with malignant disease are at higher risk for thromboembolic events with a prevalence of 7% to 26%. 1,10,13,30,31 In our study, we found that the risk of thromboembolic events was not statistically different between the patients with multiple myeloma and the nonmyeloma patients. It is unclear why the incidence of pulmonary embolism was actually less in myeloma population. This may have been due to increased awareness and emphasis in DVT prophylaxis in urban teaching centers where most of the patients with myeloma were treated (see Table 1).
Our study showed no differences in in-hospital mortality between the 2 groups. We do not know the exact surgical procedures performed in the multiple myeloma cases; but long-stem hip implants are often required for arthroplasty, and long intramedullary nails are needed to protect the entire bone from other lytic lesions. 9 –11 The risk of intraoperative hypotension and potential death has been previously reported to be higher with these longer devices. 10,12,13 However, this did not translate into higher mortality rates in our study, which is in agreement with a recent report. 32
One limitation of this study is that the analysis of information was originally intended for billing purposes. The data from the NIS are limited to diagnoses recorded during the patient’s hospital stay and do not adequately provide information on functional or postdischarge outcomes, such as readmission rates and deep infections. Another limitation of this study is that we were unable to assess the timing to surgery, the complexity of the cases, presence of bone lesions near the joint, and types of surgical devices used. In addition, as in all claims-based studies, coding misclassification may occur. 33 –35
In conclusion, we found that the patients with multiple myeloma are at higher risk for hospital-acquired pneumonia, sepsis, surgical site infection, and acute renal failure than hip fracture patients without multiple myeloma. We found no evidence of higher inpatient mortality rates. Our study findings emphasize the importance of medical care in the perioperative period in order to decrease the risks of common perioperative problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mears: editorial board (Geriatric Orthopaedic Surgery and Rehabilitation), board member (International Geriatric Fracture Society).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Barnes: royalties (DJO, Zimmer), consultant (DJO, Zimmer), stock (Liventa), research support (Liventa), editorial board (JSOA, CORR, JOA), board member (AAHKS, SOA, MAOA, AR Ortho society HKA foundation).