
Abstract
Background/Purpose
The high prevalence of hypovitaminosis D among trauma patients have been related to risk of fractures, falls, non-union and poor operative outcomes. There is limited evidence that ties up Vitamin D levels with fracture severity. The objective of this study is to determine the association of pre-operative Vitamin D levels and fracture severity.
Methods
This was a retrospective, cross-sectional study of patients with extremity fractures classified according to the AO Trauma classification system with baseline pre-operative vitamin D levels. The association between vitamin D levels and fracture severity of surgically treated trauma patients were analyzed. Sub-group analysis was performed on patients without osteoporosis and those patients who suffered from low-energy trauma.
Results
Ninety-six (96) patients were included. Those with severe fractures (AO -C fractures, 31B1.3/B2.3 and 31A3) were associated with lower Vitamin D levels (µ = 17.87 µg/mL) (p < 0.001). There was a strong, positive significant correlation (rs (4) = .426, p = < 0.001) between hypovitaminosis D and increasing fracture severity. This significant association of hypovitaminosis D with worse fracture patterns remains in the patient sub-group without osteoporosis (p = 0.030), and in those who sustained low-mechanism injuries (p < 0.001).
Conclusion
We present initial evidence that low pre-operative Vitamin D level is associated with increasing fracture severity at the time of injury. Early detection, surveillance and management of low vitamin D levels can lead to drastic changes in the holistic approach to fracture prevention and treatment.
Introduction
Calcitriol acts on numerous physiologic pathways related to calcium absorption, regulation of parathyroid hormone and mineralization of osteoid. Well-studied factors that affect Vitamin D levels in the body include altitude, climate and sun exposure practices such excessive use of sunblock, diets low in dairy products and race/ethnicity.1,2 Multiple studies have observed that Hypovitaminosis D is under reported. 3 Similarly, Hypovitaminosis D among Southeast Asians may have been overlooked and underestimated mainly because of the existing temperate climate 1 and in turn may affect how clinicians approach these patients. It is common to encounter asymptomatic patients with Vitamin D deficiency – if left untreated, may lead to worsening osteoporosis, osteomalacia, muscle weakness predisposing to falls and injuries, nonspecific backache and generalized body ache.
There have been multiple studies linking Vitamin D deficiency with increased risk of fractures4–6 and non-union, 3 making it an important variable to consider in the course of management.
In a study involving pre-operative patients, 43% had insufficient serum vitamin D levels, and this number increased to 66% in patients being operated for trauma. 7 Vitamin D status at the time of injury affects fracture healing, 3 increases callus volume 8 and improves posterolateral fusion rates in an in vivo study done among rats. 9 Conversely, a study in 2017 showed that despite a high rate of Hypovitaminosis D (88%) in their population of patients with long bone fractures, the overall non-union rate was low (4%), suggesting conflicting reports on the significance of Vitamin D. There are limited reports on the relationship of hypovitaminosis D with fracture severity. Larrosa et al. in 2011 showed that among elderly patients above 65, severe vitamin D deficiency seems to be associated with severe osteoporotic hip fractures. 10 A prospective, non-randomized study of pediatric patients with low-energy forearm fractures was performed by Hosseinzadeh et al. They concluded that Vitamin D deficiency and insufficiency are common in children with low energy forearm fractures, especially in obese children and in fractures requiring surgical treatment. 11 To date, we are not aware of any local study that described the association of Hypovitaminosis D among orthopedic trauma patients with their fracture severity.
The primary objective of this study is to determine the association of pre-operative level of Vitamin D and the fracture severity among adult trauma in-patients at a tertiary hospital. This study also presented an opportunity to determine the risk factors of increased fracture severity among our patient population. We also looked into those patients with adequate follow-ups and identified the rate of union in our population. We hypothesize that, patients with existing hypovitaminosis D at the time of injury present with a more severe fracture.
Methods
Study design
This was a retrospective, cross sectional, analytical study, utilizing chart/records review. Our study was approved by the local Institutional Review Board and Ethics Committee. We included all patients with pre-operative serum Vitamin D levels who underwent operative treatment for extremity fractures at St Luke's Medical Center-Quezon City from January 2016 to February 2020. Patients were included in this study if: (1) they are seen and diagnosed with a closed extremity fracture confirmed by two orthogonal view radiographs, (2) serum Vitamin D levels taken pre-operatively within 3 weeks of injury until immediately post-surgery, (3) they are stratified as low to intermediate risk for perioperative medical complications prior to the surgical procedure, (4) complete radiographic data uploaded in the local Carestream Vue Motion (PACS) system, and (5) if they had a minimum follow-up of 9 months or until fracture union has been documented. Exclusion criteria included: (1) open fractures, (2) pathologic fractures secondary to metastatic bone disease, (3) Metabolic or endocrine disease affecting calcium and vitamin D metabolism, (4) revision cases, (5) presence of active infection or chronic osteomyelitis, (6) degenerative joint disease adjacent to the fractured region, and (7) Chronic immunosuppressive conditions. Fellowship-trained, board-certified orthopedic surgeons performed all surgeries. Baseline demographic data was obtained as well as previous diagnosis of osteoporosis, smoking status, history of Diabetes mellitus and any previous systemic steroid intake. This study followed the STROBE criteria for quantitative studies. 12
Fracture severity and vitamin D levels
Upon admission of these trauma cases, an initial AO classification is assigned. This was later confirmed by the attending consultant after the index surgery. The AO classification provides a description of fracture patterns in increasing severity, based on the energy of injury or the potential complexity of the recommended treatment. The fractures included in the study were grouped into three anatomic categories: Long bone, femoral neck and pertrochanteric region fractures. Long bone fractures are further divided into A (simple diaphyseal fractures/extraarticular fractures), B (wedge diaphyseal fractures/partial articular fractures) and C (multifragmentary diaphyseal fractures/complete articular fractures) type fractures. Femoral neck (31B) fractures are divided to B1.1/B2.1 (subcapital – valgus impacted/transcervical – simple), B1.2/B2.2 (subcapital – undisplaced/transcervical – multifragmentary) and B1.3/B2.3 (subcapital – displaced/ Transcervical, shear) fractures. Trochanteric region (31A) fractures are divided to A1 (simple pertrochanteric), A2 (multifragmentary pertrochanteric, incompetent lateral wall) and A3 (intertrochanteric/reverse obliquity) fractures. For the statistical analysis, fractures were grouped as mild (long bone A fractures, femoral neck B1.1/B2.1, pertrochanteric A1), moderate (long bone B, femoral neck B1.2/B21, pertrochanteric A2) and severe (long bone C, femoral neck B1.3/B2.3, pertrochanteric A3).
Patients were categorized as having vitamin D deficiency (<20 µg/ml), vitamin D insufficiency (≥20–29.9 µg/ml), or normal vitamin D levels (>30 µg/ml), following the 2011 American Endocrine Society guidelines. 1 We only recorded the final AO classification. Treatment for Vitamin D with oral supplementation was started as soon as the diagnosis is established. Effects of vitamin D supplementation in our trauma population was outside the scope of this study.
Clinical union was assessed by the attending surgeon by checking for tenderness and motion at the fracture site and pain on weight bearing of the affected extremity. 13 An independent, blinded, board-certified radiologist determined radiographic union, which is defined as the presence of bridging callus across at least three of four cortices or two of four cortices with a stable implant from at least two orthogonal views of the affected extremity on follow-up radiographs. If discrepancies between clinical and radiographic union existed, the clinical assessment of union was preferred. 13 Nonunion was diagnosed once patients did not meet the criteria for clinical or radiographic union, did not have union after 9 months of follow-up, and was indicated or has already underwent re-operation for a diagnosis of a nonunion. Follow-up data were obtained from the surgeon's clinics from the patients’ post-operative visits.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics (Arrmonk, NY, USA). Chi-square test for association was done to determine association between Hypovitaminosis D and fracture severity for the entire population. Fisher's exact test was used in the analysis of sub-groups with confounding risk factors identified in the study, if the sub-group population was less than 67. Spearman rank-order correlation was performed on the variables to measure the strength and direction of association that exists between the groups. Descriptive statistics were used to describe the study population. Level of significance was set at p < 0.05 for all analyses conducted.
Results
Patient characteristics
117 patients were included in the study. Twelve patients with pathologic fractures were excluded. Four patients were excluded due to known thyroid/parathyroid disorders; Five patients were further excluded due to serum Vitamin D taken more than 3 weeks from injury. We included 96 patients in our final population. Eight of these patients had 2 fractures on different sites. For these patients, their fractures were treated as individual fractures. Table 1 summarizes the clinical and demographic characteristics of these patients.
Clinical and demographic characteristics of participants.
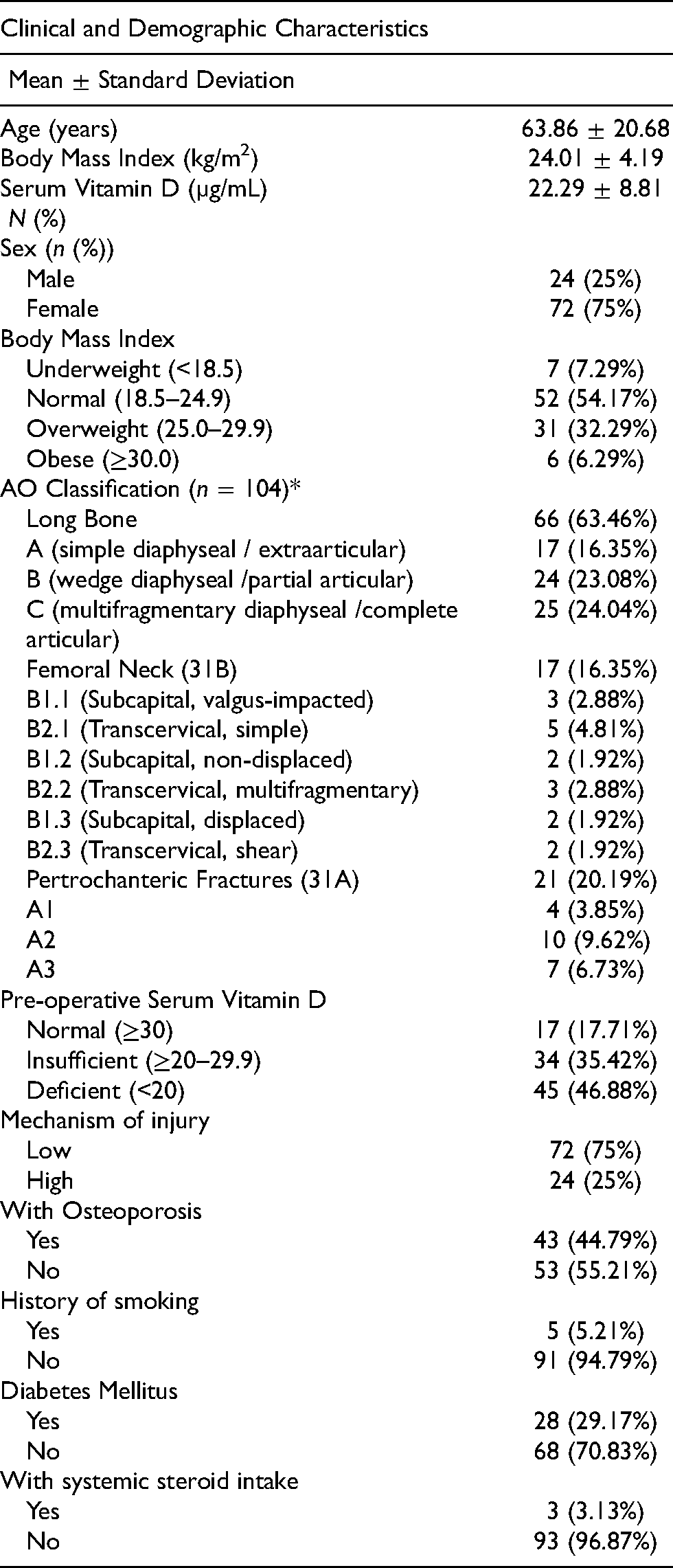
79 patients (82.30%) had hypovitaminosis D, and the majority of these are Vitamin D deficient (45/79, 56.98%). Majority of our patients are females and only 6 (6.29%) are obese. 66 (63.46%) patients comprise majority of the documented fractures under the long bone category. Majority (75%) of our population sustained a low energy mechanism injury. Low mechanism injury is defined as forces equivalent to a fall from a standing height or less. 14 43 (44.79%) patients were labelled as osteoporotic because of a previous diagnosis with bone densitometry, ongoing treatment, previous or current fragility fracture.
Figure 1 shows the Vitamin D status for each fracture under their corresponding AO classification. There is a significant relationship between increasing fracture severity and Hypovitaminosis D (X2 (4, N = 104) = 20.6, p < .001). Patients presenting with more severe fractures showed lower levels of Vitamin D and higher prevalence of hypovitaminosis D compared with patients with less severe fractures. Spearman's correlation was run, which showed a strong positive correlation between Hypovitaminosis D and increasing fracture severity, which was statistically significant (rs (4) = .426, p = < 001). Serum Vitamin D levels for each fracture severity category was graphically represented in Figure 2. Majority of the population had sub-optimal Vitamin D levels, and it was observed that the trend of their measured Vitamin D levels decrease with worsening fracture severity. Measured serum Vitamin D for patients who presented with severe fracture patterns were lower than the moderate and mild group.
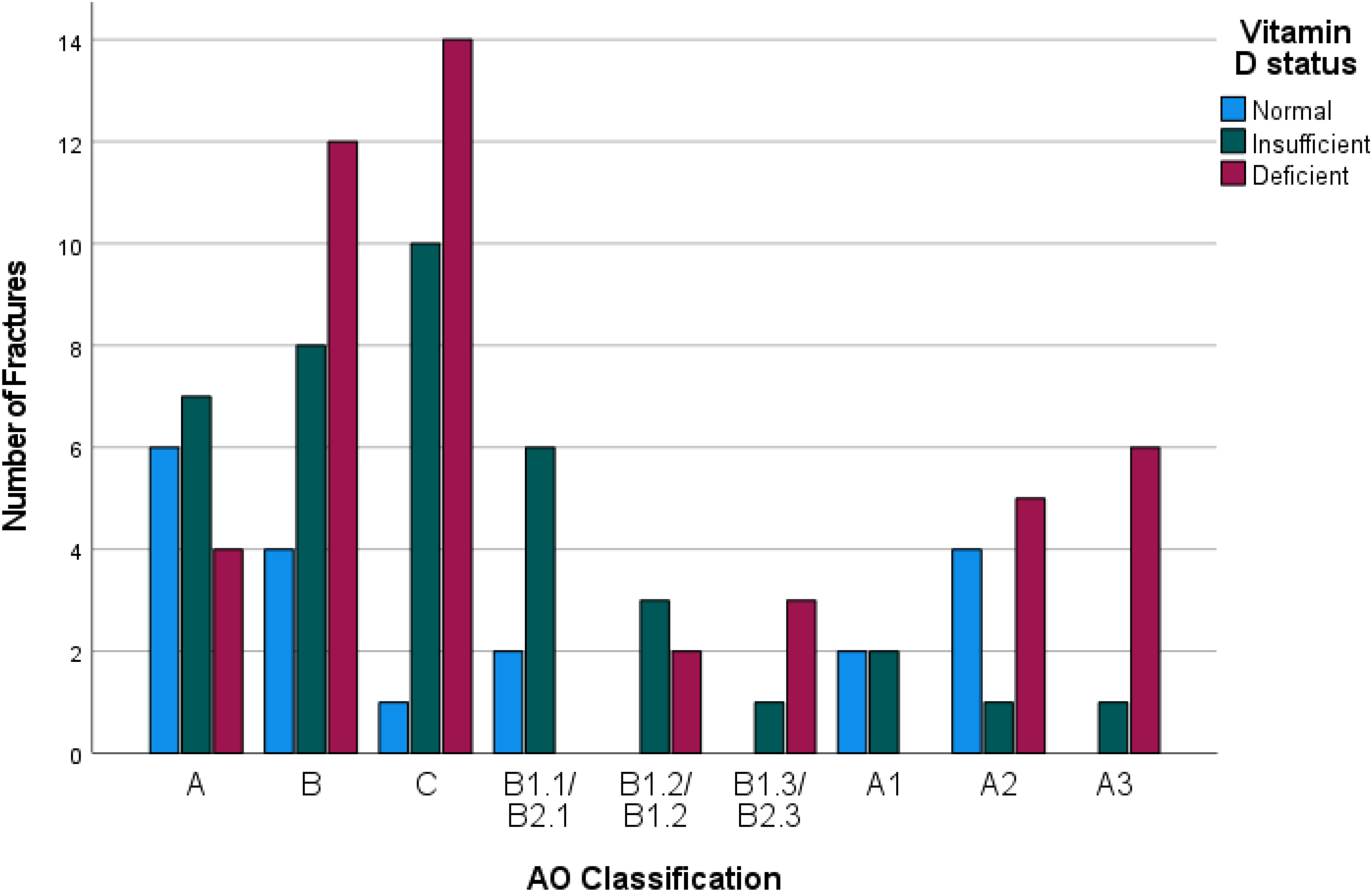
Vitamin D Status per AO classification.
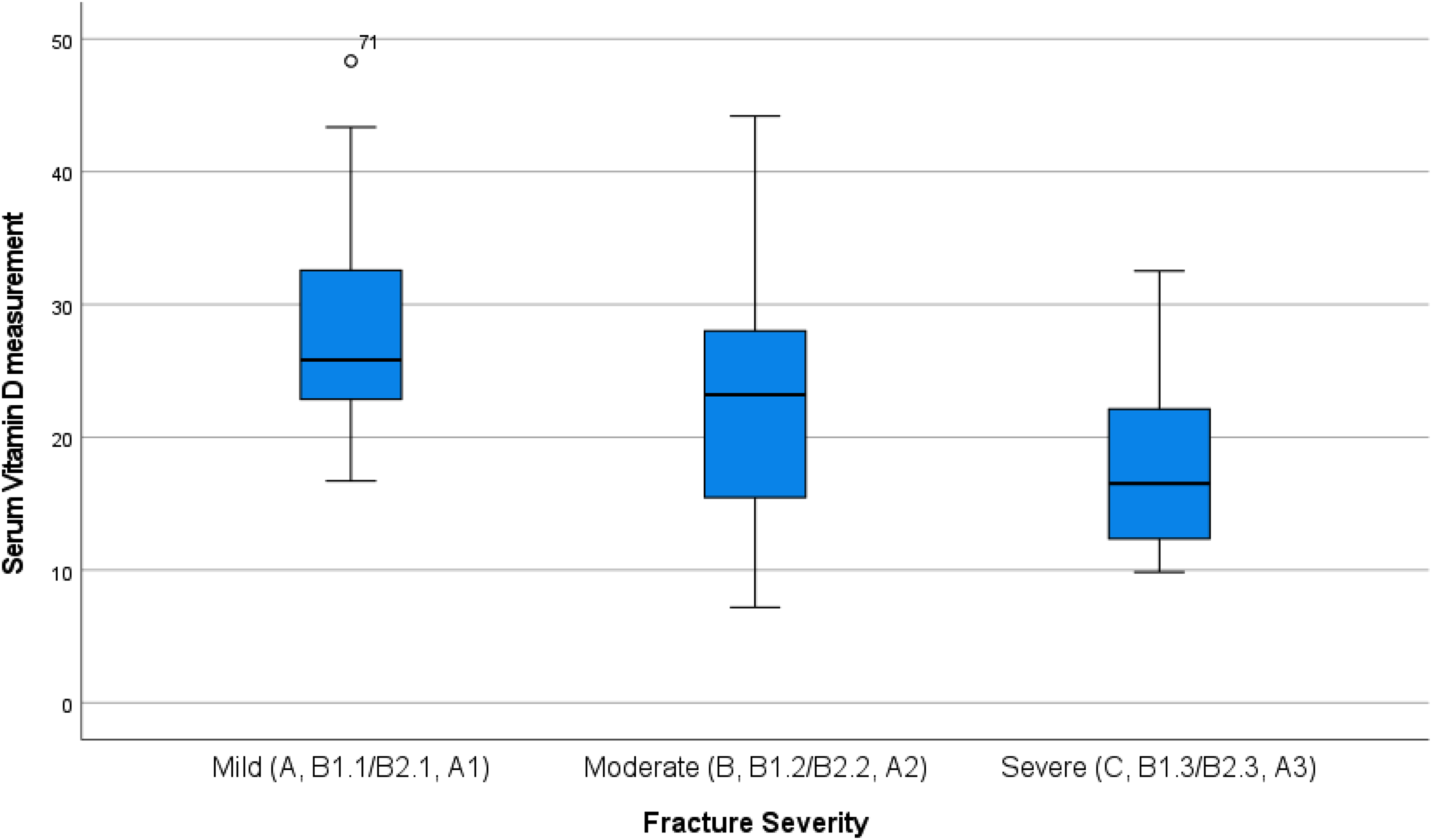
Measured Serum vitamin D levels per assigned fracture severity group.
Figure 3 shows the breakdown of non-osteoporotic fractures according to Vitamin D status. Among these patients, the frequency of vitamin D deficiency increased together with fracture severity. Based on these results, Fisher's test indicate that there was a significant association between Hypovitaminosis D and increasing fracture severity (Χ2(4, N = 48) = 10.69, p = .030). A Spearman's correlation was run, which showed in a moderate association between Hypovitaminosis D and increasing fracture severity, which was statistically significant (rs (4) = .311, p = .011). For those with osteoporosis at time of injury, there was no significant association with vitamin D levels and fracture severity (Χ2(4, N = 66) = 8.67, p = .070).
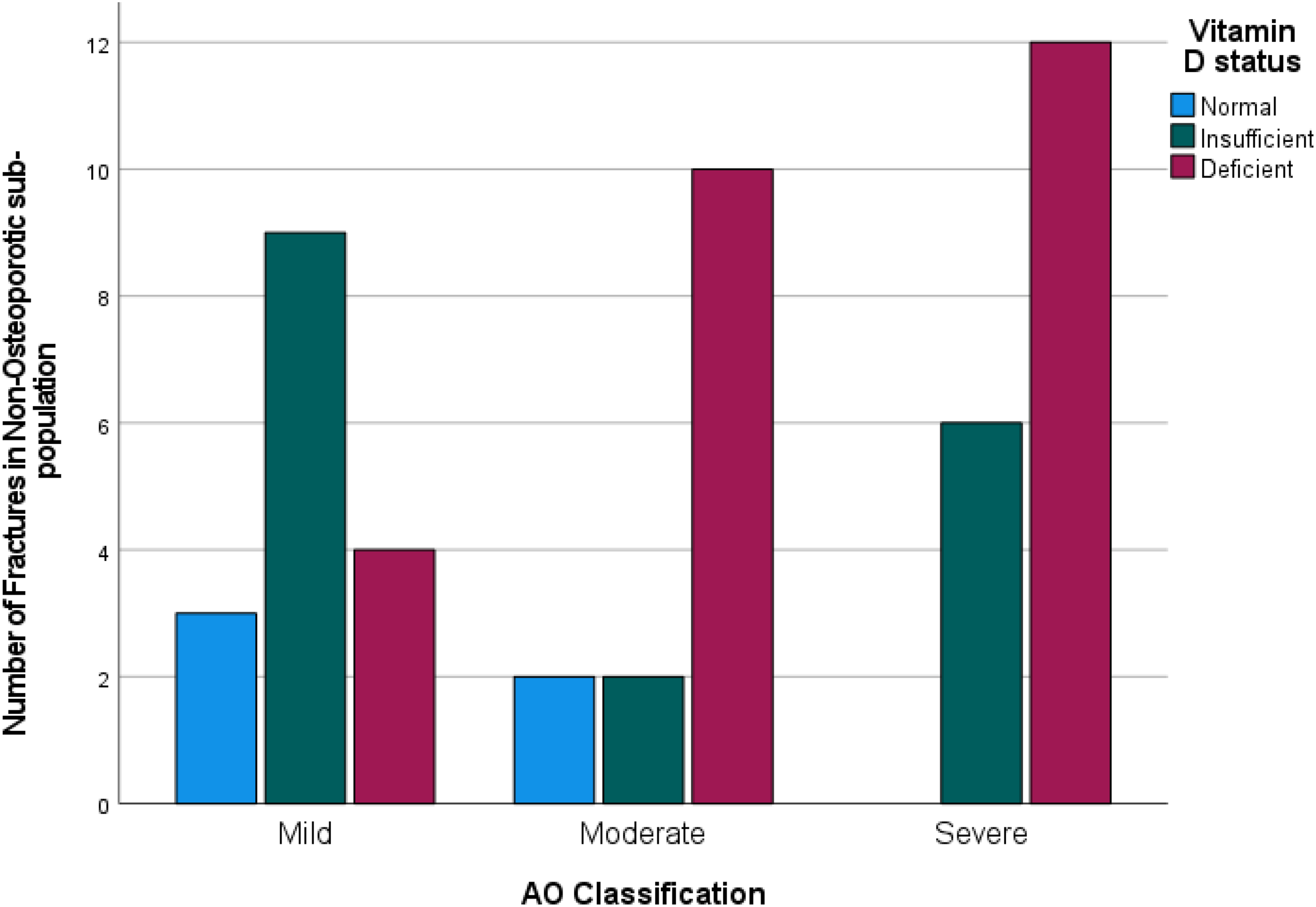
Vitamin D Status per assigned fracture severity group, non-osteoporotic population.
Figure 4 shows the breakdown of fractures sustained from a low-energy mechanism according to Vitamin D status. In this sub-group, there was a trend of increasing fracture severity with worsening vitamin D status. There was a significant association between Hypovitaminosis D and increasing fracture severity (Χ2(4, N = 76) = 22.97, p < .001) in this group. Spearman's correlation showed a strong positive correlation between hypovitaminosis D and worsening fracture severity, which was statistically significant (rs = .542, p < .001). In a smaller sub-group of patients who had high-energy injury, there was no significant association with fracture severity and vitamin D levels (Χ2(4, N = 28) = 4.461, p = .320).
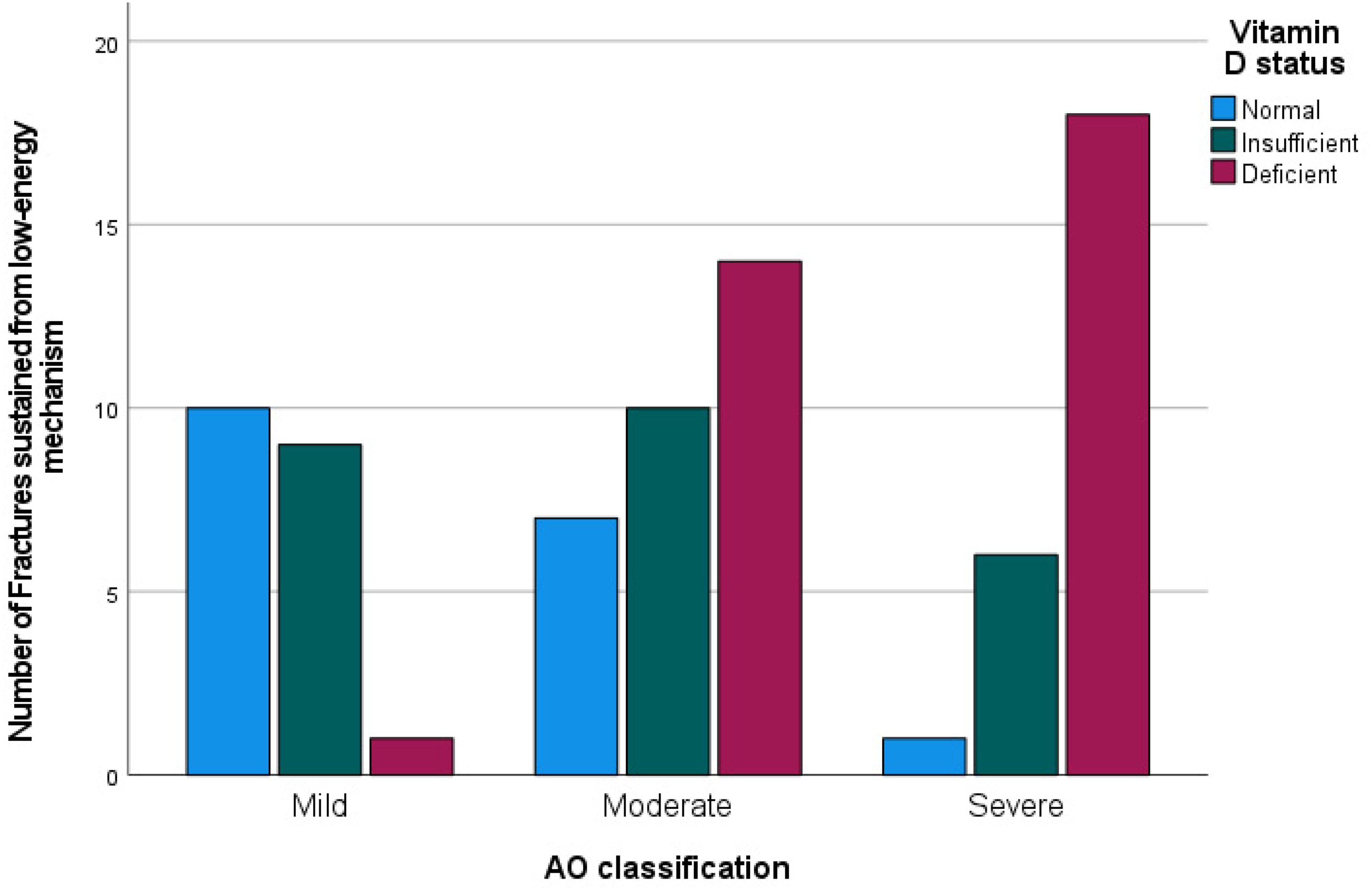
Vitamin D Status per assigned fracture severity group, low-energy mechanism population.
Thirteen patients had incomplete follow-up data. Out of the 83 patients followed-up, 1 patient was treated for non-union and 1 case was labelled as delayed union. The non-union case was a 21 year old female who sustained a closed 32A2 fracture with severe Vitamin D deficiency (7.2 µg/mL). Her latest follow-up radiographs and CT scan at 11 months show persistence of the fracture line with pain on weight bearing. She is yet to be treated with a revision surgery for nonunion at the time of writing. The delayed union case was a 62 year old male, non-osteoporotic, with a closed 44C1 fracture with Vitamin D insufficiency (15.85 µg/mL). He had pain on weight bearing and tenderness over the fracture until 6 months post-op and the fracture line was apparent on radiographs until 11 months post-operatively. Excluding 13 patients who underwent arthroplasty, the union rate for our population is 97.14%.
Discussion
There are many factors that can influence fracture severity, including intrinsic factors of the bone at the time of injury, the specific bone involved, genetic factors, nutrition and balance. 11 In summary, our population is mainly Asian, with a mean age of 63 years old with normal BMI, living in a tropical climate with undocumented sun exposure status/sunscreen use and an unknown percentage of patients who take Vitamin D supplementation at the time of injury.
The optimal level of serum vitamin D is controversial. The 2011 American Endocrine Society guidelines is popular among others because histological markers have identified evidence to suggest that there is indeed a significant difference in bone quality between a vitamin D level of 20 and 30 µg/mL. 15 Mass spectroscopy systems are currently favored as the standard, however, due to logistic sophistication, immunoassays are more commonly available and are still accepted. 16 In our institution, serum 25 (OH) vitamin D is obtained via direct chemiluminescent technology/competitive immunoassay using the Siemens ® Adavia Centaur XPT System. 25 (OH) vitamin D is the major circulating form of vitamin D, with a circulating half-life of 2–3 weeks, and it is the best indicator to monitor for vitamin D status. 17
The prevalence of hypovitaminosis D has been established in several orthopaedic populations. Particularly, the high prevalence of hypovitaminosis D among trauma patients, as high as 82% in some reports, holds true in our population.7,18–20. Vitamin D has a direct effect on bone mineralization21 and Vitamin D-specific receptors are seen in high numbers on fast-twitch muscle fibers, which are the first to respond in a fall. 22 Hence, low vitamin D levels, especially those of <9 µg/mL, have been associated with osteomalacia, impaired muscle function, poor neuromuscular control, decreased bone mineral density and increased fracture risk.6,7,23,24 However, there is a scarcity of data describing the effect of low vitamin D levels on fracture severity. Our study was able to find a significant association between low vitamin D levels and increasing fracture severity, supporting previous claims that low vitamin D levels is indeed clinically important.3,10,11
Our results showed a moderate association between low vitamin D and increasing fracture severity among those without osteoporosis, whereas no association was found among those patients with osteoporosis. This underscores the importance of vitamin D in the absence of osteoporosis. This could mean that treating hypovitaminosis D among non-osteoporotic patients may decrease risk of sustaining severe fracture patterns. These younger patients are those at highest risk for low vitamin D levels secondary to lifestyle changes leading to decreased sun-exposure.15, 18 Meanwhile, low prevalence of hypovitaminosis D among osteoporotic patients is not surprising, as many of these patients have an established diagnosis of osteoporosis and likely have been managed with calcium and vitamin-D supplementation prior to injury. 7 In addition, there was a strong, statistically significant correlation between hypovitaminosis D and worsening fracture severity among those suffering from low-energy injuries, while there was no association established among those suffering from high-energy mechanism injuries. The authors have a shared experience of having encountered young adults with complex fracture patterns secondary to low-mechanism injuries. Our results provide preliminary data that complex fracture patterns can result from even low-energy trauma on the background of low vitamin D. We theorize that this is one of the more important subgroups to investigate in future studies.
Should our results be corroborated by future studies involving a larger population, a drastic change in the approach to fracture prevention and treatment may be warranted, with the focus shifting to ameliorating the risk of sustaining severe fractures. This begins by increasing awareness among individuals to encourage sunlight exposure, which has been proven to increase vitamin D levels. 24 A survey of over 400 orthopedic trauma surgeons done last 2016 showed that 65.8% of surgeons routinely prescribe vitamin D to fragility fracture patients and 25.7% routinely prescribe vitamin D to non-fragility fracture patients. This study identified considerable variability in treatment regimens for both fragility fracture patients and non-fragility fracture patients.25 There is great potential for intervention, if it can be proven that a specific protocol of vitamin D supplementation can decrease the risk of sustaining more severe fractures because despite the presence of various treatment protocols, vitamin D supplementation is generally ascribed as cost-efficient and safe.13,26
There is a high union rate observed in our population. Causality has not been established between Vitamin D status and non-union, owing to difficulty in controlling numerous risk factors that play a role in union.3,13 Determining the effects of vitamin D levels on fracture union was outside the scope of our study. It is also possible that the current threshold for vitamin D deficiency and insufficiency is not clinically relevant to fracture healing 7 or that high union rates may be independent of supplementation.27
There are several limitations and potential biases in our study. There is no independent interpretation of the injury radiographs to classify the fractures. Likewise, there was no separate comparison done between the initial AO classification assigned upon admission and the final AO classification made post-operatively. In addition, the attending surgeon was not blinded to the Vitamin D status of the patient. Another limitation of our study is the small sample size. Inherent to purposive sampling is selection bias and prevalence-incidence bias. Since our population involved patients who were surgically treated, the population may be skewed towards more severe fracture patterns. Determination of Vitamin D status is not a standard practice in our institution, hence the currently tested population represents a fraction of the entire group of interest Subsequent research should equally sample both non-surgically and surgically treated fractures. A randomized block design for prospective studies or matched patient selection in retrospective studies with large enough sample size to allow for sub-group analyses is recommended for future studies. Finally, the magnitude of percent deficiency from the normal level to have clinically significant effects on fracture severity remains to be unknown.
Our study provided preliminary evidence that an important association between low Vitamin D levels and increasing fracture severity exists. Our results should raise awareness among orthopedic surgeons about hypovitaminosis D. Prospective studies with better population recruitment or retrospective studies utilizing propensity matching techniques can eliminate possible confounding factors that can have an effect on fracture severity in relation to Vitamin D levels, such as obesity, smoking status and steroid intake. Additional studies can look into the benefit of early detection and determine a clinically relevant treatment protocol for the treatment of hypovitaminosis D in relation to fracture prevention.28
Conclusion
Serum vitamin D levels were significantly associated with the severity of fracture as described in the AO classification (p < 0.001). This association was also seen in the sub-group of patients who are not osteoporotic (p < 0.030) and those whose injuries were secondary to a low-energy mechanism (p < 0.001). Hypovitaminosis D predisposes orthopedic trauma patients to worse fracture patterns. Given that treatment of low vitamin D levels is through oral supplementation, authors recommend that hypovitaminosis D be treated to decrease risk of developing severe traumatic fractures.
Footnotes
Acknowledgements
Irwin O. Sarmiento, MD, FPCR for participating in determining radiologic outcomes of the patients.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.